Exploring Vidian Nerve Schwannomas, A Case Report and Literature Review
Exploring Vidian Nerve Schwannomas, A Case Report and Literature Review
Maryam Aljawi, MD 1*, Maryam Aljneibi2, MD, Mohamed Elhammady, MD3, Florian Roser, MD4, Mahdi A. Shkoukani, MD5
1,2,5: Otolaryngology head and neck surgery, Cleveland Clinic Abu Dhabi, UAE .
3: Neurosurgery, Cleveland Clinic Abu Dhabi, UAE.
4: Florian Roser, MD – Neurosurgery, Cleveland Clinic Abu Dhabi, UAE
*Correspondence to: Maryam Aljawi, Otolaryngology head and neck surgery, Cleveland Clinic Abu Dhabi, UAE.
Copyright
© 2025 Maryam Aljawi, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 June 2025
Published: 30 June 2025
Abstract
Vidian nerve schwannomas are extremely rare enteties with a handful of cases reported in the literature. Diagnosis can be challenging due to the paucity of cases and the wide differential diagnosis of anterior skull base lesions. Vidian nerve schwannomas can present with symptoms such as headaches, decreased sensation over V2 distribution, decreased lacrimation or nasal dryness. These symptoms are not specific since any sphenoid or skull base lesion can cause a mass effect on the Vidian or Trigemenal nerve.
Surgical approaches to Vidian schwannomas are particularly challenging due to the difficult access to the lateral recess of the sphenoid sinus. Extended endoscopic skull base approaches have largely replaced the open approaches through the pterygopalatine fossa and have become the gold standard with good exposure and lower morbidity and complications. Although these tumors are benign, they can cause significant morbidity due to mass effect on the surrounding structures such as the optic nerve.
We present a case of a 45-year-old woman who presented with vision changes and dryness of the eye. MRI showed a large homogenous contrast enhancing mass in the sphenoid sinus with bone remodeling of the skull base. She underwent transsphenoidal endonasal excision of the mass by the otolaryngology and neurosurgery team. Intraoperatively, the mass in the lateral recess of the sphenoid was difficult to access and a transptyregoid approach was used for better exposure. Complete resection of the tumor was achieved. Final surgical pathology came back as schwannoma. Further review of the preoperative MRI concluded the mass to be of a Vidian nerve origin. She was evaluated by ophthalmology at 1 month and 6 months postoperatively and had stable optic neuropathy with no progression in symptoms.
Exploring Vidian Nerve Schwannomas, A Case Report and Literature Review
Introduction
Vidian nerve schwannomas are exceedingly rare, with only a limited number of cases documented in the medical literature. Diagnosing these tumors can be particularly challenging due to their paucity and the broad differential diagnosis associated with anterior skull base lesions. Symptoms of Vidian nerve schwannomas may include headaches, reduced sensation in the V2 distribution, hypolacrimation, or nasal dryness. However, these symptoms are nonspecific, as any lesion within the sphenoid sinus or anterior skull base can exert a mass effect on the Vidian or trigeminal nerves, leading to similar clinical manifestations.
The surgical management of Vidian nerve schwannomas is further complicated by the challenging anatomical location of the tumor, which is often situated in the lateral recess of the sphenoid sinus. Historically, open approaches through the pterygopalatine fossa were employed; however, these have largely been replaced by extended endoscopic skull base techniques. Endoscopic approaches are now considered the gold standard for their ability to provide excellent exposure while minimizing patient morbidity and surgical complications.
Although Vidian nerve schwannomas are benign in nature, their growth can result in significant morbidity due to the mass effect they exert on surrounding critical structures, such as the optic nerve. Early diagnosis and appropriate surgical intervention are essential to prevent long-term complications and preserve patient quality of life.
Case Presentation
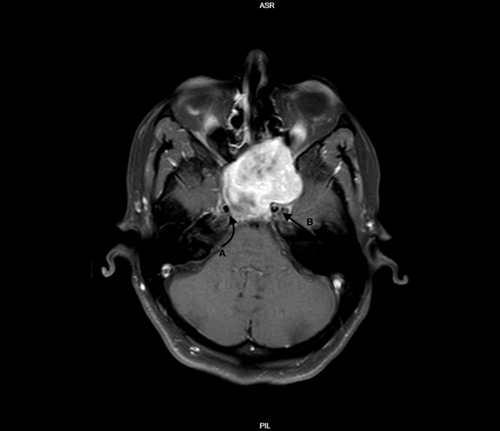
We report the case of a 45-year-old woman who presented with complaints of vision changes and dryness in her eye. Magnetic resonance imaging (MRI) revealed a large, homogeneously contrast-enhancing mass located in the sphenoid sinus, accompanied by evidence of bone remodeling at the skull base (Figure 1,2).
The patient underwent a transsphenoidal endonasal excision of the mass, performed collaboratively by the otolaryngology and neurosurgery teams. Intraoperatively, the tumor was found to be located in the lateral recess of the sphenoid sinus, a region that posed significant challenges for access. To overcome this, a transpterygoid approach was employed, providing better surgical exposure. Complete resection of the tumor was successfully achieved.
Final histopathological analysis of the excised tissue confirmed the diagnosis of schwannoma. Subsequent detailed review of the preoperative MRI suggested that the mass originated from the Vidian nerve.
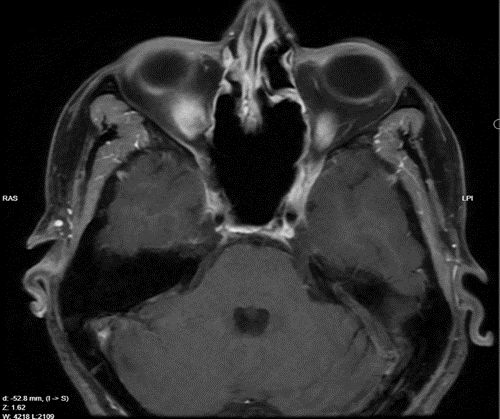
Postoperatively, the patient was closely monitored by ophthalmology. At follow-ups conducted one month and six months after surgery, she demonstrated stable optic neuropathy without any progression of her symptoms (Figure 4).
|
Cases |
Author |
Age |
Gender |
Tumor size |
Clinical presentation |
Management |
Outcome |
|
1 |
Cheong et al., 2006 |
13 |
F |
12mmx10mm |
Headache and unilateral facial palsy |
EES |
N.A |
|
2 |
Honda et al., 2008 |
49 |
F |
N.A |
Unilateral hearing loss and serous otitis media |
Maxillary swing with endoscopic assistance |
No recurrence in 1 month |
|
3 |
Hackman et al., |
49 |
M |
10mmx14mm |
Occipital headache |
Observation |
N.A |
|
4 |
Hackman et al., |
58 |
M |
N.A |
Unilateral palate pain and lip numbness |
EES |
N.A |
|
5 |
Wu et al., 2012 |
78 |
F |
N.A |
Unilateral oculomotor palsy and CSF leak |
EES |
No recurrence in 24 months |
|
6 |
Hong et al., 2014 |
41 |
M |
28mmx16mm |
Occipital headache |
EES |
N.A |
|
7 |
Yamasaki et |
49 |
F |
20mmx14mm |
Asymptomatic |
Radiation thearpy |
N.A |
|
8 |
Fortes et al., 2019 |
60 |
F |
N.A |
Unilateral facial hypostheisa |
EES |
No recurrence in 3 months |
|
9 |
Masroor et al., 2018 |
54 |
F |
41mmx36mm |
Periorbital pressure and oculomotor plasy, visual field defect |
EES |
No recurrence in 28 months |
|
10 |
Tanaka et al., 2021 |
21 |
F |
44mmx36mm |
Hypolacrimination |
EES |
No recurrence in 5 months |
|
11 |
Bang et al., 2024 |
58 |
F |
N.A |
Headache and left eye dryness |
EES |
No recurrence in 8 months |
Figure 1: T1 MRI Axial view of the lesion
Figure 2: T1 MRI coronal view of the lesion
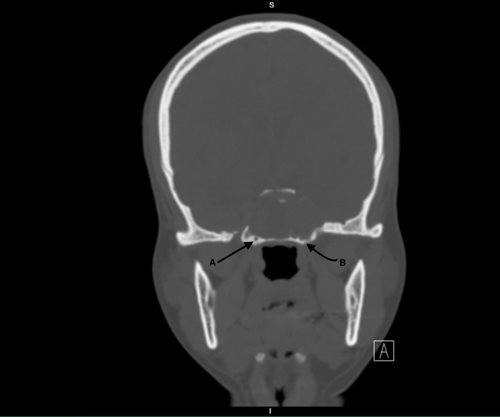
Figure 3: CT coronal view bone window showing bilateral vidian canals
Figure 4: T1 MRI axial view post resection
Discussion
Head and neck schwannomas are not uncommon. They most commonly arise from the vestibular nerve, acounting to around 51%7. Followed by the trigeminal nerve accounting for 8%7. The diagnosis of schwannomas is typically made histologically. However, this could be predetected on preoperative imaging with certain charactarisitcs including iso or hypointensity on T1 images, hyperintensity on T2 images and enhancement with contrast. The MRI scan is also helpful in determining the origin of these tumors with features such as bone remodeling and enlargement of ther bony canals of the affected nerve. Vidian nerve schwannomas are a rare entity with only previous 11 cases reported in the literature to our knowledge summarized in table 1(1-10).
All previously reported cases of vidian nerve schwannoma presented with unspecific symptoms including headaches. Or symptoms from compression of other cranial nerves including hyposthesia, vision changes or hearing loss. There are no evident abnormalities, such as decreased lacrimation or nasal mucosal dryness, that have led to the investigation and diagnosis of vidian nerve tumors.
The standard treatment is surgical resection, which is also the gold standard for diagnosis to obtain histopathologic confirmation. Previously, open approaches were utilized for surgical access due to the difficulty in reaching areas such as the lateral recess of the sphenoid and the pterygopalatine fossa, as well as the potential challenges associated with the need to ligate internal maxillary artery branches in those regions.
Historically, approaches such as the maxillary swing or a combination of a Caldwell-Luc or Denker’s approach were the standard treatment. However, the endoscopic endonasal approach has now largely replaced open procedures in experienced hands, minimizing morbidity and shortening hospital length of stay.
Conclusion
Vidian nerve schwannomas are difficult to diagnosis due to the unspecific presenting symptoms. Radiologic charactaristics can presume the diagnosis of a schwannoma. Surgical resection is the mainstay of treatment. Endoscopic endonasal approach has improved visualization of different regions of the anterior skull base and have allowed full resection with minimal morbidity and short hospital stay.
References
1. Cheong, J. H., Kim, J. M., Bak, K. H., Kim, C. H., Oh, Y. H., & Park, D. W. (2006). Bilateral vidian nerve schwannomas associated with facial palsy. Case report and review of the literature. Journal of neurosurgery, 104(5), 835–839. https://doi.org/10.3171/jns.2006.104.5.835
2. Honda, K., Asato, R., Tanaka, S., Endo, T., Nishimura, K., & Ito, J. (2008). Vidian nerve schwannoma with middle cranial fossa extension resected via a maxillary swing approach. Head & neck, 30(10), 1389–1393. https://doi.org/10.1002/hed.20793
3. Hackman, T., Rickert, C. G., Getz, A. E., & Uppaluri, R. (2011). Endoscopic surgical management of vidian nerve schwannoma. The Laryngoscope, 121(2), 241–244. https://doi.org/10.1002/lary.21285
4. Wu, S. W., Chen, W. L., Chen, W. L., & Chen, M. K. (2012). Transnasal endoscopic resection of vidian nerve schwannoma accompanied by sphenoid mucopyocele and oculomotor palsy: a case report. B-ENT, 8(3), 207–211.
5. Hong, H. P., Yoon, S. W., Park, M. J., & Jung, S.-C. (2014). A case of vidian nerve schwannoma: Resection by endoscopic sinus surgery. Korean Journal of Otorhinolaryngology-Head and Neck Surgery, 57(1), 50. https://doi.org/10.3342/kjorl-hns.2014.57.1.50
6. Yamasaki, A., Sedaghat, A. R., Lin, G. C., Curry, W. T., Shih, H. A., & Gray, S. T. (2015). A Rare Finding of Schwannoma of the Vidian Canal: A Case Report. Journal of neurological surgery reports, 76(1), e48–e51. https://doi.org/10.1055/s-0034-1544112
7. Fortes, B., Beer-Furlan, A., Balsalobre, L., Vellutini, E., & Stamm, A. (2019). Endoscopic endonasal access for the treatment of Vidian nerve schwannoma: a case report. Brazilian journal of otorhinolaryngology, 85(5), 670–672. https://doi.org/10.1016/j.bjorl.2016.04.015
8. Masroor, F. A., Gilde, J., & Liang, J. (2018). Vidian Nerve Schwannoma: A Rare Skull-Base Neoplasm Presenting with Ocular Manifestations: A Case Report and Literature Review. The Permanente journal, 22, 18–021. https://doi.org/10.7812/TPP/18-021
9. Tanaka, C., Kikuchi, M., Matsunaga, M., Omori, K., & Nakagawa, T. (2021). Endoscopic Endonasal Surgery of a Large Vidian Nerve Schwannoma With Preparation for Avoiding Major Vascular Injury. Cureus, 13(3), e14230. https://doi.org/10.7759/cureus.14230
10. Bang, J. H., Jin, S. H., Kim, S. J., & Lee, K. H. (2024). Vidian Nerve Schwannoma Extending Into the Foramen Rotundum in a Female Patient: A Case Report. Journal of rhinology : official journal of the Korean Rhinologic Society, 31(3), 184–188. https://doi.org/10.18787/jr.2024.00028.