Umbilical Cord Aneurysm: A Case Report
Umbilical Cord Aneurysm: A Case Report
Douha Abdalla1*,Ihab Abbasi 2 , Ahmed Mahmoud3, Mustafa Sabir Abakar Awad4, Asma Mustafa Ahmed Ali5, Dr Khadeeja Idrees6
1,2, 3,6. Department of Obstetrics and Gynaecology, Glangwili General Hospital.
4. Department of Community Medicine Al-Neelain University Faculty of Medicine, Khartoum – Sudan.
5. Abdullah Bin Omran Hospital For Obstetric and Gynecology.
*Correspondence to: Douha Abdalla, Department of Obstetrics and Gynaecology, Glangwili General Hospital, Carmarthen – Wales (UK).
Copyright
© 2024 Douha Abdalla. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 October 2024
Published: 30 December 2024
DOI: https://doi.org/10.5281/zenodo.14575525
Abstract
Abnormalities of the umbilical vessels are being increasingly identified prenatally as the result of more detailed ultrasound examination of the umbilical cord in utero. Aneurysm of the umbilical artery is the least common vascular anomaly found in the cord. In this case we report the postnatal diagnosis of aneurysm of the umbilical cord in 41-weeks neonate. The prenatal ultrasound findings, clinical course, subsequent management and outcome in these cases are reviewed.
Keywords: Case Report, Umbilical cord, Aneurysm.
Umbilical Cord Aneurysm: A Case Report
Introduction
An umbilical cord aneurysm is an extremely rare vascular anomaly characterized by the focal dilation of one or more vessels in the umbilical cord, which may involve the umbilical vein, arteries, or both. This condition is rarely encountered in clinical practice, with an estimated incidence of 0.02-0.1% in pregnancies, and poses significant risks to the fetus, including fetal hypoxia and intrauterine death if left undiagnosed and untreated [1].
Umbilical artery aneurysm is a rare structural anomaly of the umbilical cord and is frequently associated with fetal aneuploidy, fetal growth restriction and fetal demise [1]. In many cases, umbilical cord aneurysms are associated with chromosomal anomalies, such as trisomy 18 and 21, or other congenital malformations, further complicating the management of affected pregnancies. Despite its rarity, understanding the clinical presentation, diagnostic approaches, and management strategies for umbilical cord aneurysms is crucial to mitigate fetal morbidity and mortality [2,3]. Euploid fetuses with umbilical artery aneurysms have high rates of demise, typically occurring between 26- and 34-weeks’ gestation. It is quite dif?cult to ascertain the exact etiology and to predict the timing of greatest risk of intrauterine fetal demise (IUFD) [4].
Important clinical parameters, such as the in?uence of aneurysm size and location on perinatal outcomes, as well as the appropriate timing and mode of delivery, have yet to be fully elucidated [3]. Such information would undoubtedly improve patient counseling and support a more comprehensive multidisciplinary approach, involving perinatology, neonatology, and medical genetics teams.
The etiology of umbilical cord aneurysms remains largely unclear; however, potential contributing factors include underlying structural vascular defects, turbulent blood flow, or infections that compromise the integrity of the vessel wall [2]. Additionally, prenatal detection is challenging and often requires advanced imaging modalities, such as Doppler ultrasound, to identify abnormal blood flow patterns within the dilated vessels [4]. This case report aims to provide insights into the clinical course of an umbilical cord aneurysm, contributing to understating the condition, predisposing factors and it’s clinical implications.
Case Presentation
A 27-year-old English woman, gravida 2 para 0, with no significant medical history, presented as a non-smoker and did not consume alcohol.
The patient attended regular antenatal care visits, which were largely unremarkable except for a Group B Streptococcus (GBS) infection. Her family history was notable for heart disease, thrombotic events, and death of her partner’s brother due to Ataxia -telangiectasia. All of her antenatal care visits were unremarkable.
At 41 weeks, she delivered a female newborn with an umbilical cord aneurysm via assisted vaginal delivery. Labor lasted 19 hours and 12 minutes, with a 2-minute third stage. A histopathology was requested to identify the pathology within the umbilical tissues, the report revealed three vessels and 4 blocks from the umbilical insertion with placental bed, showing markedly distended, blood-filled vascular spaces and prominent clot formation within the lumen of the vessels, resulting in aneurysmal expansion. No degenerative changes were observed, consistent with umbilical artery aneurysm.
The neonate weighed 3.8 kg with a head circumference of 34 cm. APGAR scores were 7 at 1 minute and 9 at 5 minutes. Immediately after delivery, the neonate received a vitamin K injection and passed meconium. Due to the mother's GBS-positive status, the baby exhibited grunting and retractions, requiring Positive End-Expiratory Pressure (PEEP] for 20 minutes. The umbilical cord arterial pH was 7.028, and the venous pH was 7.35.
The neonate was successfully initiated on breastfeeding and was discharged in good condition.
Figure 1
Discussion
According to the literature, 63% of umbilical artery aneurysm [UAA] cases are associated with a single umbilical artery. This may result from compensatory enlargement of a single umbilical artery, leading to increased cardiac output in the developing fetus. This also explains why all cases were diagnosed after 21 weeks of pregnancy [1, 2]. The pathology occurs due to clot formation in the lumen of the vessel; an expanding aneurysm can compress the umbilical vein leading to fetal anemia, or a thin, abnormal vessel wall may be prone to rupture, resulting in perivascular hematoma. The risk of rupture is highest during delivery, and therefore, a cesarean section should be considered the preferred mode of delivery [1–5].
A MEDLINE search using the terms ‘umbilical cord’, ‘umbilical artery’ and ‘aneurysm’ revealed only two cases of umbilical artery aneurysm reported in the English language literature [5, 6]. Which a very small number indicates the need for further cases to aid in fully understating the condition and its implications.
We report a case of a 41-week neonate with unremarkable antenatal period, in which an umbilical cord aneurysm was discovered after delivery.
The mechanisms leading to the formation of aneurysms in the umbilical vessels are poorly understood, although congenital thinning of the vascular wall could be the most probable etiologic factor [7]. It seems likely that Wharton's jelly plays a critical role in preventing aneurysmal dilatation of the umbilical vessels, even when a significant weakness of the arterial or venous wall develops. This hypothesis is further supported by the observation that, although aneurysms are rarely found in the umbilical cord, they are relatively common in placental surface vessels, with a reported prevalence of up to 2% in detailed examinations of the chorionic vessels [8]. In our case, the aneurysm was located near the umbilical cord insertion with the placental bed. Nevertheless, despite of the rarity of this condition, the prenatal diagnosis of an umbilical artery aneurysm is significant due to its high association with life-threatening fetal complications, such as thrombosis and compression of neighboring vessels [5, 6]. These complications are not restricted to umbilical artery aneurysms, as they can also occur in cases of umbilical vein aneurysms, where fetal distress and unexpected intrauterine death have been reported [8, 9].
In this case, the umbilical artery aneurysm shares striking similarities in terms of clinical features and underlying pathology. The aneurysm was detected postnatally, located between the umbilical insertion and the placental bed, and was associated with otherwise normal three-vessel umbilical cord. The association between umbilical artery aneurysm and a single umbilical artery has been reported previously [6], although in that case, the aneurysm developed in the middle third of the cord and there were no associated anomalies. We are only aware of a recent report describing the prenatal diagnosis of an umbilical vein aneurysm due to an arteriovenous fistula in a fetus with trisomy 18[10]. It is possible that the development of an aneurysm in the umbilical vessels is a phenomenon that occurs preferentially late in pregnancy. The wide availability of early prenatal diagnosis and subsequent termination of pregnancies affected by trisomy 18 has made the detection of such associations increasingly rare. The reason for this association can be explained by the abnormal placental vasculature found in trisomy 18. It is well known that the placenta from third-trimester fetuses with autosomal trisomy shows a significant reduction in the number of small muscular arteries and a reduced small muscular artery-to-villus ratio[11], which may result in increased intraluminal vascular pressure, favoring the formation of aneurysms. Alternatively, the development of an aneurysm could represent a compensatory mechanism by which the feto-umbilical circulation attempts to reduce the already high downstream resistance of the trisomic placenta.
Umbilical cord anomalies, although rare, are associated with significant fetal morbidity and mortality. Therefore, careful prenatal examination of the umbilical cord by ultrasound to detect these anomalies has been advocated [12]. If an anechogenic lesion is detected in the umbilical cord, differential diagnoses to consider include true cysts, pseudocysts, aneurysm of the umbilical vessels, and umbilical vein varix. In these cases, color Doppler ultrasound plays a critical role in differentiating vascular from non-vascular lesions. If multiple congenital anomalies are detected, prenatal karyotyping is mandatory to guide clinical management. In cases of localized dilatation of the umbilical vessels in otherwise structurally normal fetuses, close antenatal fetal surveillance and delivery as soon as fetal lung maturity is confirmed are recommended.
Conclusion
Umbilical artery aneurysm is a rare structural anomaly of the umbilical cord. Recommendations for adequate intervals of fetal monitoring and surveillance require further studies with more reported cases to inform prudent management guidelines. When monitoring the aneurysms with ultrasound, changes in size as well as Doppler indices play a pivotal role in helping to determine the timing and mode of delivery, thus allowing for a favorable outcome, as seen in this case.
Competing interests: The authors declare that they have no competing interests.
Funding: Not applicable.
Acknowledgements: Not applicable.
References
1. Parast, M. M., & Boyd, T. K. (2018). Pathology of the umbilical cord. American Journal of Clinical Pathology, 149(2), 100-110.
2. Wolman, I., Altman, E., & Jaffa, A. J. (1997). Umbilical artery aneurysm diagnosed in utero: a case report and review of the literature. Journal of Ultrasound in Medicine, 16(7), 501-504.
3. Sepulveda, W., & Romero, R. (2005). Prenatal diagnosis of umbilical cord aneurysm using color Doppler and three-dimensional ultrasound. Journal of Ultrasound in Medicine, 24(8), 1141-1145.
4. Sepulveda, W., & Espinoza, J. (2003). Prenatal diagnosis of umbilical cord anomalies. Prenatal Diagnosis, 23(9), 759-763.
5. Fortune DW, Ostor AG. Umbilical artery aneurysm. Am J Obstet Gynecol 1978; 131: 339–340.
6. Siddiqi TA, Bendon R, Schultz DM, Miodovnik M. Umbilical artery aneurysm: prenatal diagnosis and management. Obstet Gynecol 1992; 80: 530–533.
7. Benirschke K, Kaufmann P. Pathology of the Human Placenta ( 4th edn.) New York, NY: Springer-Verlag, 2000; 373–375.
8. Wentworth P. Some anomalies of the foetal vessels of the human placenta. J Anat 1965; 99: 273–282
9. White SP, Kofinas A. Prenatal diagnosis and management of umbilical vein varix of the intra-amniotic portion of the umbilical vein. J Ultrasound Med 1994; 13: 992–994.
10. Vandevijver NM, Hermans RH, Schrandel-Stumpel CC, Arends JW, Peeters LL, Moerman PL. Aneurysm of the umbilical vein: case report and review of the literature. Eur J Obstet Gynecol Reprod Biol 2000; 89: 85–87
11. Berg C, Geipel A, Germer U, Gloeckner-Hofmann K, Gembruch U. Prenatal diagnosis of umbilical cord aneurysm in a fetus with trisomy 18. Ultrasound Obstet Gynecol 2001; 17: 79–81
12. Rochelson B, Kaplan C, Guzman E, Arato M, Hansen K, Trunca C. A quantitative analysis of placental vasculature in the third-trimester fetus with autosomal trisomy. Obstet Gynecol 1990; 75: 59–63
13. Nyberg DA, Souter VL. Sonographic markers of fetal trisomies: second trimester. J Ultrasound Med 2001; 20: 655–674
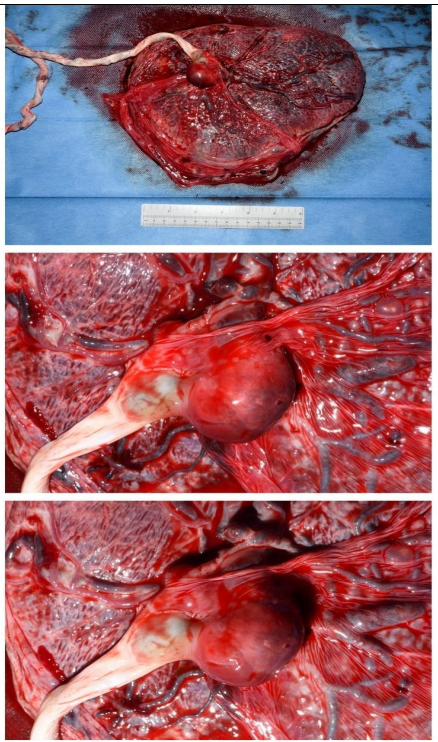
Figure 1