Enhanced Postoperative Pain Relief with Ultrasound-Guided Oblique Subcostal Transversus Abdominis Plane (OSTAP) Block Using Ropivacaine Following Laparoscopic Cholecystectomy: A Detailed Prospective Observational Analysis
Enhanced Postoperative Pain Relief with Ultrasound-Guided Oblique Subcostal Transversus Abdominis Plane (OSTAP) Block Using Ropivacaine Following Laparoscopic Cholecystectomy: A Detailed Prospective Observational Analysis
Dr. Sandeep Agrawal1*, Dr. Subramanian Manimaran2
1. Specialist Anesthetist, Department of Anaesthesia, Sheikh Khalifa Medical City- Ajman, UAE.
2. Consultant Anaesthesia, Department of Anaesthesiology, Asian Institute of Nephrology and Urology Hospital, Nungambakkam, Chennai, India. 600034.
*Correspondence to: Dr. Sandeep Agrawal, Specialist Anesthetist, Department of Anaesthesia, Sheikh Khalifa Medical City- Ajman, UAE.
Copyright.
© 2025 Dr. Sandeep Agrawal This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 June 2025
Published: 01 July 2025
DOI:https://doi.org/10.5281/zenodo.15797857
Abstract
Background: Acute postoperative pain remains a substantial concern for patients undergoing abdominal surgeries, including laparoscopic cholecystectomy (LC). Despite its minimally invasive nature, LC often leads to significant pain during the immediate postoperative period. The Oblique Subcostal Transversus Abdominis Plane (OSTAP) block, guided by ultrasound, has emerged as a novel regional anesthesia technique that may enhance pain control while reducing reliance on opioids.
Objective: This study aimed to assess the analgesic efficacy of ultrasound-guided OSTAP block with ropivacaine in patients undergoing laparoscopic cholecystectomy, focusing on VAS scores, time to first analgesia, opioid consumption, and adverse events within the first 24 hours postoperatively.
Methods: A prospective observational study was conducted on 80 patients aged 18–70 years with ASA physical status I-II scheduled for elective LC. Patients were randomly divided into two groups: Group A received bilateral ultrasound-guided OSTAP block with 20 mL of 0.2% ropivacaine per side; Group B received conventional analgesia alone. All patients underwent standardized general anesthesia. Pain was evaluated using the Visual Analog Scale (VAS) at 0, 2, 4, 6, 12, and 24 hours. Tramadol was administered as rescue analgesia for VAS > 4. Time to first analgesia, total tramadol consumption, and adverse effects were recorded and analyzed.
Results: VAS scores were significantly lower in Group A at all measured time points. Group A reported a mean 24-hour VAS of 2.4 ± 1.3 compared to 4.8 ± 3.4 in Group B. The average time to first analgesic request in Group A was 7.25 ± 1.2 hours versus 4.05 ± 0.8 hours in Group B (p=0.003). Group A also had significantly lower total tramadol consumption (80 ± 30.2 mg) compared to Group B (170 ± 70.5 mg). No significant difference was observed in the incidence of postoperative complications between the groups.
Conclusion: Ultrasound-guided OSTAP block with ropivacaine is a highly effective and safe technique for postoperative analgesia following laparoscopic cholecystectomy. It reduces pain scores, delays the requirement for rescue analgesia, and lowers opioid consumption without increasing adverse effects.
Keywords: OSTAP block, Laparoscopic Cholecystectomy, Postoperative Pain, Ropivacaine, Ultrasound-Guided Block, VAS, Regional Anesthesia.
Enhanced Postoperative Pain Relief with Ultrasound-Guided Oblique Subcostal Transversus Abdominis Plane (OSTAP) Block Using Ropivacaine Following Laparoscopic Cholecystectomy: A Detailed Prospective Observational Analysis
Introduction
Laparoscopic cholecystectomy (LC) has become the procedure of choice for gallbladder removal due to its minimally invasive nature, shorter hospital stay, and reduced overall morbidity. However, pain during the early postoperative period continues to be a significant challenge. The pain arises from surgical incisions, pneumoperitoneum, and tissue manipulation, necessitating effective analgesia to improve recovery outcomes and patient comfort.
Traditionally, opioids have been used as the primary method of analgesia but are associated with side effects such as nausea, vomiting, sedation, respiratory depression, and delayed bowel function. In recent years, multimodal analgesia strategies incorporating regional techniques have been increasingly recommended. One such technique is the Transversus Abdominis Plane (TAP) block, initially introduced by Rafi and later refined by Hebbard with ultrasound guidance for precise drug delivery.
The Oblique Subcostal TAP (OSTAP) block targets the upper abdominal wall by depositing local anesthetics between the transversus abdominis and rectus muscles. The use of ultrasound enables accurate needle placement, enhancing efficacy and minimizing risks. Previous studies have suggested that OSTAP blocks can significantly reduce postoperative pain and opioid requirements after various abdominal surgeries.
This study investigates the impact of OSTAP block with ropivacaine on postoperative pain relief, opioid use, and adverse effects in patients undergoing LC.
Methods
Study Design and Setting: This prospective observational study was carried out at the Department of Anesthesiology, Asian Institute of Nephrology and Urology, Chennai, India, over a period of 18 months.
Patient Selection: Eighty patients of either sex, aged 18–70 years, and categorized as ASA physical status I or II, were enrolled. Patients undergoing elective LC were included. Exclusion criteria included allergy to local anesthetics, acute cholecystitis, severe cardiopulmonary or neurological disorders, and conversion to open surgery.
Group Allocation: Patients were divided into two groups of 40 each:
- Group A: Received ultrasound-guided bilateral OSTAP block with 20 mL of 0.2% ropivacaine per side.
- Group B: Received only conventional postoperative analgesia.
Anesthesia Protocol: All patients received a standard general anesthesia regimen. Induction included IV midazolam (3 mg), glycopyrrolate (0.2 mg), fentanyl (1.5 µg/kg), propofol (2.5 mg/kg), and rocuronium (0.6 mg/kg). Maintenance was achieved with sevoflurane in a 60:40 N2O-O2 mixture.
OSTAP Block Technique: Following surgery, an OSTAP block was performed under ultrasound guidance using a Sonosite machine with a 6–13 MHz linear probe. After skin preparation, the transducer was placed 2 cm subxiphoid and moved along the subcostal margin to identify the rectus abdominis and transversus abdominis muscles. A 20 G insulated needle was introduced in-plane, and correct needle placement was confirmed with saline injection. Then, 20 mL of 0.2% ropivacaine was injected on each side, with real-time visualization of drug spread.
Postoperative Monitoring and Data Collection: Pain was assessed using VAS scores at 0, 2, 4, 6, 12, and 24 hours postoperatively. Tramadol (1 mg/kg) was administered as rescue analgesia when VAS exceeded 4. Time to first analgesia, total tramadol consumption, and adverse events (nausea, vomiting, shoulder pain, pruritus) were recorded.
Statistical Analysis: Data were analyzed using SPSS v20.0. Continuous variables were presented as mean ± SD and compared using Student’s t-test or Mann-Whitney U-test. Categorical variables were analyzed using Chi-square or Fisher’s exact test. A p-value < 0.05 was considered statistically significant.
Results
Demographics: No significant differences were observed between the groups in age, sex, weight, height, ASA grade, or surgery duration (p > 0.05).
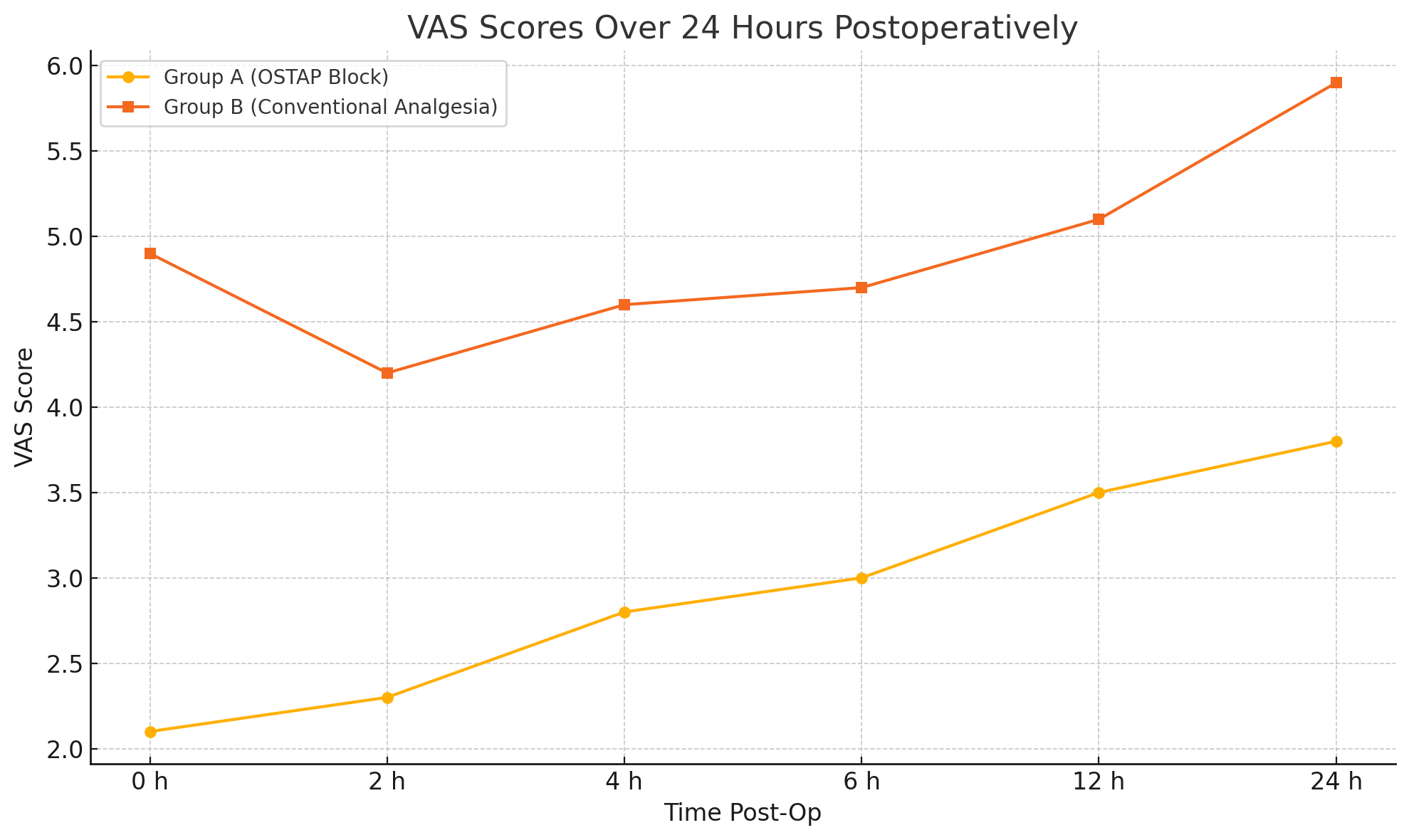
Pain Scores: VAS scores were consistently lower in Group A across all time intervals (0–24 hours), with statistical significance (p < 0.05). The average 24-hour VAS score was significantly lower in Group A (2.4 ± 1.3) compared to Group B (4.8 ± 3.4).
Time to First Analgesia and Tramadol Use: Group A showed a longer time to first analgesic request (7.25 ± 1.2 h vs. 4.05 ± 0.8 h, p = 0.003) and required significantly less tramadol (80 ± 30.2 mg vs. 170 ± 70.5 mg).
Adverse Events: There was no statistically significant difference in the incidence of postoperative complications, such as nausea, vomiting, or pruritus, between the two groups.
Table 1: Demographic Profile of Study Participants
|
Variable |
Group A (OSTAP) |
Group B (Conventional) |
P-value |
|---|---|---|---|
|
Age (years) |
46.55 ± 12.56 |
47.80 ± 11.37 |
0.810 |
|
Sex (M/F) |
15/25 |
17/23 |
0.756 |
|
Weight (kg) |
61.50 ± 8.87 |
62.50 ± 9.88 |
0.721 |
|
Height (cm) |
166.2 ± 3.61 |
168.5 ± 4.21 |
0.642 |
|
ASA (I/II) |
22/18 |
23/17 |
0.562 |
|
Duration of Surgery |
49.13 ± 10.13 |
48.91 ± 9.98 |
0.467 |
Table 2: Postoperative VAS Scores (Mean ± SD)
|
Time Point |
Group A (OSTAP) |
Group B (Conventional) |
P-value |
|---|---|---|---|
|
0 hours |
2.1 ± 1.2 |
4.9 ± 1.6 |
0.0001 |
|
2 hours |
2.3 ± 1.1 |
4.2 ± 2.2 |
0.012 |
|
4 hours |
2.8 ± 1.5 |
4.6 ± 3.1 |
0.0056 |
|
6 hours |
3.0 ± 1.9 |
4.7 ± 2.6 |
0.0028 |
|
12 hours |
3.5 ± 2.5 |
5.1 ± 2.9 |
0.029 |
|
24 hours |
3.8 ± 2.1 |
5.9 ± 3.2 |
0.0061 |
Figure 1
Discussion
Our findings affirm that the ultrasound-guided OSTAP block is a valuable regional anesthesia technique for improving postoperative pain control in LC. Patients receiving the block had lower pain scores, delayed analgesic requirements, and reduced opioid use.
Consistent with studies by Champaneria et al. and Mishriky et al., TAP and OSTAP blocks have demonstrated efficacy in abdominal surgeries, including hysterectomies and cesarean sections. Ultrasound guidance enhances safety by allowing real-time visualization of anatomical structures and needle positioning.
The relatively avascular nature of the TAP facilitates sustained local anesthetic action, reducing the need for systemic analgesics and associated side effects. The findings of this study align with earlier literature confirming the analgesic benefits of regional blocks in multimodal pain management protocols.
No complications related to the block were observed, underscoring its safety profile when performed under ultrasound guidance.
Conclusion
Ultrasound-guided OSTAP block with ropivacaine offers superior postoperative analgesia in patients undergoing laparoscopic cholecystectomy. It is associated with lower VAS scores, prolonged time to first analgesic request, and reduced opioid consumption, without added risk of complications. Incorporating this technique into routine perioperative care can enhance patient comfort, accelerate recovery, and reduce opioid dependency.
References
1. Bucher P, Pugin F, Buchs NC, et al: Randomized clinical trial of laparoendoscopic singlesite versus conventional laparoscopic cholecystectomy. Br J Surg 2011; 98: 1695–702.
2. Keus F, de Jong JA, Gooszen HG, et al: Laparoscopic versus open cholecystectomy for patients with symptomatic cholecystolithiasis. Cochrane Database Syst Rev 2006; 18:CD006231.
3. Bisgaard T, Klarskov B, Kehlet H, et al: Preoperative dexamethasone improves surgical outcome after laparoscopic cholecystectomy: a randomized double-blind placebo-controlled trial. Ann Surg 2003; 238: 651–660.
4. Barczynski M, Herman RM: A prospective randomized trial on comparison of low-pressure and standard-pressure pneumoperitoneum for laparoscopic cholecystectomy. Surg Endosc 2003; 17: 533–538.
5. Buvanendran A, Kroin JS: Multimodal analgesia for controlling acute postoperative pain. Curr Opin Anaesthesiol 2009; 22: 588–593.
6. Rafi AN. Abdominal field block: a new approach via the lumbar triangle. Anaesthesia 2001; 56: 1024-1026.
7. Johns N, O’Neill S, Ventham NT, et al: Clinical effectiveness of transversus abdominis plane (TAP) block in abdominal surgery: a systematic review and meta-analysis. Colorectal Dis 2012; 14:e635–e642.
8. Hebbard P. Subcostal transversus abdominis plane block under ultrasound guidance. Anesth Analg 2008; 106: 674-675.
9. Hebbard P, Fujiwara Y, Shibata Y, Royse C. Ultrasound-guided transversus abdominis plane (TAP) block. Anaesth Intensive Care 2007; 35: 616-6176.
10. Siddiqui MR, Sajid MS, Uncles DR, et al: A meta-analysis on the clinical effectiveness of transversus abdominis plane block. J Clin Anesth 2011; 23: 7–14.
11. Charlton S, Cyna AM, Middleton P, et al: Perioperative transversus abdominis plane (TAP) blocks for analgesia after abdominal surgery. Cochrane Database Syst Rev 2010; 12:CD007705.
12. Carney J, Finnerty O, Rauf J, et al: Studies on the spread of local anaesthetic solution in transversus abdominis plane blocks. Anaesthesia 2011; 66: 1023–1030.
13. Moher D, Liberati A, Tetzlaff J, et al: Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 2009; 339:b2535.
14. Von Korff M, Saunders K, Thomas Ray G, et al: De facto long-term opioid therapy for noncancer pain. Clin J Pain 2008; 24: 521–527.
15. Peng K, Liu HY, Wu SR, et al: Effects of combining dexmedetomidine and opioids for postoperative intravenous patient-controlled analgesia: a systematic review and meta-analysis. Clin J Pain 2015; 31: 1097–1104.
16. McDonnell JG, O’Donnell BD, Curley GCJ, et al. The analgesic efficacy of transversus abdominis block after abdominal surgery. Anesth Analg 2007; 104: 193–7.
17. Niraj G, Kelkar A, Fox A. Application of the transversus abdominis plane (TAP) block in the intensive care unit. Anaesth Intensive Care 2009; 37.
18. Rozen WM, Tran TM, Ashton MW, Barrington MJ, Ivanusic JJ, Taylor GI. Refining the course of the thoracolumbar nerves: a new understanding of the innervation of the anterior abdominal wall. Clin Anat.2008; 21:325–333.
19. Petersen PL, Mathiesen O, Torup H, Dahl JB. The transverses abdominis plane block: a valuable option for postoperative analgesia? A topical review. Acta Anaesthesiol Scand. 2010;5:529–35.
20. Champaneria R, Shah L, Geoghegan J, Gupta JK, Daniels JP. Analgesic effectiveness of transversus abdominis plane blocks after hysterectomy: a meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2013;166:1–9. 30. Charlton S, Cyna AM, Middleton P, Griffiths JD. Perioperative transversus abdominis plane (TAP) blocks for analgesia after abdominal surgery. Cochrane Database Syst Rev. 2010:CD007705.