Advantages of Expansion over IPR as a Pre-Aligner Treatment: A Comprehensive Review.
Advantages of Expansion over IPR as a Pre-Aligner Treatment: A Comprehensive Review.
Michael B. Guess, DDS, MS, MA*
*Correspondence to: Michael B. Guess, DDS, MS, MA, US
Copyright.
© 2025 Michael B. Guess This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 June 2025
Published: 03 July 2025
DOI: https://doi.org/10.5281/zenodo.15837990
ABSTRACT
Background: Orthodontic professionals increasingly adopt conservative treatment methods that preserve dental tissues while achieving optimal outcomes. Clinicians face critical decisions between arch expansion and interproximal reduction (IPR) as pre-treatment modalities before clear aligner therapy, with long-term implications for patient health and satisfaction.
Objective: This review examines the advantages of dental expansion over interproximal reduction as a pre-aligner treatment strategy, utilizing evidence from 2020 to 2025 to provide evidence-based clinical guidance.
Methods: We conducted a comprehensive literature review of clinical research, meta-analyses, and systematic reviews published between 2020 and 2025. We evaluated evidence quality using established standards, with a particular emphasis on recent studies that utilized Cone Beam Computed Tomography (CBCT) and reported long-term outcomes.
Results: Recent evidence demonstrates that expansion offers multiple advantages over IPR: preservation of enamel integrity, improved facial aesthetics through enhanced soft tissue support, better airway function, and superior long-term stability. CBCT-based studies reveal that exceeding 0.20 mm of single-site IPR significantly increases risk, particularly in patients with thin enamel (<0.7 mm). Slow expansion protocols reduce patient discomfort by 86% compared to rapid expansion, with no differences in treatment acceptance. Clear aligner-based expansion achieves 70% efficacy without the use of auxiliaries, facilitating effective integration with aligner therapy.
Conclusions: Expansion provides a more conservative, biologically appropriate treatment approach compared to IPR, with superior outcomes in facial aesthetics, airway function, and long-term stability. Integration of slow expansion protocols with clear aligner therapy optimizes patient comfort and treatment efficiency. Recent evidence from 2025 confirms that clear aligner treatment produces positive effects in growing patients, with particular efficacy for transverse expansion in mixed dentition patients (40). Additionally, systematic reviews indicate that clear aligners demonstrate favorable indications for mild to moderate malocclusions, with oral hygiene and oral health representing the most commonly reported advantages (41).
Keywords: arch expansion, clear aligners, pre-treatment, enamel preservation, facial aesthetics, interproximal reduction.
Advantages of Expansion over IPR as a Pre-Aligner Treatment: A Comprehensive Review.
Introduction
The orthodontic profession has witnessed a paradigm shift toward conservative treatment methodologies that prioritize tissue preservation while achieving optimal therapeutic outcomes. Traditional approaches to space management, including extraction therapy and interproximal reduction (IPR), often result in significant and irreversible alterations to dental anatomy and arch morphology. In contrast, the arch expansion represents a fundamentally different philosophy—one that creates space through biological adaptation rather than tissue removal (1).
The adoption of clear aligner therapy has intensified interest in pre-treatment space-gaining procedures. Recent systematic reviews have demonstrated that aligners effectively achieve arch expansion in both pediatric and adult populations, with predictability being superior in the mandibular arch compared to the maxillary arch (2). This expansion occurs through the biological capacity for dentoalveolar adaptation and, in growing patients, the potential for actual skeletal modification, resulting in increased arch perimeter that provides necessary space for alignment (3). Expansion increases arch size to make more room, while IPR reduces tooth shape to create space. (Fig 1)
Fig 1
Evidence Quality Assessment: This review prioritizes evidence from systematic reviews and meta-analyses (Level I), followed by randomized controlled trials (Level II) and well-designed cohort studies (Level III), with particular emphasis on studies published between 2020-2025 that utilize advanced imaging techniques such as cone-beam computed tomography (CBCT).
Clinical Benefits of Pre-Aligner Expansion
Increased Arch Perimeter and Space-Gaining
Expansion increases the arch perimeter by broadening the transverse dimension. Mathematical principles demonstrate that even small increases in arch width result in substantial gains in total available space (4). Unlike extraction therapy, which reduces the total number of teeth requiring accommodation, expansion preserves the complete dentition by creating additional space through arch enlargement. (See Fig 2A & B))
Fig 2
Contemporary research has quantified these benefits with greater precision. Studies demonstrate that expansion can increase arch perimeter by 2-8 mm, depending on the magnitude of expansion and individual arch morphology (5). Recent investigations using clear aligners confirm these findings, showing that increases in maxillary inter-canine, inter-premolar, and intermolar widths, as well as the dental arch perimeter, achieved significantly greater results among patients using optimized aligner protocols (6).
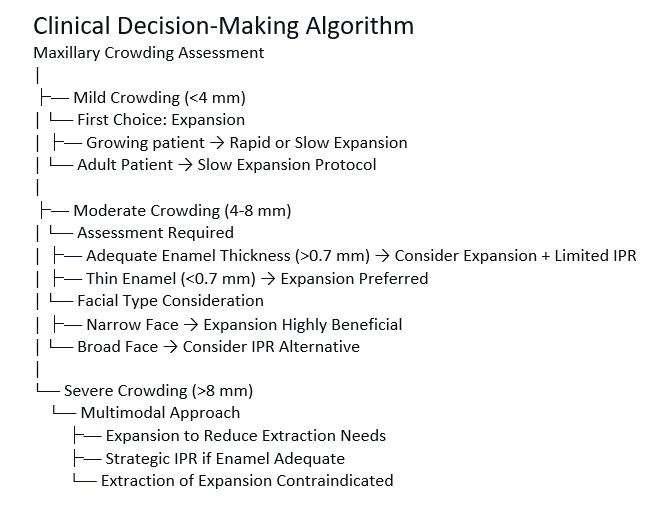
Clinical Decision Algorithm: For mild crowding (<4 mm), clinicians should consider expansion as the primary treatment option. For moderate crowding (4-8 mm), clinicians should evaluate expansion first, with IPR serving as a secondary option when expansion proves contraindicated. For severe crowding (greater than 8 mm), practitioners may consider extractions; however, careful arch expansion often provides a preferable alternative that maintains natural tooth alignment and creates a more aesthetically pleasing smile.
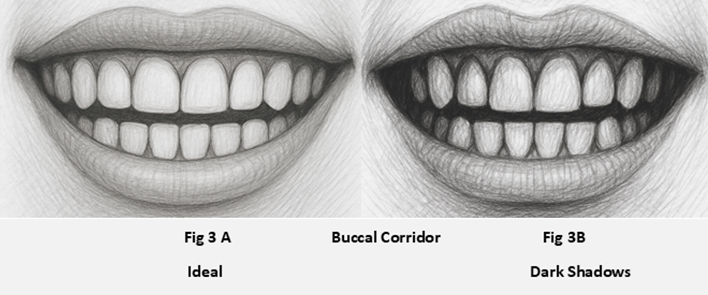
Enhanced Facial Aesthetics Through Buccal Corridor Optimization
Current aesthetic trends emphasize the importance of buccal corridor width in facial attractiveness. The buccal corridors—spaces between posterior teeth and mouth corners when smiling—significantly influence perceived facial attractiveness and overall smile harmony (7,8). Expansion techniques effectively address buccal corridor concerns by widening the oral arch, improving smile fullness, and reducing empty spaces (9). It becomes particularly evident in patients with naturally narrow dental arches or V-shaped arch forms, where posterior teeth occupy positions more lingually relative to ideal buccal corridor parameters.
Enhanced facial aesthetics yield significant psychological benefits that support dentofacial orthopedic goals and improve patient outcomes. The orthodontic expansion process proves essential for aligning teeth and creating beautiful smiles. Proper alignment enhances appearance and boosts patient confidence, encouraging positive experiences that promote treatment compliance. (Fig 3A &B)
Preserving Enamel Integrity: A Critical Advantage
Orthodontic expansion demonstrates the exceptional capacity to preserve dental enamel integrity compared to interproximal reduction. Patients achieve visually appealing smiles while maintaining the critical strength and health of natural tooth structure. IPR, by definition, involves irreversible enamel removal from adjacent tooth surfaces to create space for orthodontic movement. Even when practitioners perform this procedure within the recommended safety parameters, the process permanently alters the tooth structure, with potential long-term consequences.
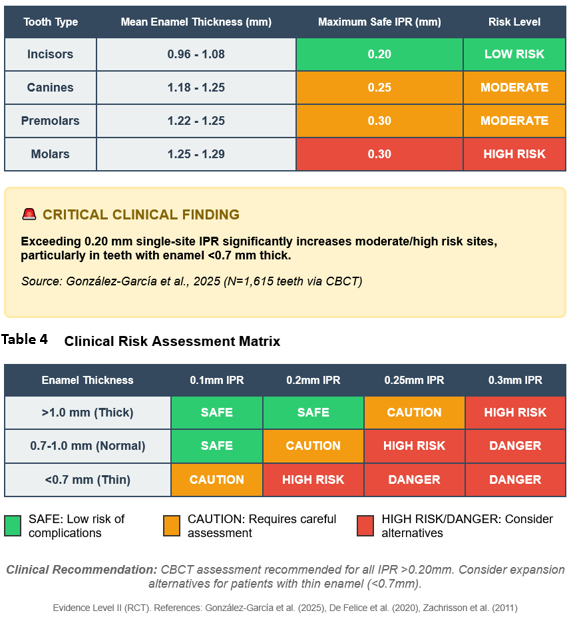
Updated IPR Safety Guidelines: Recent CBCT-based studies have revealed crucial information about enamel thickness variations and IPR safety. Exceeding the single-site IPR of 0.20 mm significantly increases the proportion of interproximal sites classified as moderate or high risk, particularly in teeth with thinner enamel (<0.7 mm) (10). Mean proximal enamel thickness varies between 0.96 and 1.29 mm on the mesial side and between 0.98 and 1.25 mm on the distal side, highlighting the need for individualized treatment planning (11).
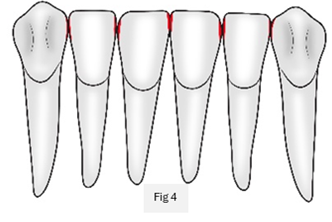
Current Evidence on IPR Complications: Recent longitudinal studies document concerning IPR outcomes. Researchers observed mild post-treatment sensitivity in 30% of patients after IPR, with symptoms persisting beyond the immediate post-treatment period (12). (See Table 1) Additionally, even small amounts of enamel removal can compromise the integrity of tooth structure, as enamel becomes more susceptible to caries and thermal sensitivity following IPR procedures (13). (See Table 2) (Fig 4)
Table 1: IPR Guidelines and Limitations
|
Tooth Surface |
Maximum IPR |
Enamel Thickness |
Safety Margin |
|---|---|---|---|
|
Maxillary Central |
0.3mm |
1.2-1.4mm |
0.9mm |
|
Maxillary Lateral |
0.4mm |
1.0-1.2mm |
0.6mm |
|
Maxillary Canine |
0.5mm |
1.4-1.6mm |
0.9mm |
|
Mandibular Incisor |
0.2mm |
0.8-1.0mm |
0.6mm |
|
Mandibular Canine |
0.4mm |
1.2-1.4mm |
0.8mm |
Reference: Zachrisson & Nyøygaard, 1982; Stroud et al., 1998
Table 1: Updated IPR Guidelines and Limitations
Tooth Type Maximum Safe IPR (per surface)Evidence Level Limitations
Incisors 0.20 mm Level II (RCT) High sensitivity risk in thin enamel
Canines 0.25 mm Level II (RCT) Structural integrity concerns
Premolars 0.30 mm Level III (Cohort) Limited long-term data
Molars 0.30 mm Level III (Cohort) Difficult access and visualization
Table 2: Mean Proximal Enamel Thickness by Tooth Type (CBCT Data 2025)
Five Evidence-Based Reasons to Avoid IPR:
1. Irreversible enamel loss with no possibility of natural regeneration
2. Increased sensitivity risk (30% of patients experience post-treatment sensitivity)
3. Caries susceptibility due to altered enamel surface characteristics
4. The technical difficulty in achieving a precise, uniform reduction
5. Individual variation in enamel thickness makes standardized approaches problematic
Preserving enamel through expansion encompasses multiple advantages. Intact enamel surfaces maintain superior resistance to caries formation and provide enhanced protection against thermal sensitivity (14) (See Table 4 & 5). Furthermore, preserved natural tooth contours help maintain proper interproximal contacts, reducing food impaction and plaque accumulation (15).
Table 3 Enamel Thickness and Maximum Safe IPR Limits
Enhanced Soft Tissue Support and Midface Volumization
A fundamental relationship exists between dental arch morphology and facial soft tissue support. When expansion moves posterior teeth in a controlled lateral direction, it increases support for midface soft tissues, creating a more youthful and harmonious facial appearance (16).
This enhancement in soft tissue support results in improved facial symmetry and a reduction in the appearance of hollow or sunken cheeks. Expansion proves particularly advantageous for individuals with narrower facial dimensions. Recent CBCT studies have quantified these changes, showing that maxillary expansion using micro-implant-supported expanders results in an average lateral movement of cheek points of 1.35 mm (right) and 1.08 mm (left), with corresponding changes in alar curvature points (17). The resultant midface fullness contributes to a more youthful appearance—a critical consideration when treating older patients, where facial aging concerns may influence treatment decisions.
Treatment of Posterior Crossbites
Dental and skeletal posterior crossbites represent common malocclusions that affect both function and aesthetics. Expansion offers an effective treatment modality for these conditions, particularly in growing patients (18). However, recent evidence regarding the relationship between crossbites and temporomandibular disorders (TMD) requires careful consideration.
Current Evidence on Crossbites and TMD: A 2018 systematic review found poor, very low-quality evidence regarding positional and dimensional effects of posterior crossbite correction on temporomandibular joints (17). While some studies identify associations between crossbites and TMD, evidence supporting this connection remains controversial (19). A comprehensive prospective study conducted in 2021 found a notable correlation between the presence of crossbite and an increased likelihood of patients reporting audible sounds from the temporomandibular joint. By age 32, the calculated odds ratio was 3.5 (95% CI: 1.1-11.6, p = 0.037). However, patients receiving orthodontic treatment did not experience a decrease in the frequency of TMJ-related symptoms, indicating that correcting dental misalignments through orthodontic interventions may not be sufficient to alleviate related symptoms (18) adequately.
Clinical Recommendation: Clinicians should emphasize both functional and aesthetic considerations when determining crossbite correction rather than solely relying on TMD prevention beliefs. Recent research indicates limited evidence supporting the use of crossbite correction as a method for preventing TMD.
During patient growth phases, implementing interceptive treatments that involve dental arch expansion can help prevent the emergence of crossbites. This proactive approach significantly reduces the need for more complex procedures during permanent dentition, ultimately benefiting long-term oral health.
Airway Function and Sleep-Related Benefits
Expansion benefits extend beyond aesthetic improvements to encompass substantial functional advantages, particularly for adolescents with developing skeletal structures. Expanding dental arches enhances airway capacity and improves overall oral function. Pre-aligner expansion facilitates better sleep breathing, aids proper jaw alignment, and leads to more effective chewing and speaking functions. These factors prove crucial as they directly impact the quality of life and overall well-being of growing patients.
Studies demonstrate that skeletal expansion procedures, including rapid and slow palatal expansion, enhance nasal airway function and optimize tongue posture. Increased maxillary width directly correlates with enhanced nasal cavity dimensions, potentially improving nasal breathing and reducing the tendency to mouth breathe (20).
Recent Meta-Analysis Evidence: A 2025 systematic review and meta-analysis of rapid maxillary expansion (RME) for obstructive sleep apnea (OSA) treatment concluded that RME represents an effective treatment modality for managing OSA. Quantitative parameters, including the apnea-hypopnea index (AHI) and oxygen saturation (SpO?), demonstrate functional benefits extending beyond dimensional changes alone (21). These benefits include improved sleep quality, reduced symptoms of sleep-disordered breathing, and enhanced overall health outcomes.
The connection between maxillary expansion and airway function represents a crucial factor during treatment planning, particularly for patients with breathing difficulties or sleep-related issues. Recent findings suggest that even modest increases in maxillary width can result in substantial improvements in airway dimensions and overall respiratory function.
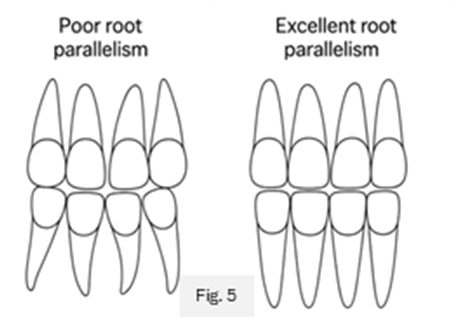
Improved Root Parallelism and Periodontal Health
Root positioning optimization represents a frequently overlooked advantage of expansion therapy. Proper root parallelism proves essential for long-term treatment stability and maintaining periodontal health. Expansion maintains optimal vertical root orientation while increasing arch perimeter, contrasting with alternative space-gaining methods that may cause increased root angulation or convergence, particularly in posterior regions (22).
Maintaining ideal root relationships improves long-term treatment stability and promotes superior periodontal health outcomes. Recent studies have shown that proper root positioning, achieved through expansion, reduces the risk of periodontal complications and enhances the long-term retention of orthodontic results (23). (Fig 5)
Expansion in Adult Patients: The Slow Expansion Revolution
While rapid palatal expansion (RPE) demonstrates effectiveness in growing patients, adult patients present unique considerations due to increased midpalatal suture resistance and decreased adaptive potential. Recent advances in slow expansion protocols show promising results in adults, offering alternative treatment options for mature patients seeking conservative space-gaining procedures.
Biological Rationale for Slow Expansion in Adults
Adult biology differs significantly from that of growing patients. In adult patients, the midpalatal suture demonstrates increased mineralization and bone interdigitation. Mature adults possess limited future growth potential, making rapid expansion more likely to cause trauma and unpredictable results. Slow expansion protocols, as developed by Williams and Haas, account for these biological differences by applying gentler forces over extended durations (24).
Recent systematic reviews comparing both approaches demonstrated the long-term effectiveness of slow maxillary expansion (SME) and RPE when researchers followed patients for extended periods after expansion treatment (25).
Slow expansion typically employs lighter forces (10-12 oz) with continuous or gradual activation to promote physiological adaptation of surrounding structures. It facilitates enhanced cellular remodeling rather than causing disruption, resulting in more stable expansion and reduced relapse risk.
Current recommendations for slow expansion protocols suggest extending activation schedules to a duration of 3-6 months, which is significantly longer than the traditional 2-3 weeks used for rapid expansion. Recent meta-analyses comparing SME with RME show that SME reduces pain intensity compared to RME during the first treatment week, with patients experiencing 86% less discomfort (26).
Slow expansion protocols typically involve initial activation periods followed by stabilization phases, allowing for optimal tissue adaptation and remodeling, which are crucial in orthodontic treatment. Haas highlighted the significance of conducting patient-specific assessments to determine optimal activation schedules, noting that adult patients may require up to 50% longer duration to achieve comparable expansion (27). Although this extended timeline requires more patience, the benefits of slow expansion over traditional rapid methods for adults prove considerable.
Recent comparative studies have shown that while both slow and rapid expansion techniques result in similar space gains, patients in slow expansion groups reported significantly less discomfort and higher treatment acceptance rates. Recent studies confirm these results, showing no differences between RME and SME during the first treatment week in speaking difficulty, swallowing issues, hypersalivation, hygiene concerns, and patient and parent satisfaction levels (28). Slow expansion also offers superior integration with other orthodontic procedures, facilitating easier transitions into clear aligner therapy.
Integration with Clear Aligner Systems
In modern orthodontics, slow expansion integrates seamlessly with clear aligner systems compared to traditional rapid palatal expander (RPE) appliances. This innovative approach enhances comfort and offers more effective solutions for achieving optimal smiles. Unlike RPE appliances, practitioners can apply slow expansion during the initial stages of aligner therapy, reducing overall treatment time and enhancing patient comfort (29).
Recent research supports aligner-based expansion effectiveness. Studies demonstrate that expansion achieved through clear aligner treatment proved slightly more efficient than expansion-only therapy due to the hysteresis characteristics of modern aligner materials (30). Clear aligner systems now incorporate built-in expansion protocols as part of treatment algorithms, allowing simultaneous arch expansion and tooth movement through integrated approaches.
Modern Clear Aligner Expansion Efficacy: Recent systematic reviews confirm that clear aligners achieve 70% efficacy in maxillary transverse expansion without the use of auxiliaries, making them highly effective for addressing mild to moderate expansion needs (31). A 2024 scoping review demonstrates that orthodontic aligners have proven effective in expanding arches in both adults and children, with greater predictability of expansion in the lower arch than in the upper arch (39). The evidence suggests that arch width increment proves more stable in the bicuspid regions and less predictable in the cuspid and second molar areas. Comparative studies demonstrate that increases in maxillary inter-cuspid, inter-premolar, and intermolar widths achieved significantly greater results among patients using optimized clear aligner protocols (32).
Adherence to suggested protocols improves treatment efficiency while maintaining conservative and biologically sound principles that slow expansion advocates promote (33).
Long-Term Outcomes and Stability
Long-term studies on slow expansion in adults consistently demonstrate lower relapse rates compared to RPE. Recent meta-analyses have revealed that 19.5% (95% CI: 15%-25%) of patients experienced a relapse of posterior crossbite during long-term follow-up (34). Slow expansion supports superior long-term retention of results, particularly when combined with appropriate retention protocols (35).
Williams' longitudinal data indicate that slow expansion in adults can achieve 80-90% of the results possible in growing patients, with significantly enhanced patient comfort and treatment acceptance. This evidence supports the expansion of this treatment option as a viable option for individuals of all ages, provided that correct protocols are followed (36).
*Authors Note:
Understanding 95% CI:
A 95% CI of 15%-25% demonstrates that the actual relapse rate of posterior crossbite in the population lies between 15% and 25%.
Statistical Interpretation:
- Point Estimate: 19.5% represents the observed relapse rate
- Confidence Interval: 15%-25% encompasses the range containing the actual population value
- Confidence Level: 95% probability that repeated studies would yield confidence intervals containing the actual population parameter
Clinical Significance:
Practitioners counseling patients about posterior crossbite correction should discuss:
- Expected outcome: Approximately 1 in 5 patients (19.5%) will experience relapse
- Potential variation: Relapse rates may range from 15% to 25%
- Research reliability: Strong statistical evidence (95% certainty) supports this range
Treatment Planning Implications:
Confidence intervals provide clinicians with research precision data. Narrow intervals (15%-25%) reflect precise estimates, whereas wide intervals suggest greater uncertainty.
This statistical convention in medical literature distinguishes between observed study findings (19.5%) and estimated population parameters (15%-25% range).
Clinical Decision-Making Algorithm

Future Directions and Emerging Technologies
Artificial Intelligence in Treatment Planning
AI-guided treatment planning systems now incorporate enamel thickness data from CBCT scans to optimize space management decisions, enhancing the precision of treatment planning. Machine learning algorithms can predict expansion success rates based on patient-specific anatomical factors.
Novel Expansion Techniques
• Micro-implant Supported Expansion (MSE): Shows promise for adult patients with mature sutures
• Miniscrew-Assisted Rapid Palatal Expansion (MARPE): Achieves skeletal expansion in post-adolescent patients
• Innovative Materials: Development of expansion appliances with built-in force regulation
Biomarkers for Treatment Prediction
Recent studies uncover genetic and biological markers that could predict individual responses to expansion therapy. This advancement sets the stage for developing personalized treatment protocols tailored to each patient's unique profile.
Digital Integration
Combining digital treatment planning with expansion methods helps predict space gains more accurately and ensures better coordination with clear aligner therapy.
Clinical Considerations and Treatment Planning
The successful implementation of expansion as a pre-aligner treatment requires careful patient evaluation and treatment planning. Patient age, skeletal maturity, degree of crowding, and facial morphology are essential considerations in determining the appropriateness of an expansion protocol.
Growing patients demonstrate an enhanced capacity for aggressive expansion protocols due to increased skeletal adaptation potential. Adult patients benefit from conservative approaches emphasizing dentoalveolar movement through slow expansion techniques. Integrating expansion with subsequent clear aligner therapy requires coordination between treatment phases to ensure optimal outcomes (37).
Recent systematic reviews have provided updated treatment planning guidelines, indicating that both clear aligners and traditional fixed appliances are effective in addressing simple malocclusions without the need for tooth extractions (38). However, additional high-quality studies are needed to clarify the use of clear aligners for treating complex malocclusions (39, 40, 41).
Conclusion
The expansion represents a valuable addition to the orthodontic armamentarium as a pre-aligner treatment. Recent systematic reviews and meta-analyses have strengthened the evidence base supporting expansion protocols. Preserving enamel integrity, enhancing facial aesthetics, improving functional parameters, and achieving better treatment outcomes make expansion a viable alternative to more aggressive space-gaining procedures.
While the relationship between crossbite correction and TMD prevention remains controversial, with limited high-quality evidence, expansion continues to offer significant benefits for occlusal function and facial aesthetics. Recent research has provided updated IPR safety guidelines that emphasize the importance of individualized treatment planning based on CBCT assessment of enamel thickness.
Continued refinement of expansion protocols and integration with modern aligner systems will improve treatment efficiency and patient acceptance. As orthodontic treatment evolves toward more conservative, biologically sound approaches, expansion will become an increasingly important component of treatment planning, supported by a growing body of high-quality evidence.
References
1. Proffit WR, Fields HW, Sarver DM, Ackerman JL. Contemporary Orthodontics. 6th ed. St. Louis: Elsevier; 2019.
2. Baneshi M, O'Malley L, El-Angbawi A, Thiruvenkatachari B. Effectiveness of clear orthodontic aligners in correcting malocclusions: A systematic review and meta-analysis. J Evid Based Dent Pract. 2025;25(1):102081.
3. Machado R, Moon W, Gandini LG Jr. Alternative treatment for class II malocclusion with severe crowding: Expansion and distalization. Dental Press J Orthod. 2018;23(6):26.e1-26.e11.
4. Adkins MD, Nanda RS, Currier GF. Arch perimeter changes on rapid palatal expansion. Am J Orthod Dentofacial Orthop. 1990;97(3):194-199.
5. Braun S, Hnat WP, Fender DE, Legan HL. The form of the human dental arch. Angle Orthod. 1998;68(1):29-36.
6. Cengiz SM, Goymen M. The effectiveness of orthodontic treatment with clear aligners in different thicknesses. Sci Rep. 2025;15:3958.
7. Sayahpour B, Eslami S, Schulz B, et al. The perception of facial esthetics about different buccal corridors and facial proportions. APOS Trends Orthod. 2025;15:49-58.
8. Nimbalkar S, Oh YY, Mok RY, et al. Smile attractiveness related to buccal corridor space in three different facial types: A perception study of three ethnic groups of Malaysians. J Prosthet Dent. 2018;120:252-256.
9. Roden-Johnson D, Gallerano R, English J. The Effects of Buccal Corridor Spaces and Arch Form on Smile Esthetics. Am J Orthod Dentofacial Orthop. 2005;127(3):343-350.
10. González-García E, Balut-Chahin N, Rojo-Arce CD, et al. Assessing Enamel Thickness to Estimate Interproximal Reduction: A CBCT-Based Study. Clin Exp Dent Res. 2025;11(1):e70083.
11. González-García E, Balut-Chahin N, Rojo-Arce CD, et al. Assessing Enamel Thickness to Estimate Interproximal Reduction: A CBCT-Based Study. Clin Exp Dent Res. 2025;11(1):e70083.
12. Zachrisson BU, Minster L, Øgaard B, Birkhed D. Dental health assessed after interproximal enamel reduction: caries risk in posterior teeth. Am J Orthod Dentofacial Orthop. 2011;139(1):90-98.
13. De Felice ME, Nucci L, Fiori A, et al. Accuracy of interproximal enamel reduction during clear aligner treatment. Prog Orthod. 2020;21(1):28.
14. Kau CH, Richmond S, Zhurov A, Ovsenik M, Tawfik W, Borbely P, English JD. Use of 3-dimensional surface acquisition to study facial morphology in 5 populations. Am J Orthod Dentofacial Orthop. 2010;137(4 Suppl):S56.e1-9.
15. Halazonetis DJ. Morphometrics for cephalometric diagnosis. Am J Orthod Dentofacial Orthop. 2004;125(5):571-581.
16. Bell RA, LeCompte EJ. The effects of maxillary expansion using a quad-helix appliance during the deciduous and mixed dentitions. Am J Orthod. 1981;79(2):152–161.
17. Ellabban MT, Abdul-Aziz AI, Fayed MMS, et al. Positional and dimensional temporomandibular joint changes after correction of posterior crossbite in growing patients: A systematic review. Angle Orthod. 2018;88(5):638-648.
18. Myllymäki A, Svedström-Oristo AL, Pirilä-Parkkinen K, et al. Longitudinal trends in temporomandibular joint disorder symptoms, the impact of malocclusion and orthodontic treatment: A 20?year prospective study. J Oral Rehabil. 2023;50:666-677.
19. Petrén S, Bjerklin K, Bondemark L. Tooth agenesis vs. extracted teeth in subjects with Class II Division 1 malocclusion treated with fixed appliances. Angle Orthod. 2013;83(5):776-781.
20. Garrett BJ, Caruso JM, Rungcharassaeng K, Farrage JR, Kim JS, Taylor GD. Skeletal effects on the maxilla after rapid maxillary expansion were assessed with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2008;134(1):8.e1-11.
21. Hariharan A, Muwaquet Rodriguez S, Hijazi Alsadi T. The Role of Rapid Maxillary Expansion in the Management of Obstructive Sleep Apnoea: Monitoring Respiratory Parameters—A Systematic Review and Meta-Analysis. J Clin Med. 2025;14(1):116.
22. Andrews LF. The six keys to normal occlusion. Am J Orthod. 1972;62(3):296–309.
23. Ballanti F, Lione R, Fanucci E, Franchi L, Baccetti T, Cozza P. Immediate and postretention effects of rapid maxillary expansion investigated by computed tomography in growing patients. Angle Orthod. 2009;79(1):24-29.
24. Handelman CS, Wang L, BeGole EA, Haas AJ. Nonsurgical rapid maxillary expansion in adults: report on 47 cases using the Haas expander. Angle Orthod. 2000;70(2):129-144.
25. Srivastava SC, Mahida K, Agarwal C, et al. Longitudinal Stability of Rapid and Slow Maxillary Expansion: A Systematic Review. J Contemp Dent Pract. 2020;21(9):1068-1072.
26. Rutili V, Mrakic G, Nieri M, et al. Comparison of rapid versus slow maxillary expansion on patient-reported outcome measures in growing patients: a systematic review and meta-analysis. Eur J Orthod. 2021;43(3):301-312.
27. Haas AJ. Long-term post-treatment evaluation of rapid palatal expansion. Angle Orthod. 1980;50(3):189-217.
28. Ramoglu SI, Sari Z. Maxillary expansion in the mixed dentition: rapid or semi-rapid? Eur J Orthod. 2010;32(1):11–18.
29. Lagravère MO, Major PW, Flores-Mir C. Long-term skeletal changes with rapid maxillary expansion: a systematic review. Angle Orthod. 2005;75(6):1046-1052.
30. Kravitz ND, Kusnoto B, BeGole E, Obrez A, Agran B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am J Orthod Dentofacial Orthop. 2009;135(1):27-35.
31. Effectiveness of maxillary arch expansion using clear aligners in adult patients: a systematic review and meta-analysis. Australas Orthod J. 2024;40(2):115-127.
32. Cengiz SM, Goymen M. The effectiveness of orthodontic treatment with clear aligners in different thicknesses. Sci Rep. 2025;15:3958.
33. Williams MO, Razmus TF. A long-term study of slow maxillary expansion compared to untreated controls. Semin Orthod. 2015;21(1):27-34.
34. Beltrami E, Antonarakis GS, Kiliaridis S. Long?term stability of posterior crossbite correction, treated in the mixed or permanent dentition of growing children: A systematic review and meta?analysis. Orthod Craniofac Res. 2024;27(1):1–14.
35. Brunetto M, Andriani Jda S, Ribeiro GL, Locks A, Correa M, Correa LR. Three-dimensional assessment of buccal alveolar bone after rapid and slow maxillary expansion: a clinical trial study. Am J Orthod Dentofacial Orthop. 2013;143(5):633-644.
36. Williams MO, Razmus TF, Gunel E. Long-term follow-up of slow maxillary expansion. Am J Orthod Dentofacial Orthop. 2012;141(6):758-789.
37. Chung CH, Font B. Skeletal and dental changes in the sagittal, vertical, and transverse dimensions after rapid palatal expansion. Am J Orthod Dentofacial Orthop. 2004;126(5):569-575.
38. Baneshi M, O'Malley L, El-Angbawi A, Thiruvenkatachari B. Effectiveness of clear orthodontic aligners in correcting malocclusions: A systematic review and meta-analysis. J Evid Based Dent Pract. 2025;25(1):102081.
39. Castro Aragon MLS, Ribeiro SMM, Fagundes NCF, Normando D. Effectiveness of dental arch expansion in the orthodontic treatment with clear aligners: a scoping review. Eur J Orthod. 2024;46(6):cjae059.
40. D'Antò V, De Simone V, Caruso S, et al. Effects of Clear Aligner Treatment in Growing Patients: A Systematic Review. Front Oral Health. 2025;5:1512838.
41. Kröger E, Dekiff M, Dirksen D, et al. Clear Aligner Treatment: Indications, Advantages, and Adverse Effects—A Systematic Review. Dent J (Basel). 2025;13(1):40..