A Quality Improvement Initiative to Reduce Unnecessary Antibiotic Utilization in a Tertiary Care NICU
A Quality Improvement Initiative to Reduce Unnecessary Antibiotic Utilization in a Tertiary Care NICU
Binoy Shah¹*, Dr Vaishali chudhary2, Dr Ashish Mehta3
*Correspondence to: Binoy Shah, Arpan Newborn Care Center, Ahmedabad, Gujrat, India.
Copyright
© 2025: Binoy Shah. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 Aug 2025
Published: 01 Sep 2025
DOI: https://doi.org/10.5281/zenodo.17090648
Abstract
BACKGROUND: Antibiotics are the most frequently used medications in the NICU. Such wide and sometimes unnecessary use can be deleterious and can lead to morbidities like necrotizing enterocolitis, bronchopulmonary dysplasia, late-onset sepsis, emergence of multi-drug resistance, adding unnecessary cost to patient and health care centres and also lengthens NICU stay. Antimicrobial stewardship is necessary to prevent the overuse of antibiotics.
AIMS AND OBJECTIVES: The aim of the study is to reduce AUR (Antibiotic Utilization Rate – primary outcome measure) by at least 30% of the baseline using antibiotic stewardship, over 4 months and to sustain this improvement for the next 2 months.
METHODS:
DESIGN: Quality improvement study
STUDY SITE: Neonatal Intensive care unit of Arpan new born care centre, Ahmedabad.
This quality improvement study aimed to reduce AUR by implementing anti-microbial stewardship. The study was carried out over 6 months with initial observation and then an intervention phase including nursing and fellow doctor education, timely de-escalation of antibiotics, thoroughly following hand hygiene, monthly review of AUR etc.
RESULTS: Following interventions, AUR was reduced to 356 per 1000 patient days from a baseline of 620 per 1000 patient days.
CONCLUSION: Antimicrobial stewardship for reducing unnecessary antibiotic utilization is effective, appears to be safe and results in a sustained and significant decrease in antibiotic utilization as in our centre.
A Quality Improvement Initiative to Reduce Unnecessary Antibiotic Utilization in a Tertiary Care NICU
Introduction
Antibiotics are most widely used medications in NICU. (1) Prolonged use of broad-spectrum antimicrobial in neonates can lead to invasive candidiasis, perturbation of microbiome (2) , necrotizing enterocolitis, late onset sepsis (3) and mortality. There is increasing evidence that prolonged antibiotic usage is associated with poor short-term neurodevelopmental outcomes. (4) Also, rapid surge in the emergence of the multi drug resistant organism can lead to prolonged hospital stay, increased duration of antibiotic therapy, and raise expenditure. (5) Overuse of antimicrobials during the neonatal period can lead to multi drug resistance. (6) Likelihood of isolating drug resistant organism from an individual is related to number and days of antibiotics to which the individual was exposed. (7) The prevention and management of MDR require a set of coordinated intervention, which are collectively termed as antimicrobial stewardship. In a simple terms AMS is the use of right antibiotic for the right indication on the right patient at the right time with the right dose and route causing the least harm to the patient and population. (8) The centre for Disease Control and Prevention recommended the implementation of antibiotic stewardship program in all acute care hospital and outlined seven core elements that are necessary for implementing the successful ASPs.(9) CDC advocates the use of checklist to systematically assess all the key elements and action to ensure the AMS in hospital. A dedicated staff should be assigned to ensure that the principles and action to improve antibiotic use remains in place. QI team can play a vital role in dosing QI studies and helping in the implementation of the AMS program. (10)
Summary of Core Elements of Hospital Antibiotic Stewardship Programs (9)
• Leadership Commitment: Dedicating necessary human, financial and information technology resources.
• Accountability: Appointing a single leader responsible for program outcomes. Experience with successful programs show that a physician leader is effective.
• Drug Expertise: Appointing a single pharmacist leader responsible for working to improve antibiotic use.
• Action: Implementing at least one recommended action, such as systemic evaluation of ongoing treatment need after a set period of initial treatment (i.e. “antibiotic time out” after 48 hours).
• Tracking: Monitoring antibiotic prescribing and resistance patterns.
• Reporting: Regular reporting information on antibiotic use and resistance to doctors, nurses and relevant staff.
• Education: Educating clinicians about resistance and optimal prescribing
Interventions to reduce antibiotic utilization: (9)
- Antibiotic time-outs
- Prospective audits and feedback
- Dose adjustments
- Dose optimization
- Time sensitive automatic stop orders
Our study used some of above-mentioned interventions to reduce antibiotic utilization and improve outcomes.
Aim
Global aim of the QI study is to reduce Antibiotic utilization rats in NICU and improve the outcomes.
The SMART aim of the study is to reduce AUR at least 30% of the baseline AUR in NICU over period of 4 months and to sustain this improvement for next 2 months.
Objectives
1. To increase awareness regarding unnecessary antibiotic usage amongst doctors and nursing staff
2. To reduce AUR in NICU and reduce unnecessary antibiotic usage
Materials and Methods
DESIGN: Quality improvement study
STUDY SITE: Neonatal Intensive care unit, Arpan newborn care centre, Ahmedabad.
Study population: Neonates of all gestational age, admitted in Arpan hospital including inborn as well as out born babies.
Study period: 6 months
Pre intervention phase: 2 months
Intervention phase: 4 months
STUDY TOOLS:
1. Baseline data of AUR collected from NICU review records and database.
2. To analyse root cause, fishbone analysis was used.
3. Unit’s antibiotic policy from protocols.
4. Regular educations sessions for nursing staff as well as for fellow doctors by means of presentations, posters, demonstrations.
5. Periodic audits by infection control team for compliance.
STUDY VARIABLES:
Outcome indicators:
Antibiotic utilization rate
AUR= total no of antibiotic days*1000/total no of patients
Antibiotic days are counted as total number of antibiotics to all patients at given time-point.
Process indicators:
- Compliance to teaching / education
- Hand hygiene audits
STUDY PROCEDURE:
Baseline AUR was calculated for three months.
STEP 1: Baseline data was collected for initial 2 months by keeping daily record of total antibiotic days and total number of patients between 15 October to 15 November and 1st dec to 31 dec, 2023. Data crossmatched with electronic data available with in charge of infection control team. Data was analysed and baseline AUR for the months of October - November and December.
|
AUR nov-oct |
AUR December |
|
639 |
620 |
STEP 2: Quality improvement team:
A QI team was formed including 6 members: one team leader ensuring changes are implemented correctly, one senior doctor for reviewing and discussing antibiotic policy of the unit amongst consultant and fellow, one head nurse ensuring implementation of changes at nursing staff level. One nursing in charge from all shifts, one person from infection control team for regular auditing compliance of nursing staff as well as doctors. Group discussion was held amongst team members, suggestions from team members were noted, solutions and suggestions were discussed.
STEP 3: Analysing the problem and measuring quality of care:
Current problem was analysed using fishbone diagram. Factors affecting problem were discussed and those having more impact will be addressed in intervention phase. Outcome indicators and process indicators were developed.
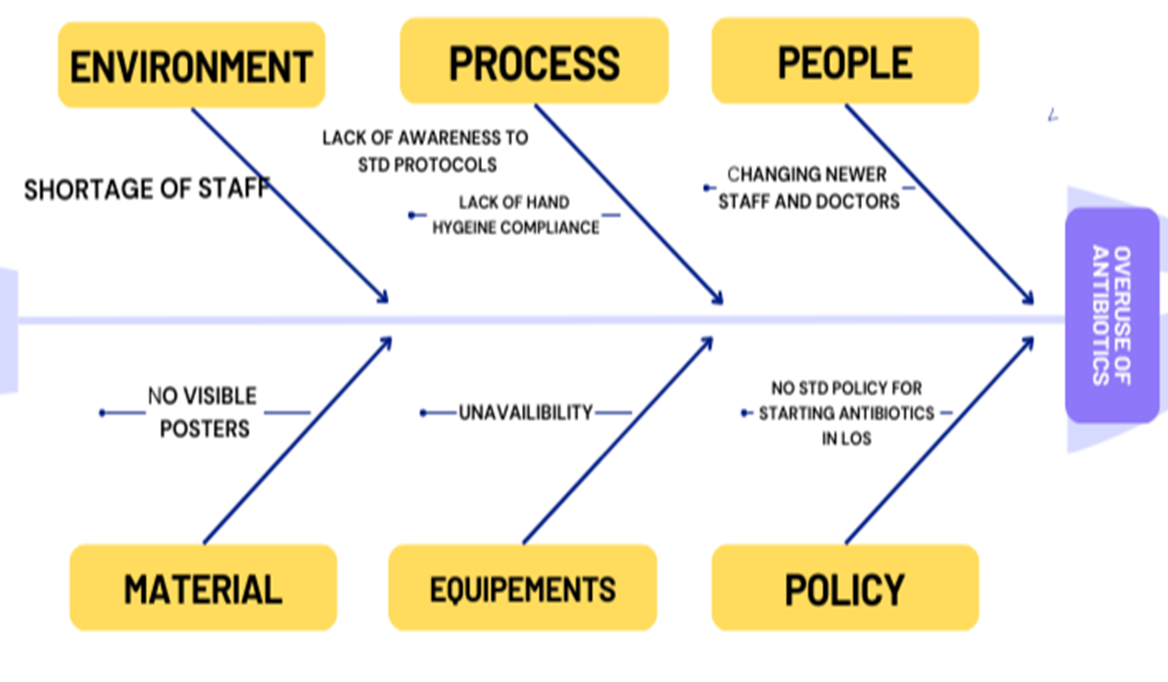
Fig 1
A fishbone diagram was sketched to identify possible areas of pitfall with respect to process, people, measures, equipment, material and environment. Diagram showed problematic areas like lack of awareness to the standard protocols, non-adherence to asepsis, periodically changing nursing staff and treating doctor, unnecessarily prolonging days of antibiotics etc.
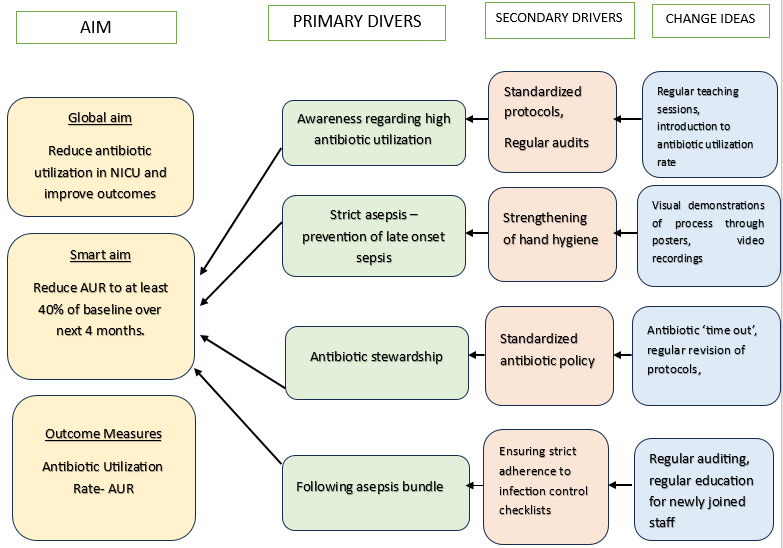
Fig 2
Study Flow- Intervention Phase
PDSA CYCLE 1: increasing awareness regarding antibiotic usage:
Introductory lectures were held for doctors as well as for nursing staff. Lectures included introduction antibiotic stewardship, unit policy for antibiotics, insisting everyone to enthusiastically take part in process.
PDSA CYCLE 2: education on hand hygiene:
Regular educative sessions were carried out for Nursing staff. This included presentation on importance of hand hygiene, indications, moments of hand hygiene, frequency of hand washing, ideal length of time for which hand washing to be done, presentation and demonstration of steps of hand hygiene. Attaching and drawing attention to posters related to hand hygiene in hand washing area. Regular auditing was done by infection control team in charge to ensure compliance to hand hygiene.
PDSA CYCLE 3: Drawing attention to antibiotic time out:
Monthly review of antibiotic utilization rate was done, last months’ AUR were written on white boards of both centres, to draw regular attention of treating doctors. This was to reminder about ‘antibiotic time-out’ i e discontinuing antibiotic at 48 hours, which were started for suspected sepsis as soon as culture results are available.
PDSA CYCLE 4: Revising infection control check lists
Regular educative sessions were carried out for doctors as well as nursing staff, also including newly joined staff and fellow doctors revising all infection control check lists used during various procedures like central line insertion, venous canula insertion, withdrawing blood cultures, ICD insertion, IV fluid preparation, injection preparation and injection, handling RT aspirates etc. particular insistence was given to follow every step in maintaining asepsis. Regular auditing was done during procedures ensuring there was no breech in sterile field during procedure.
Confidentiality
All the data and records generated through the course were kept confidential and study personnel will only have access to the data and records for the purpose of study.
Ethics
Permission from ethics committee was not required as ours was a quality improvement study.
Results
Outcome Indicator
|
|
AUR |
|
January |
884 |
|
February |
701 |
|
March |
368 |
|
April |
356 |
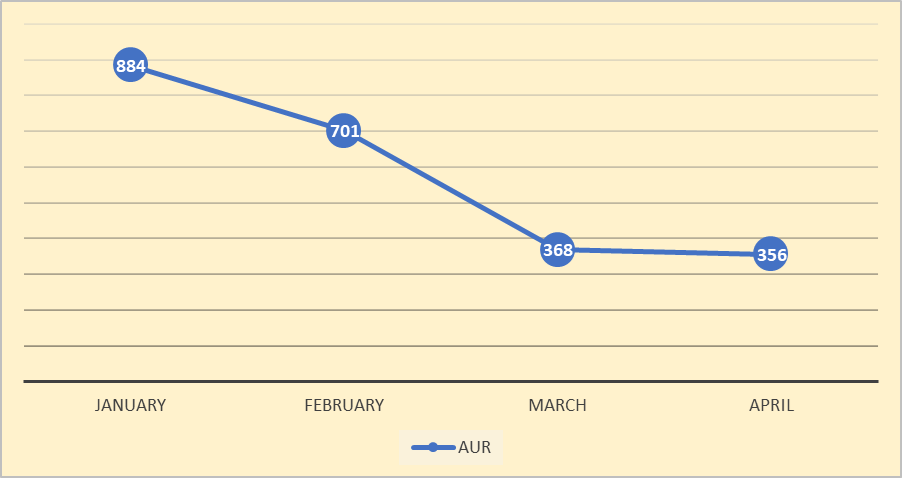
Monthly Review of antibiotic utilization rate was done. Following were the results over next four months in intervention phase. AUR significantly reduced over next four months.
Fig 3
Process indicators:
- Attendance in training sessions gradually improved over time.
- Compliance to hand hygiene improved during intervention phase as observed by infection control team.
No quantitative records were maintained for process indicators.
Sustaining The Improvement:
Improvement in antibiotic utilization rate was sustained over next two months.
|
Month |
AUR |
|
May |
338 |
|
June |
334 |
Discussion
In 1st PDSA cycle, doctors and nursing staff were made aware of high antibiotic utilization. They were introduced to antibiotic stewardship. Current NICU antibiotic policy was revised, discussed again with all doctors and staff. At the end of 1st PDSA cycle AUR increased from baseline of 620 to 884. So, the change might not have been effective. During same period, there was significant increase in number of admissions which were out born and also the surgical patients.
In 2nd PDSA cycle, emphasis was on hand hygiene through presentations, demonstrations, posters near handwashing area. Regular auditing to ensure compliance was done by infection control team in-charge. After this cycle, AUR decreased to 701. So, regular auditing and feedback was helpful here.
In 3rd PDSA cycle, which included drawing attention to antibiotic ‘time out’ – i e timely discontinuation as soon as negative culture results are available. Daily review of need of antibiotic in particular patient. Following this, AUR declined to 368.
In 4th PDSA cycle, which insisted on revising all infection control check-lists. This also was done through presentations, live demonstrations etc. Regular auditing for compliance was done by nursing in charge and team leader doctor. After this AUR declined to 356.
Our team by applying sequential and multidisciplinary approach, was able to reduce antibiotic usage to 40%, which exceeded initial goal of 30%. Implementations that are described in our study can be easily implemented at any other centre and successful results can be achieved. What worked most in our study in successfully decreasing AUR was nursing and fellow doctors’ education. As nursing staff I core of NICU, any change that is to be brought from ground level, should involve them. Another factor that helped in maintaining the changes was regular auditing and repeated reminder to ‘antibiotic time out’ to treating doctors. Regular communication with microbiology team regarding blood culture results so that patient do not receive unnecessary antibiotics.
Limitations
The initiative was able to reduce antibiotic utilization effectively. All healthcare workers were well aware of all protocols to be followed, still due to logistic issues and attitude of health care workers, they were not compliant enough. Using quality improvement approach, we decreased unindicated use of antibiotics. Although quantitative audits and feedbacks were not stressed upon during QI. Other than this, varying number of admissions per month might have affected antibiotic utilization rate.
Conclusion
Implementation of AMS brought effective and sustained decrease in utilization of antimicrobials at our centre. Every NICU should implement antibiotic stewardship programme which is also effective in low resource settings.
References
1. Graus JM, Herbozo C, Hernandez R, Pantoja AF, Zegarra J. Managing antibiotics wisely in a neonatal intensive care unit in a low resource setting. Journal of Perinatology. 2022 Jul 1;42(7):965–70.
2. Morales-Betancourt C, De la Cruz-Bértolo J, Muñoz-Amat B, Bergón-Sendín E, Pallás-Alonso C. Reducing Early Antibiotic Use: A Quality Improvement Initiative in a Level III Neonatal Intensive Care Unit. Front Pediatr. 2022 May 31;10.
3. Pantoja A, Sveum S, Frost S, Duran A, Burks J, Schernecke C, et al. New strategies to Reduce Unnecessary Antibiotic Use in the NICU: A Quality Improvement Initiative. Pediatr Qual Saf. 2023 May 7;8(3):E659–1987.
4. Ting JY, Shah PS. Antibiotic stewardship in neonates: Challenges and opportunities. Vol. 9, Translational Pediatrics. AME Publishing Company; 2020. p. 198–201.
5. Begnaud CM, Lemoine J, Broussard L, Rholdon R, Doshi H. A quality improvement project to reduce antibiotic utilization and ancillary laboratory tests in the appraisal of early-onset sepsis in the NICU. J Pediatr Nurs. 2021 Sep 1;60:215–22.
6. Fischer AM, Mitchell JL, Stanley KC, Javed MJ. A Quality Improvement Project to Reduce Antibiotic Exposure in Premature Neonates. Hosp Pediatr. 2023 May 1;13(5):435–42.
7. Konda KC, Singh H, Madireddy A, Poodari MMR. Quality improvement initiative approach to decrease the unindicated usage of antibiotics in a neonatal intensive care unit of a tertiary care teaching hospital in Hyderabad, India. BMJ Open Qual. 2021 Aug 3;10.
8. Rajar P, Saugstad OD, Berild D, Dutta A, Greisen G, Lausten-Thomsen U, et al. Antibiotic Stewardship in Premature Infants: A Systematic Review. Vol. 117, Neonatology. S. Karger AG; 2021. p. 673–86.
9. Department of Health U, Services H, for Disease Control C, Center for Zoonotic Infectious Diseases N, of Healthcare Quality Promotion D. CORE ELEMENTS OF HOSPITAL ANTIBIOTIC STEWARDSHIP PROGRAMS The Core Elements of Hospital Antibiotic Stewardship Programs [Internet]. Available from: http://www.cdc.gov/getsmart/healthcare/
10. Meyers JM, Tulloch J, Brown K, Caserta MT, D’Angio CT. A quality improvement initiative to optimize antibiotic use in a level 4 NICU. Pediatrics. 2020 Nov 1;146(5).