Humanity and Human Relationships: A Philosophical and Social Exploration
Humanity and Human Relationships: A Philosophical and Social Exploration
Riya Singhal *1; Varsha Ojha 2
1) Riya Singhal, Deira International School.
2) Varsha Ojha, Consultant OBGYN, Prime Hospital, Dubai.
*Correspondence to: Riya Singhal, Deira International School.
Copyright
© 2025 Riya Singhal. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 12 May 2025
Published: 15 May 2025
DOI:https://doi.org/10.5281/zenodo.15681360
Abstract
This article explores the intricate relationship between humanity and human relationships, delving into the philosophical, psychological, and sociological dimensions that define and shape our shared existence. It examines how the essence of humanity is expressed through empathy, compassion, moral responsibility, and the need for connection. Human relationships spanning familial, social, romantic, and professional spheres are not only vital to individual well-being but also fundamental to the progress and sustainability of societies.
Humanity and Human Relationships: A Philosophical and Social Exploration
1. Introduction
Humanity is a profound and multifaceted concept that embodies the essential qualities, values, and behaviors which define human existence. At its core, humanity is not solely a biological classification but a deeply philosophical and moral construct. It encompasses compassion, empathy, emotional intelligence, and an inherent sense of ethical responsibility toward others. These attributes are not innate in isolation; rather, they are cultivated and expressed within the dynamic realm of human relationships. The connection between individuals—their interactions, emotional exchanges, and mutual dependencies—form the true framework through which humanity is realized and nurtured.
Human relationships are the living canvas upon which the principles of humanity are painted. From birth to death, individuals are shaped by the emotional and social environments around them. Relationships serve as the conduit for love, understanding, learning, growth, and healing. They influence personality development, shape moral perspectives, and determine emotional resilience. Whether it is the unconditional love found in families, the solidarity of friendships, the intimacy of romantic bonds, or the collaborative spirit of communities, every relationship carries the potential to reflect and reinforce our human values.
Moreover, relationships are not only personal but also deeply social and cultural in nature. They reflect the collective values of societies and the moral fabric of civilizations. The way individuals interact with each other—through kindness or cruelty, cooperation or conflict—often mirrors the state of humanity at large. In times of crisis or social change, it is these relationships that either hold communities together or expose their fragility.
In the context of a rapidly modernizing world, where digital connectivity often overshadows face-to-face interaction, the essence of genuine human relationships is increasingly at risk. Emotional disconnection, loneliness, and reduced interpersonal empathy are becoming prevalent concerns, particularly among younger generations. This shift raises important questions about the future of humanity: Can we preserve the depth of human connection in an age of virtual relationships? Will technological advancement strengthen or weaken the bonds that form the foundation of society?
This article seeks to explore these questions by examining the essence of humanity through the lens of human relationships. It aims to analyze how empathy, trust, and communication underpin these connections, and how modern societal trends are reshaping the way individuals relate to one another. By doing so, it offers insights into how we might reclaim and strengthen our shared humanity in a world that is both increasingly connected and paradoxically divided.
The Nature of Humanity
Humanity encompasses both innate biological instincts and cultivated emotional and ethical traits. At the heart of it is empathy, the ability to understand and share the feelings of another person. Empathy is not only a personal virtue but also the cornerstone of social harmony, allowing people to form deep and meaningful bonds. It gives rise to compassion and moral responsibility, encouraging individuals to act in ways that support the well-being of others. From a biological standpoint, humans are inherently social creatures who rely on cooperation and connection for survival. The structure of early human societies, organized around group living and shared resources, reflects the deep evolutionary need to belong. Over time, this evolved into more complex emotional and ethical relationships, but the foundational need for connection has remained unchanged.
Dimensions of Human Relationships
Human relationships manifest in a variety of forms, each fulfilling unique roles in an individual’s emotional and social life. Familial relationships are typically the first ones we form and are crucial for emotional development. They provide a foundation of trust, security, and identity, shaping how individuals relate to others later in life. Friendships, on the other hand, offer companionship and mutual support outside of family ties. They allow people to share experiences, exchange ideas, and offer emotional relief, especially during times of stress or transition. Romantic and intimate relationships are another dimension, characterized by deeper emotional bonding, vulnerability, and often long-term commitment. These relationships are often a central source of happiness and personal growth, requiring trust, mutual respect, and open communication. In contrast, professional and community-based relationships are formed around shared goals and responsibilities. Though they may not always be emotionally intimate, they are crucial for collaboration, social integration, and societal development.
The Role of Communication and Trust
Communication and trust serve as the foundation for all types of human relationships. Without clear, honest, and empathetic communication, misunderstandings arise, which can lead to conflict and emotional detachment. Trust enables individuals to feel safe and valued in a relationship, while communication ensures that thoughts, feelings, and expectations are understood. Emotional intelligence also plays a significant role in navigating relationships—it allows people to interpret emotional cues, manage conflicts with empathy, and create deeper connections through mindful interaction. Relationships lacking in trust or meaningful communication often deteriorate over time, highlighting the importance of cultivating these qualities intentionally.
Challenges to Human Relationships in the Modern Era
Despite living in an era of global connectivity, many modern social environments have created barriers to authentic human connection. One significant challenge is the growing dependency on digital communication. While technology has enabled people to stay in touch across vast distances, it has also led to superficial interactions, reduced empathy, and feelings of social isolation. This digital paradox—being constantly connected yet emotionally detached—can undermine the depth of real-life relationships. Additionally, the rise in mental health issues such as anxiety, depression, and emotional burnout affects how individuals relate to others. High stress levels, especially from work-related pressures and social comparison, can lead to emotional withdrawal and strained relationships. Cultural and generational shifts also play a role, with evolving norms sometimes weakening traditional values like loyalty, patience, and long-term commitment. While such changes allow for more personal freedom and autonomy, they can also result in less stable and enduring social bonds.
Rebuilding and Nurturing Humanity through Relationships
Reaffirming our humanity requires an intentional investment in building and nurturing human relationships. One important step is to incorporate emotional literacy into education systems. Teaching children and young adults how to understand and manage emotions, resolve conflict, and develop empathy can lead to healthier relationships across all areas of life. Furthermore, encouraging community involvement through volunteerism and service fosters a shared sense of purpose and connection. Such acts reinforce the importance of interdependence and social responsibility. On a personal level, practices like mindfulness and self-reflection can improve the way individuals relate to others. Being present in interactions, recognizing emotional triggers, and practicing compassion can significantly enhance the authenticity and depth of relationships. These practices not only strengthen interpersonal bonds but also contribute to a more empathetic and unified society.
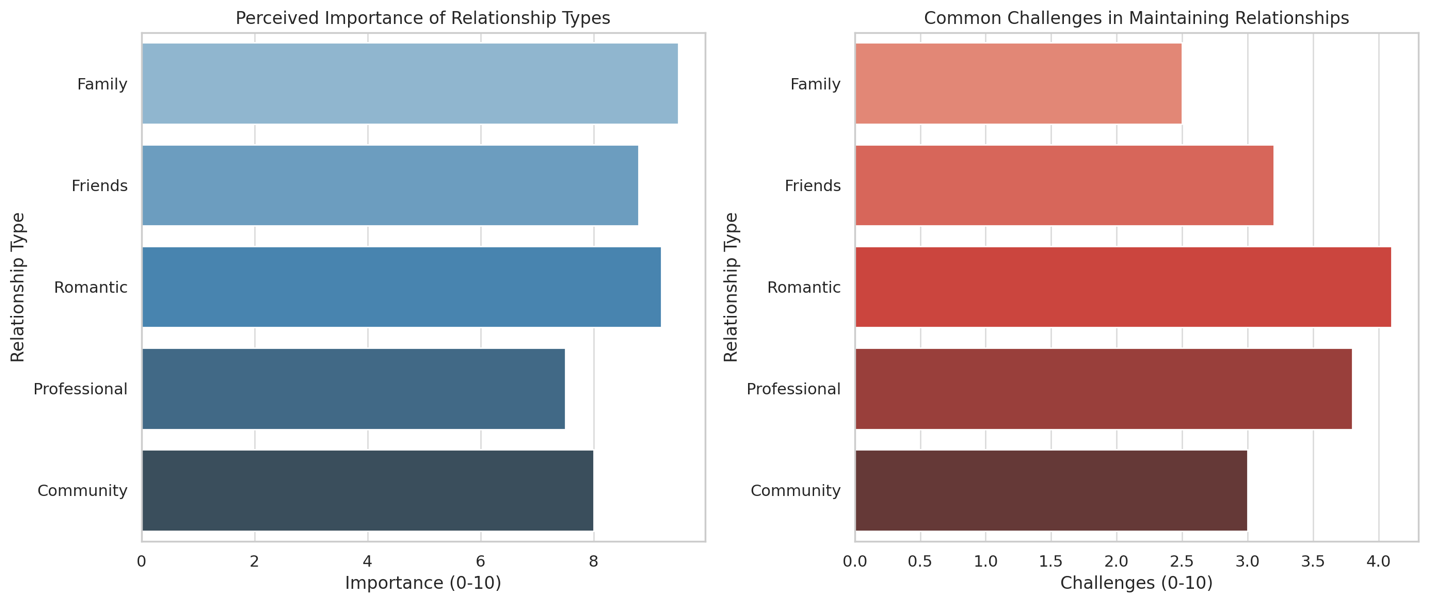
Figure 1
Conclusion
Humanity and human relationships are interdependent forces that sustain individuals and civilizations. In an era where technological and cultural transformations threaten the depth of human connection, it is crucial to revive the essence of humanity through intentional, compassionate, and value-driven relationships. Strengthening these bonds is not merely a personal endeavor but a social imperative that shapes the future of humanity itself.
References
1. Baumeister, R. F., & Leary, M. R. (1995). The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychological Bulletin, 117(3), 497–529.
2. Fromm, E. (1956). The Art of Loving. Harper & Row.
3. Goleman, D. (2006). Social Intelligence: The New Science of Human Relationships. Bantam.
4. Putnam, R. D. (2000). Bowling Alone: The Collapse and Revival of American Community. Simon & Schuster.
5. Turkle, S. (2011). Alone Together: Why We Expect More from Technology and Less from Each Other. Basic Books.