Fatal Cerebral Aneurysm
Fatal Cerebral Aneurysm
Dr. Hassan Jazayeri *
*Correspondence to: Dr. Hassan Jazayeri Neurologist.
Copyright
© 2025 Dr. Hassan Jazayeri, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 May 2025
Published: 31 May 2025
DOI: https://doi.org/10.5281/zenodo.15688150
Abstract
Aneurysm disease, which is a congenital disorder and is usually discovered incidentally during the examination of diseases, can be found in any part of the brain. Given that aneurysm is a structural weakness in the arteries within the brain, the threat of rupture can occur in any situation and put the person on the verge of losing his health, and this is the main threat. Do all aneurysms eventually rupture? The answer to this question cannot be predicted, but finding it in front of the patient can make the medical teams of the patients more alert.
Fatal Cerebral Aneurysm
Introduction
When this 74-year-old male patient was brought to our hospital as an emergency, my colleagues asked me to visit him, given that the patient had neurological symptoms, including speech disorders and severe headaches and dizziness. I had known him closely for many years and he was never a patient who complained of headaches. He did not even have high blood pressure. Or did he have other diseases such as diabetes or heart problems. His main problems were mostly due to multiple lumbar discopathy along with spondylolisthesis, which he had also operated on two years ago and his condition was almost stable. When I found him in the same state of lethargy and speech disorders, along with half-body drowsiness, the first thing I thought about was a stroke. While he was lying on the stretcher and I was about to start the clinical examination, he suddenly took a deep breath and closed his eyes and I was very worried. At first I thought he had gone into a coma. But after a short while, he opened his eyes and asked me: Has something happened? Because I don't remember what happened that I am now on the ambulance stretcher. I, taking the opportunity that he had regained consciousness, tried to make the most of my efforts to take a detailed history and then a clinical examination. To decide where to send him... I had a complete understanding of his medical history and the only thing that came to mind was a stroke or even a transient ischemic attack or TIA. While I was talking to him, I noticed that the patient's eyes were closed and his mouth was open as if he was choking. I called his name out loud and asked what was wrong. But he started snoring and while he had his eyes closed, he tried to vomit and he couldn't. I couldn't even open his mouth because he was so stiff and tense that when I saw that he wasn't showing any reaction or action, I told the ambulance driver and the medical team to move quickly and get him to the hospital and the emergency department as soon as possible. Considering that he had no neurological problems, it was impossible to make a preliminary diagnosis for this patient. At that moment, all I could do was to get him to the emergency room at all costs. To provide him with more specialized care. And when the ambulance arrived, my only concern was whether this patient would reach Nana Teresa Hospital safely. I insisted on the patient's medical team to take him to the emergency room at all costs so that his specialized problem could be followed up as soon as possible. Two hours later, and the patient was placed in the intensive care unit while he was in a deep coma, the first initial reports showed massive bleeding in the brain tissue due to a ruptured cerebral aneurysm. And this was while we had no medical history or document from the patient to confirm this.
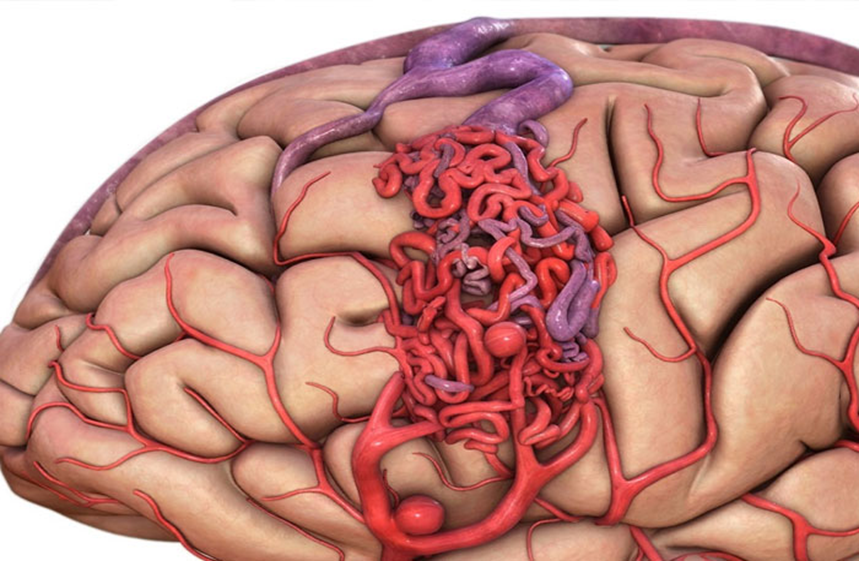
What is a cerebral aneurysm?
A cerebral aneurysm is a weak and prominent area in the wall of an artery in the brain. Sometimes it is also called a "balloon" or "vascular bundle". This weak area can swell under the pressure of blood flow and pose a risk of rupture (burst) and bleeding into the brain.
History:
Brain aneurysms have probably existed since ancient times, but due to the lack of advanced diagnostic methods, their understanding and recognition have been very limited. Sudden deaths or strokes that we now know can be caused by ruptured aneurysms were previously attributed to other causes.
Development of diagnostic methods:
A turning point in the recognition and treatment of brain aneurysms was the development of medical imaging methods:
Cerebral Angiography: The invention of cerebral angiography in the 20th century made it possible to directly observe the blood vessels of the brain and diagnose aneurysms in living people. This method helped doctors identify the location, size, and shape of the aneurysm before it ruptured.
Computed Tomography (CT Scan) and Computed Tomography Angiography (CTA): With the advent of CT scans, the diagnosis of bleeding from ruptured aneurysms became much faster and more accurate. CTA also allows for more detailed visualization of vessels and aneurysms. • Magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA): MRI and MRA are noninvasive procedures that provide very detailed images of brain structures and their vessels and are important in diagnosing unruptured aneurysms and planning treatment.
A cerebral aneurysm is a weak, prominent area in the wall of an artery in the brain. It is sometimes called a "balloon" or "vascular bundle." This weak area can swell under the pressure of blood flow, posing a risk of rupture (bursting) and bleeding into the brain.
History:
Cerebral aneurysms have probably existed since ancient times, but due to the lack of advanced diagnostic methods, their understanding and detection have been very limited. Sudden deaths or strokes that we now know can be caused by aneurysm rupture were previously attributed to other causes.
Development of diagnostic methods:
A turning point in the recognition and treatment of cerebral aneurysms was the development of medical imaging methods:
• Cerebral Angiography: The invention of cerebral angiography in the 20th century made it possible to directly observe the blood vessels of the brain and diagnose aneurysms in living people. This method helped doctors identify the location, size, and shape of the aneurysm before it ruptured.
Computed tomography (CT Scan) and computed tomography angiography (CTA): With the advent of CT scans, the diagnosis of bleeding due to ruptured aneurysms became much faster and more accurate. CTA also allowed for more accurate visualization of vessels and aneurysms.
• Magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA): MRI and MRA are non-invasive methods that provide very detailed images of the structures of the brain and its vessels and play an important role in the diagnosis of unruptured aneurysms and treatment planning.
Advances in treatment methods:
Along with the advances in diagnosis, treatment methods for cerebral aneurysms also evolved:
• Open surgery (Surgical Clipping): The first successful surgical method for closing cerebral aneurysms was developed in the 20th century. In this procedure, the surgeon accesses the aneurysm by opening the skull and blocks blood flow by placing a metal clip around its neck. This procedure remains an effective treatment for many aneurysms.
• Endovascular Treatment: In recent decades, endovascular procedures have emerged as a less invasive alternative to open surgery. Procedures such as coiling (filling the aneurysm with metal wires through a catheter) and stenting (placing a mesh tube in the artery to support it) have revolutionized the treatment of brain aneurysms.
Incidence of Brain Aneurysms:
• It is estimated that about 3 to 5 percent of people will develop a brain aneurysm during their lifetime.
• About 6.7 million people in the United States have an unruptured brain aneurysm, which is about 1 in 50 people.
• The annual rate of aneurysm rupture is about 8 to 10 per 100,000 people.
• About 30,000 cases of brain aneurysm rupture occur in the United States each year.
• Women are more likely to develop brain aneurysms than men (3 to 2 ratio).
• Women are at higher risk of aneurysm rupture than men, especially those over the age of 55.
It is important to see a doctor right away if you experience a sudden, severe headache or other suspicious symptoms. Early diagnosis and treatment can significantly reduce the risk of serious complications from a brain aneurysm.
Prevalence by gender:
• Women are more likely to develop brain aneurysms than men.
• The female-to-male ratio is estimated to be about 1.5 to 1 or 2 to 1.
• Women are also at higher risk of aneurysm rupture than men, especially those over the age of 55.
• The exact reason for this difference is not yet fully understood, but hormonal factors and the structure of the blood vessels may play a role.
In short, women are more likely to develop brain aneurysms than men and are at higher risk of rupture. When it comes to race and ethnicity, whites appear to have a higher incidence, but other groups are also affected and may experience different outcomes if they rupture. More research is needed to fully understand these differences.
Causes of brain aneurysms:
The exact cause of brain aneurysms is not yet fully understood, but the following factors can increase your risk:
• Congenital weakness in the blood vessel wall: Some people are born with weaker blood vessel walls.
• High blood pressure: Chronic high blood pressure can damage the blood vessel walls and weaken them.
• Smoking: Smoking damages the blood vessel walls.
• Drug use: Using certain drugs, such as cocaine and amphetamines, can cause your blood pressure to suddenly rise and increase your risk of an aneurysm rupturing.
• Family history: Having a family history of brain aneurysms increases your risk.
• Older age: Brain aneurysms are more common in adults, especially those over the age of 40.
• Gender: Women are more likely than men to develop brain aneurysms.
• Underlying conditions: Certain conditions, such as polycystic kidney disease and Ehlers-Danlos syndrome, can increase your risk of an aneurysm.
• Head injury: A severe blow to the head can damage blood vessels in the brain, leading to the formation of an aneurysm.
Infection: In rare cases, an infection of the blood vessel wall can cause an aneurysm.
It is said that aneurysms are usually diagnosed incidentally because patients usually do not have serious symptoms to investigate the problem.
Figure 1
History of aneurysm discovery in neurology
The first case I found under the title of cerebral aneurysm was a 45-year-old woman who had been referred due to headache and vision problems. When we took an MRI of the brain with contrast, we found that there was a very clear and severe aneurysm on the right side in the frontal lobe area. One of my colleagues in that country recommended that since this aneurysm is behind the frontal lobe, this issue can be controlled by placing a balloon stent, and that is what happened. In fact, the issue is in the patient's mind, who is still alive. Only one memory remains and no more.
The second case happened almost a year ago. Suddenly, while the patient wanted to rest as usual at night, she was faced with a severe headache. But when the patient is sent to the emergency room, within an hour the report comes that the CT scan showed a ruptured aneurysm in the right parietal lobe. The fact is that when I spoke to the patient's family, they explained to me that the man was a healthy person and there was no chronic disease recorded in his medical record. In this case, when the CT scan of the brain pointed to this diagnosis, the patient was immediately taken to emergency surgery. Fortunately, my colleagues, under the circle of Willis. The patient not only had his bleeding stopped, but he also had a guarantee of survival.
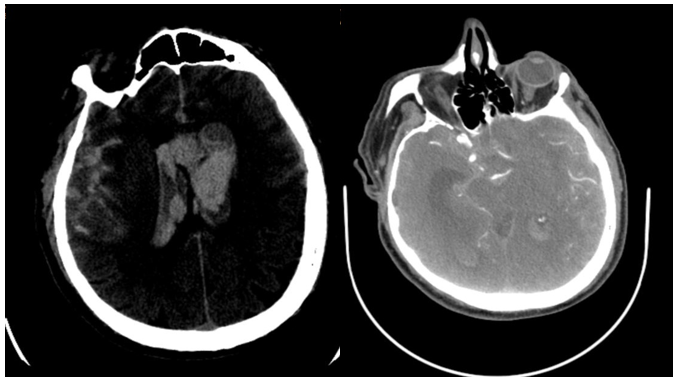
Fig 2: Brain CT-Scan of the third patient who died after few days of cerebral hemorrhage
But the third and most serious case is the one that actually motivated me to write this report because when it started, it quickly put the patient in a coma, and then after a CT scan, the problem of a brain aneurysm was confirmed, the patient never regained consciousness until they decided whether or not to perform surgery to drain the hematoma in the brain tissue or to ligate the aneurysm, because after four days in the intensive care unit, the patient died. Interestingly, this patient did not have any symptoms or complaints before the brain aneurysm ruptured and the massive bleeding that caused the patient to have this problem, and in fact, the sudden and rapid occurrence of such a problem left us all in shock and disbelief.
Symptoms of a brain aneurysm:
Many small brain aneurysms do not cause any symptoms until they rupture. However, larger aneurysms that are pressing on nearby tissues and nerves may cause the following symptoms:
• Headache: especially pain behind or above the eye
• Vision changes: blurred vision, double vision, decreased vision
• Drooping eyelid
• Dilated pupil
• Numbness or weakness on one side of the face
• Difficulty speaking
• Dizziness
• Loss of balance
Signs of a ruptured brain aneurysm (very dangerous and an emergency):
• Sudden, very severe headache
• Stiff neck
• Sensitivity to light
• Nausea and vomiting
• Seizures
• Loss of consciousness
Complications of a brain aneurysm:
The most important complication of a brain aneurysm is its rupture, which can lead to:
• Subarachnoid hemorrhage (SAH): Bleeding into the space between the brain and its protective covering. This is a very dangerous and life-threatening condition.
• Hemorrhagic stroke: Bleeding can cause permanent damage to brain tissue.
• Brain injury: Bleeding and the resulting pressure can lead to nerve damage, cognitive, motor, and sensory problems.
• Coma
• Death
• Rebleeding: After the initial rupture, there is a risk of rebleeding, which can be much more dangerous.
• Vasospasm: Narrowing of blood vessels in the brain after a hemorrhage that can restrict blood flow to the brain and cause further damage.
• Hydrocephalus: A buildup of cerebrospinal fluid in the brain.
Threats of brain aneurysms:
• Unpredictable rupture: It is difficult to tell which aneurysm will rupture and when.
And high mortality if ruptured: About 50 percent of people who have a ruptured aneurysm die.
Permanent disabilities: Many survivors of a ruptured aneurysm develop permanent neurological disabilities.
• Late diagnosis: Many aneurysms are not diagnosed until they rupture.
What causes a ruptured aneurysm?
The exact causes of a ruptured aneurysm are not fully understood, but several factors can increase the risk of rupture. In fact, rupture occurs when the weakened wall of the aneurysm can no longer withstand the blood pressure inside the vessel. Some of the most important factors contributing to aneurysm rupture include:
1. High blood pressure:
• Chronic and uncontrolled high blood pressure is one of the most important risk factors for aneurysm rupture. A sudden increase in blood pressure, especially during strenuous activity, severe stress, or taking certain medications, can put pressure on the weakened wall of the aneurysm and cause it to rupture.
2. Smoking:
• Smoking damages the walls of blood vessels and makes them weaker. Also, the nicotine in cigarettes can increase blood pressure, both of which increase the risk of aneurysm rupture.
3. Drug use: • Some drugs, especially cocaine and amphetamines, can cause a sudden, severe increase in blood pressure, significantly increasing the risk of aneurysm rupture.
4. Excessive alcohol consumption:
• Excessive alcohol consumption can also damage blood vessel walls over time and increase the risk of aneurysm rupture.
5. Aging:
• As you age, blood vessel walls naturally weaken, making aneurysms more likely to rupture.
6. Size and location of the aneurysm:
• Larger aneurysms are more likely to rupture than smaller ones. The location of the aneurysm in the brain can also affect its likelihood of rupture.
7. Sudden growth of the aneurysm:
• If an aneurysm grows suddenly, its wall may be stressed and rupture.
8. Head trauma:
• Severe head trauma can damage blood vessels in the brain and, in rare cases, cause an existing aneurysm to rupture.
9. Genetic factors and family history:
• People with a family history of brain aneurysms or certain genetic disorders associated with weak blood vessels are at higher risk of developing a ruptured aneurysm.
10. Infection:
• In rare cases, infection of the blood vessel wall can weaken it and increase the risk of aneurysm rupture.
11. Connective tissue disorders:
• Some congenital disorders that affect connective tissue, such as Ehlers-Danlos syndrome and Marfan syndrome, can weaken the blood vessel wall and increase the risk of aneurysm rupture.
Does stress play a role in these complications or in mortality?
Yes, stress can indirectly affect the complications and possibly the mortality rate of brain aneurysms. Here’s how these effects play ou.
How stress affects brain aneurysm complications:
• Increased blood pressure: Stress, especially chronic stress or acute and severe stress, can lead to high blood pressure. A sudden or sustained increase in blood pressure can put more pressure on the weakened aneurysm wall and increase the risk of rupture. A ruptured aneurysm itself is a major cause of many serious complications, such as subarachnoid hemorrhage, hemorrhagic stroke, brain injury, coma, and more.
• Impact on lifestyle: Stress can lead to unhealthy lifestyle choices, such as smoking, alcohol, and drug use to cope with stress. These factors directly damage the blood vessel walls and increase the risk of aneurysm formation and rupture.
• Inflammatory responses: Chronic stress can increase inflammation in the body. Some research suggests that inflammation may play a role in weakening the aneurysm wall and increasing the risk of rupture.
• Effects on the nervous system: Stress can stimulate the nervous system and potentially affect the blood vessels in the brain, although the exact mechanism is not yet fully understood.
Consequently, although stress is not a direct cause of aneurysms or death from them, it can play a significant role in increasing the risk of rupture and aggravating complications by affecting blood pressure and lifestyle, and indirectly affecting mortality.
My experience with the cases I have encountered, especially the last one that led to his sudden and sudden death, is that the issue of stress and its investigation is significant. Many times, patients who are constantly under stress at work may not show themselves and we only find out about it later. Likewise, we may not realize the type of stress that these patients have faced or are facing during the first visits, but being aware of this issue can set off alarm bells for us. Especially when these stresses progress in a hidden way within the person and the patient has no desire or interest in revealing these stresses to the outside world, not even to his doctor. Or with serious complications, this stress does not manifest itself outwardly, making this task more difficult. When we have a relative knowledge of the patient's condition, we can make the necessary predictions. Especially in the third case, which was a patient who I had known for more than forty years and had a relative knowledge of his diseases, when I encountered this issue, later when I went to investigate the issue, I came to the issue of stress, which can be a determining factor in the rupture process, that is, when we rule out parameters such as uncontrolled blood pressure or underlying diseases or trauma or infection, etc., the only issue that remains on the table is the issue of stress, and this is also significant. Because in many cases, patients are reluctant to discuss the amount and volume of their stress outside of themselves. Unless they face challenges, such as sleep disorders and ...
In case of rupture of a cerebral aneurysm (Subarachnoid Hemorrhage - SAH):
• It is very high and an emergency.
• About 25 percent of people die in the first 24 hours after rupture.
• About 50% of people die within 3 months of rupture due to complications.
• Even among survivors, about 66% develop permanent brain damage.
• Some studies have reported mortality rates as high as 65%.
• About 10 to 15% of patients die before reaching the hospital.
Factors affecting mortality rates after aneurysm rupture:
• Age of the patient: Older patients have a lower chance of survival.
• Neurological status at admission: Patients with worse neurological status at admission are more likely to die.
• Location of the aneurysm: Aneurysms located in the posterior circulation usually have a worse prognosis.
• Amount of bleeding: More severe bleeding is associated with a higher risk of death.
• Presence of complications: Complications such as vasospasm (narrowing of the blood vessels in the brain) and hydrocephalus (fluid buildup in the brain) can increase the risk of death.
• Timing of treatment: Prompt and timely treatment after rupture can increase the chance of survival.
• The patient's overall health and the presence of underlying diseases: The presence of underlying diseases such as high blood pressure can worsen the prognosis.
In summary, a ruptured brain aneurysm is a very dangerous condition with a high mortality rate. In contrast, unruptured aneurysms are usually not an immediate threat to life, but if detected, proper management and treatment are important to prevent possible rupture in the future.
Screening:
Brain aneurysms are not typically detected during routine, standard checkups. This is because:
• Most brain aneurysms are asymptomatic: Many people have one or more small brain aneurysms without knowing it, and these aneurysms do not cause any symptoms.
• Routine checkups do not include brain imaging: Routine medical checkups include blood tests, physical exams, and possibly some other tests, such as an electrocardiogram (ECG). Brain imaging, such as computed tomography (CT) or magnetic resonance imaging (MRI), is not typically performed during routine checkups for asymptomatic individuals. These procedures are expensive, and radiation exposure (in CT) or time-consuming (in MRI) are reasons why they are not routinely used.
• Routine screening is not recommended: Due to the relatively low incidence of aneurysm rupture in the general population and the risks and costs associated with brain imaging, routine screening for brain aneurysms is not recommended in asymptomatic individuals without a strong family history.
Conclusion
Although congenital cerebral aneurysm is a rare disease, it can be fatal in many cases or cause permanent complications in the patient and cause serious and irreversible disabilities for the sufferers. Attention to direct and indirect injuries, as well as chronic diseases and the patient's lifestyle, and regular screenings can prevent the occurrence of serious cases.
References
1. Clinical-Neurology-Aminoff-2018-10th-edition
2. Textbook of Clinical Neurology 2018 editors: J.B.M. Kuks J.W. Snoek
3. The 5-Minute Neurology Consult 2ND EDITION
4. Case Files neurology Copyright © 2008 by the McGraw-Hill Companies, Inc
5. Clinical Neurology 9 Edition (www.myuptodate.com)
6. 21 th edition Harrison’s principals of internal medicine.