To Study the Clinical Profile of Stridor in the Pediatric Age Group at a Tertiary Care Pediatric Hospital.
To Study the Clinical Profile of Stridor in the Pediatric Age Group at a Tertiary Care Pediatric Hospital.
Dr. Nilesh Gundawar*
*Correspondence to: Dr. Nilesh Gundawar, MBBS, DCH, DNB, DCH(UK), MRCPCH (UK), FRCPCH (UK), IPPC (Sydney), FPIC. Senior Specialist, PICU/PCICU Al Jalila children’s Hospital, Dubai, UAE.
Copyright
© 2025: Dr. Nilesh Gundawar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 Aug 2025
Published: 01 Sep 2025
Abstract
Introduction: Stridor is a harsh, vibratory sound produced when the airway becomes partially obstructed, resulting in turbulent flow. Several anatomical and physiological features of the respiratory system in young children render them susceptible to airway obstruction.
Stridor is one of the life-threatening symptoms presenting to the Emergency Department. Stridor is a sign of airway obstruction, so it demands immediate attention and thorough evaluation to uncover the precise underlying cause.
Children with symptoms and signs of severe airway obstruction require urgent examination of the airway under anesthesia to determine the cause and secure the airway.
Viral croup (laryngotracheobronchitis) is responsible for more than 80% of cases of acute stridor in children. Since the introduction of Haemophilus influenzae type b vaccine, childhood epiglottis has become rare, making recognition and management more challenging.
There are very few studies which studied the clinical spectrum of the stridor in the pediatric age group. We carried out this study at Rainbow Children’s hospital and perinatal center, a tertiary care unit, in Hyderabad, to study the clinical spectrum of the stridor in pediatric age group. In our study we found that stridor is one of the most common presentation with the child comes to Emergency room and if diagnosed early can respond to treatment rapidly as compared to other treatable conditions.
Materials and Methods: Patients attending Pediatric Emergency and Pediatric Department were included in the study. After taking a detailed history and examination, direct laryngoscopy was done.
Results: 50 patients with stridor were studied. Of which, 20 (40.00%) cases were having congenital anomalies which was the most common cause for the stridor followed by 13 (26.00%) had post extubation stridor.
Conclusion: Most common cause of stridor in children includes post extubation stridor and acute laryngotracheobronchitis in acquired causes and laryngomalacia in congenital causes. They are more common in children of age less than two.
Keywords: Stridor, Laryngotracheobronchitis, Laryngomalacia, Direct Laryngoscopy.
To Study the Clinical Profile of Stridor in the Pediatric Age Group at a Tertiary Care Pediatric Hospital.
Methods
Inclusion Criteria:
1. All Pediatric population attending OPD and emergency room with history of stridor related to anatomical malformations were enrolled.
2. Pediatric cases who developed stridor during the course of hospital stay were also enrolled.
Exclusion criteria:
Respiratory distress due to medical diseases like asthma, cardiac, hematological causes.
A prospective study of 50 cases, between June 2011 to May 2012, done at Department of Pediatrics, Rainbow children’s hospital, Hyderabad, of pediatric age group patients, below 16 years of age presenting with respiratory distress suspected to be due to anatomical malformations of respiratory tract or obstruction of respiratory tract, to the Emergency department, Pediatric Outpatient department and Pediatric inpatient department. The primary management was to maintain the airway in all cases by intubation if respiratory distress is severe, intravenous line established, intravenous fluid /antibiotics/steroids/racemic adrenaline, followed by history of the respiratory distress from the parents/ caretakers as per preformed questionnaire. Then according to the provisional diagnosis evaluation is done with X-ray neck ap/lateral with chest/computerized tomography/magnetic resonance imaging. The various scopies performed are direct laryngoscopy/ flexible bronchoscopy/rigid bronchoscopy/ esophagoscopy. Tracheostomy was performed in few cases to bypass airway obstruction. Definitive treatment was instituted according to the diagnosis. At the end details were tabulated and analysis was done. The results were compared with the previous studies.
Results and Discussion:
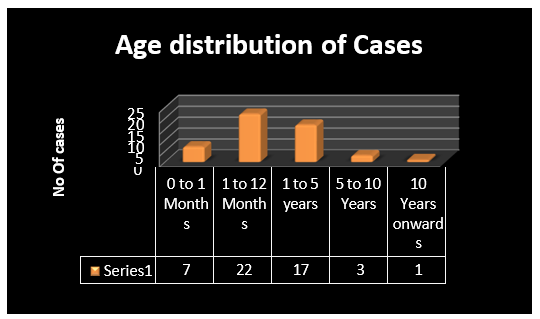
Graph 1: Graph depicting the Age Wise distribution of the cases studied.
Out of total 50 cases 29 (58%) of cases presented during first year of life, 17 (57.14%) had congenital etiology.
Out of 17 (35%) cases presented up to 5 years of age, 7 (41.17%) were having infectious etiology.
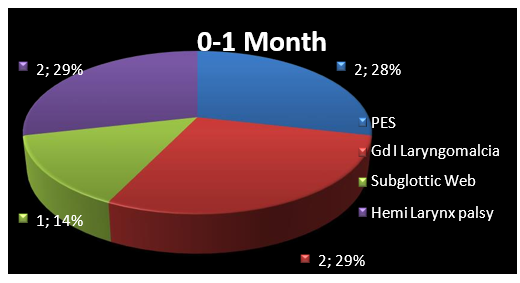
Graph 2: Graph depicting various etiological factors in the neonatal age.
Of the 7 cases, Hemi Laryngeal palsy (29%) along with the congenital malformations (29%) were more common amongst those who presented with stridor in early neonatal period.
Post Extubation Stridor/ PES (28%) is one of the important causes of the stridor in the neonatal age apart from the congenital causes.
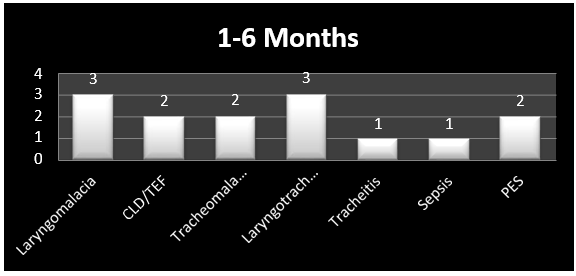
Graph 3: Graph depicting the causes of stridor in early infancy.
Out of 14 cases congenital causes remains the main etiology causing stridor, 8 (57.14%) were having congenital cause of stridor.
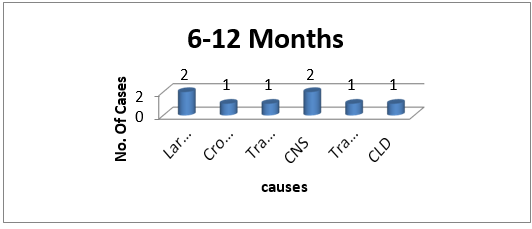
Graph 4: Graph depicting common causes of stridor amongst the late infancy.
3 (37.5%) cases out of 8 were having congenital cause of stridor.
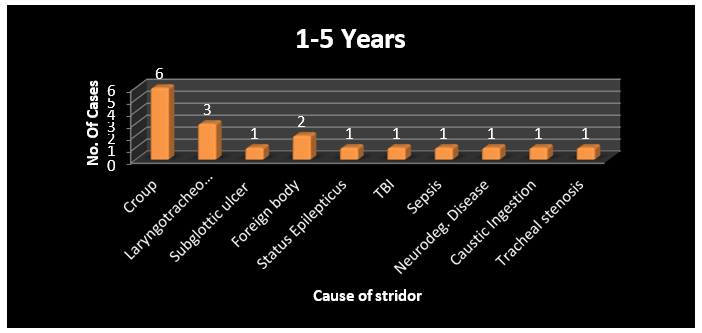
Graph 5: Chart depicting common causes of stridor amongst children of age 1-5 years.
Commonest cause of stridor amongst them was of infectious etiology 7 (41.17%) cases of the 17 cases had infectious etiology for the stridor, 6 of them were having croup and 1 child had Tracheitis.
Graph 6: Graph depicting causes of stridor amongst the cases
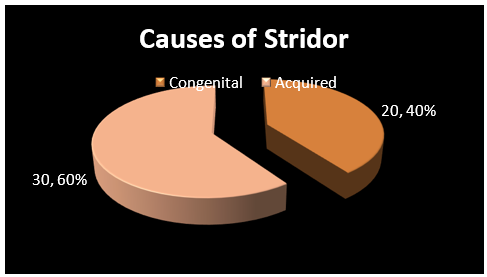
Our hospital being tertiary referral unit, most of the causes of stridor were acquired in origin (60.00%), 13 (26.00%) cases developed stridor as consequence of ventilation and 4 (8.00%) cases were having neurological stridor.
20 (40.00%) cases presented to us were having congenital causes.
|
Causes of stridor |
Number of cases |
|
Congenital |
20 (40.00%) |
|
Post Extubation Stridor |
13 (26.00%) |
|
Neurogenic |
3 (6.00%) |
|
Croup |
9 (18.00%) |
|
Foreign Body |
2 (4.00%) |
|
Lymphadenopathy |
1 (2.00%) |
|
Ingestion of caustic drain |
1 (2.00%) |
|
Epiglottitis |
1 (2.00%) |
Chart 1: Chart depicting common causes stridor
Out of 50 cases 20 (40.00%) cases were having congenital anomalies which was the most common cause for the stridor followed by 13 (26.00%) had post extubation stridor.
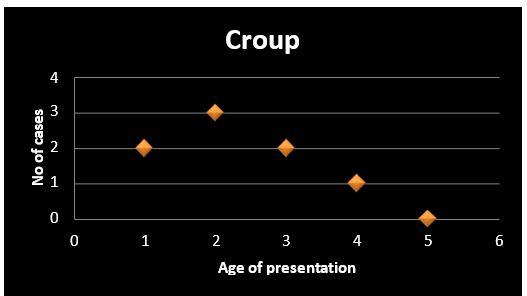
Graph 7: Graph depicting common age of presentation for croup
Out of 50 cases 9 (18%) cases were presented with signs and symptoms of croup which forms most important cause of cases with infectious etiology.
Most common age of presentation for croup is around 2 years of life. Most of the cases with croup presented in their 5 years of life.
Males are more affected as compared to females.
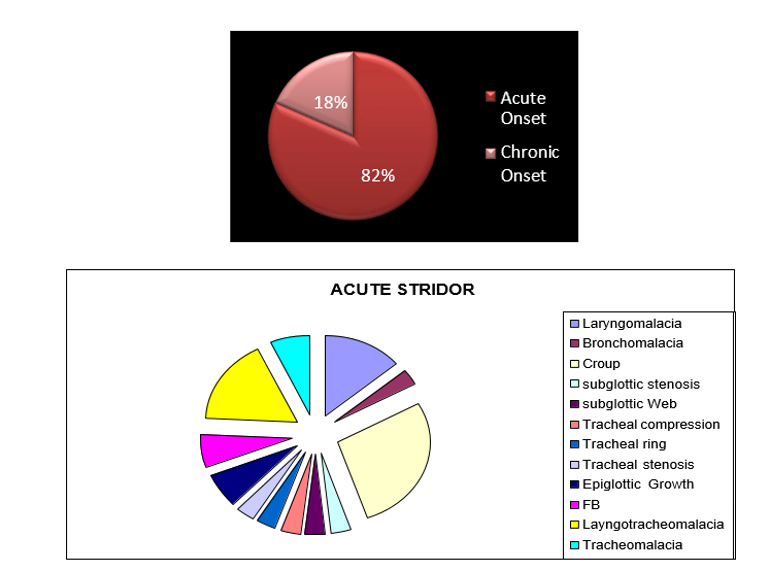
Graph 8: Graph depicting onset of the stridor and causes of acute stridor
Amongst 37 children who presented with the stridor 31(81.57%) presented with acute onset of stridor and rest 6 (18.43%) were having chronic nature of stridor.
Amongst 31 cases, 19 (61.29%) were having congenital causes and was the most important cause of acute stridor.
9 (29.03%) of cases were having infectious etiology- croup, causing acute stridor.
Discussion
Laryngomalacia is the most common cause of non-infective stridor in infancy. 1,2 It is diagnosed endoscopically by observing an abnormal prolapse of supraglottic structures during inspiration.3 Tracheomalacia as well causes chronic respiratory symptoms, mainly wheezing due to significant narrowing of the compliant trachea. 4,5 The most common finding in patients with tracheomalacia is a malformation of the cartilage rings, which causes the tracheal lumen to be oval rather than round. Laryngomalacia and tracheomalacia may coexist, but they have differences in etiology and pathophysiology. 6,7
In our study out of 50 cases enrolled 20 had congenital etiology for stridor. Amongst the congenital causes Laryngomalacia was most common amongst laryngeal causes and Laryngotracheomalacia was most common amongst the lower respiratory tract involvement. Out of 20 cases Laryngomalacia was found in 5 (25.00%), Laryngotracheomalacia was found in 5 (25.00%), Tracheomalacia was found in 3 (15.00%), Bronchomalacia was found in 1 (5.00%) & subglottic stenosis was found in 1 (5.00%) case.
In Neonates, out of 7 cases, Vocal cord palsy & Laryngomalacia were more common causing stridor and was present in 2 (10.5%) neonates amongst congenital causes, Post Extubation stridor was most common cause for the acquired etiology.
The most common causes of stridor at birth are laryngomalacia, congenital subglottic stenosis, VCP or vascular compression of trachea. The other causes are tracheomalacia, bronchomalacia and pressure effects of surrounding structures.8 In a case series evaluating cause of stridor in babies it was found that Laryngomalacia (19.4%) was the commonest congenital cause.9 In different case reports from India the other causes of stridor were tracheal duplication, Ductus Arteriosus aneurysm, subglottic cyst, tracheal and laryngeal agenesis and subglottic stenosis. 10-13
Vocal Cord Palsy accounts for 10-15% of causes of stridor. Bilateral VCP can cause biphasic stridor. Unilateral VCP is more common and is usually associated with birth injury, aberrant vessels and atrial enlargement. Bilateral VCP causes more severe symptoms and aphonia.14, 15 Often there is an associated neurological anomaly like Arnold Chiari malformation, intraventricular hemorrhage, meningoencephalocele and hydrocephalus. The other causes of VCP are traumatic forceps delivery, mediastinal surgery, and ligation of patent ductus arteriosus. However, most common cause of VCP is idiopathic.
Laryngeal webs, atresia, and stenosis result from failure of the epithelial tissue over the laryngotracheal groove to resorb by 10 weeks of gestation. While patients with these abnormalities are relatively uncommon in our study, patients with glottic webs and congenital subglottic stenosis have about a 50% likelihood of requiring tracheotomy.
In our study, amongst 20 cases, Males 13 (65.00%) outnumbered females 7 (35%) amongst congenital anomalies associated with the stridor.
|
Findings |
No of cases (n=20) |
Ken W Altman93 (n=174) |
Joshi et al118 (n=32) |
|
Laryngomalacia |
10 (50.00%) |
119(68.4%) |
13(40%) |
|
Tracheomalacia |
5(25.00%) |
42(24.1%) |
0 |
|
Bronchomalacia |
1(5.00%) |
18(10%) |
0 |
|
subglottic stenosis |
1(5.00%) |
12(6.9%) |
9(28.12%) |
|
subglottic web |
1(5.00%) |
15(8.6%) |
4(12.5%) |
|
Hemi Larynx Palsy |
2(10.00%) |
8(4.6%) |
5(15.62%) |
|
Tracheal Ring |
1(5.00%) |
0 |
0 |
|
Subglottic hemangioma |
0 |
2 (1.1%) |
0 |
|
Tracheal stenosis |
0 |
5 (2.9%) |
0 |
|
Tracheoesophageal Fistula |
2(10.00%) |
3 (1.7%) |
0 |
|
Tracheal web |
0 |
1 (0.6%) |
0 |
|
Tracheal agenesis |
0 |
1 (0.6%) |
0 |
|
Glottic or subglottic cyst |
0 |
3 (1.7%) |
0 |
|
Subglottic hemangioma |
0 |
2 (1.1%) |
0 |
|
Laryngeal stenosis or atresia |
0 |
2 (1.1%) |
0 |
Post Intubation Stridor:
Amongst acquired causes Post intubation stridor was most common cause for the stridor in pediatric age group in our study. Although it is very difficult to calculate the exact incidence of the post intubation stridor amongst pediatric age group.
|
Causes |
Our study (n=50) |
Rupa V et al 107 (n=180) |
|
|
|
Malacias, VCP, Subglottic stenosis, |
|
58 (32.2%) |
|
CONGENITAL – 20 (40%) |
20 (40%) |
|
|
|
|
Post Intubation Stridor |
|
122 (67.8%) |
|
ACQUIRED - 30 (60%) |
13(26%) |
|
|
|
Neurogenic |
4(8%) |
||
|
Croup |
9(18%) |
||
|
Foreign Body |
2(4%) |
||
|
Lymphadenopathy |
1(2%) |
||
|
Ingestion of caustic drain |
1(2%) |
||
As depicted in graph, 13 (26%) cases out of 50 cases were having post intubation stridor which is similar to previous studies 16, 17. Out of these 1 case developed tracheal stenosis and needed surgical intervention in the form of segmental tracheal reconstruction, on follow up he had repeated respiratory complaints although symptomatically he improved. 3 (23.07%) cases died during the hospital stay and 1 case went DAMA. 6 (46.15%) cases had history of Extubation failure most them were moribund and having underlying fulminant sepsis.
As depicted in graph 16, amongst 132 ventilated neonates only 2 (1.51%) developed post intubation stridor, whereas amongst 151 children who were ventilated in PICU 11(7.28%) developed post intubation stridor. 5 (38.46%) children less than 1 year were having post intubation stridor as compared to 8(61.53%) in the 1-4 years age group, so clearly indicating that the incidence increases with the advancing age up to 4 years. In the earlier series of post-intubation stridor after anesthesia, as reviewed by Koka et al., the incidence was reported as 1.6 - 6%.18 In Koka’s own series the incidence was low in infants, reached a peak in the 1–4 yrs age group, and then decreased as children grew older.
Bacterial tracheitis 8 (61.53%) was the most common in intubated cases and was one of the most important respiratory pathology causing life threatening emergency.
GERD & Tracheomalacia/Laryngomalacia:
Gastroesophageal reflux (GER) resulting in the aspiration of gastric content can cause an inflammatory reaction in the airways of infants and young children. This phenomenon is a relatively common cause of chronic pulmonary disease.19,20 This is particularly true in children with GER secondary to an immature swallowing mechanism, mental retardation, a seizure disorder, and neuromuscular disease. There is a relationship between GER and the chronic lung diseases cystic fibrosis, bronchopulmonary dysplasia, and asthma.21-23 A causal relationship has been found between GER and laryngomalacia11 and tracheomalacia. 24-28
In our study out of total 20 cases with congenital malformation, we found GERD to be associated with 7 (35%) cases, similar to 23%-53% found in other studies in patients with laryngomalacia 29,30. It is possible that gastro esophageal reflux is a factor that aggravates respiratory symptoms; however, it also may represent a concomitant, yet unrelated finding. Out of these 2 (28.57%) cases had Laryngomalacia and bronchomalacia, Laryngotracheomalacia, tracheomalacia & subglottic stenosis was present in 1 case each. Out of 7 cases, 1 case had recurrent chest infections.
In our study 4 (57.14%) cases out of 7 GERD cases under gone fundoplication in view of severity of the GERD.
BRONCHOSCOPY as a diagnostic tool:
Most infants with stridor require flexible direct laryngoscopy for diagnosis.31 Flexible fiber optic nasopharyngeal laryngoscopy is safe, allows detailed examination of nose, choanae, nasopharynx, oropharynx and hypopharynx.
During the study period 72 diagnostic bronchoscopies/laryngoscopies were done, most common indication for the direct laryngoscopy/bronchoscopy was evaluation of stridor done in 31 (43.05%) cases, followed by recurrent chest infiltrates on chest X-ray in 14 cases (19.44%).
Fiber optic bronchoscopy done under local anesthesia is the gold standard for the diagnosis of dynamic airway lesions . In our study, out of 50 patients enrolled 31 (62%) underwent bronchoscopy to ascertain the cause for stridor. As depicted in graph 9, 14 (45.16%) patients with stridor had dynamic airway lesions.
Dynamic compression of the left main bronchus had presented as obstructive hyper-aeration. It has been documented that severe bronchomalacia of the main bronchus acts as ball valve and produces hyper- aeration of lung (obstructive emphysema) 32. Impaired drainage of secretions caused by airway malacia results in backlog of secretions which may be responsible for the consolidation of the right upper lobe 33. In our study, out of 31 patients with recognizable etiology for stridor, 16 (51.61%) of them were having abnormal X ray findings, most common being hyperinflation of lung fields was found in 9 (56.25%) of them, collapse/ consolidation was found in 5 (31.25%) of them.
Laryngotracheobronchitis (CROUP):
Croup was present in 9 (18.36%) cases & was 2nd most common cause amongst the acquired causes. 6 (66.66%) cases presented before age of 3 years which correlates with the earliar studies. As per protocol if managed they respond very well to the treatment. The croup score at presentation and at end of 6 hours was significantly in favour of early treatment with the steroids.34,35,36
Klassen, et al.37 and Godden, et al. 38 found a significant reduction in croup scores at 4 hours and 2 hours with aerosolized budesonide in the treatment of children with croup, thus reiterating the sustained nature of the drug effect. The sustained effect of steroids is attributed to their anti-inflammatory effects, which are usually not apparent until 6 hours after treatment39. In our study, the croup score was significantly reduced after 4 hours of steroid treatment, although the end results could not be calculated as this was not part of ongoing study.
Most common presentation was stridor 9 (100%) followed by fever 8 (88.8%) and drooling of saliva 4 (44.4%). Leukocytosis was present in 8 (88.8%) cases with croup and strongly associated with croup. Mean duration of stay for mild to moderate stridor was 3 days as compared to 7 days for severe stridor. Only 1 (11.11%) case out of 9 needed PICU stay.
Croups occur annually in about 6% of children during their first 5 years of life. It accounts for about 2±3% of all hospital admissions for children (Denny et al., 1983; Hendrickson et al., 1997). A study in Belgium (Van Bever, 1999) found that 16% of children had suffered from croup, and 5% of children suffered from recurrent croup (i.e. they had three or more episodes). The condition is more common in atopic children.
Most children with crops have only mild symptoms. Only about 4% need to be hospitalized, and only one in 170 hospitalized children (one in 4500 of all children with croup) need to be intubated (Chapman, 1981; Marx et al., 1997). Dr Keith Hodgkin (Hodgkin, 1978) found that croup occurred in about 1 in 50 patients per year in his English general practice, mostly in their first 5 years of life.
The National Hospital Discharge Survey (Kozak et al., 2005) showed mean annual numbers of hospitalizations for a group of about 40 000, and 91% of hospitalizations occurred in children under 5 years of age. Boys get croup more often than girls, and a systematic review (Phelan et al., 1982) found that 72% of sufferers in croup trials were male. The annual incidence in children under 6 years of age ranged from 1.5% to 6%. The hospital admission rates for children with groups ranged from 1.5% to 31% of cases seen. These wide variations reflect differences in hospital admission practices and the severity of the condition in the population being assessed (Marx et al., 1997).
Conclusion
The management of stridor in pediatric age group is a teamwork of ENT surgeons, pediatrician, pediatric surgeons, anesthetist. The airway maintenance is the main management followed by ENT examination, evaluation by imaging, endoscopy and treatment of the cause. We follow the airway management algorithm in order to evaluate the child for diagnosis of the cause for treatment and successful outcomes of stidulous pediatric patients.
There is a need for more such studies emphasizing on proper upper airway evaluation and treatment protocols in tertiary care units.
Funding: No funding sources.
Conflict of interest: None declared.
Ethical approval: Not required.
References
1. Wood RE. Spelunking in the pediatric airway: exploration with the flexible fiberoptic bronchoscope. Pediatr Clin North Am 1984; 31:785–799
2. Solomons NB, Prescot CAJ. Laryngomalacia: a review and the surgical management for severe cases. Int J Pediatr Otorhinolaryngol 1987; 13:31–39
3. McSwiney PF, Cavanagh NPC, Languth P. Outcome in congenital stridor (laryngomalacia). Arch Dis Child 1977; 52:215–218
4. Benjamin B. Tracheomalacia in infants and children. Ann Otol Rhinol Laryngol 1984; 93:438–442.
5. Mair EA, Parsons DS. Pediatric tracheobronchomalacia and major airway collapse. Ann Otol Rhinol Laryngol 1992; 101:300–309.
6. Wood RE. Spelunking in the pediatric airway: exploration with the flexible fiberoptic bronchoscope. Pediatr Clin North Am 1984; 31:785–799
7. Mair EA, Parsons DS. Pediatric tracheobronchomalacia and major airway collapse. Ann Otol Rhinol Laryngol 1992; 101:300–309.
8. Fawehinmi Y, Fageeh N, Asindi A. Congenital Stridor as seen in a Neonatal Intensive Care Unit in Saudi Arabia. Niger J Pediatr 2002; 29: 11-13.
9. Rupa V, Raman R. Etiological profile of pediatric laryngeal stridor in an Indian hospital. Ann Trop Pediatr 1991; 11(2): 137- 141.
10. Sen MK, Mehta C, Chakrabarti S, Suri JC. Tracheal duplication as a cause of congenital stridor. Indian J Chest Dis Allied Sci 1999; 41(3): 159-162.
11. Jha D, Deka RC. Congenital supraglottic cyst: a rare cause of stridor. Indian J Pediatr 2000; 67(4): 311-312.
12. Das BB, Solowiejczyk DE, Kamath V, Sharma J. Congenital ductus arteriosus aneurysm presenting with stridor in a newborn. J Perinatol 2002; 22(2): 179-180.
13. Sarkar N, Agarwal R, Das AK, Atri S, Aggarwal R, Deorari AK. Congenital airway abnormalities in neonates. Indian J Pediatr 2002; 69(11) : 993-995.
14. Miller RH, Duplechain JK. Hoarseness and vocal cord paralysis. In Bailey BJ, Johnson JT, Kohut RI, Pillsbury HC, Tardy ME, eds. Head and Neck Surgery Otolaryngology Vol I. Philadelphia: J.B. Lippincott, 1993:620-629.
15. Berke GS. Voice disorders and phonosurgery. In Bailey BJ, Johnson JT, Kohut RI, Pillsbury HC, Tardy ME eds. Head and Neck Surgery-Otolaryngology Vol I. Philadelphia: J.B. Lippincott, 1993: 644-657.
16. Tellez DW, Galvis AG, Storgion SA, Amer HN, Hoseyni M, Deakers TW. Dexamethasone in the prevention of post-extubation stridor in children. J Pediatr 1991; 118: 289-293.
17. Kemper JK, Benson MS, Bishop MJ. Predictors of post-extubation stridor in pediatric trauma patients. Crit Care Med 1991; 19: 352-355
18. Koka BV, Jeon IS, Andre JM, McKay I, Smith RM. Postextubation croup in children. Anesth Analg 1977; 56(4): 501- 505.
19. Euler AR, Byrne WJ, Ament ME, et al. Recurrent pulmonary disease in children: a complication of gastroesophageal reflux. Pediatrics 1979; 63:47–51.
20. Spaulding HS Jr, Mansfield LE, Stein MR, et al. Further investigation of association between gastroesophageal reflux and bronchoconstriction. J Allergy Clin Immunol 1982; 69: 516–521.
21. Andze GO, Brandt ML, St. Vil D, et al. Diagnosis and treatment of gastroesophageal reflux in 500 children with respiratory symptoms: the value of pH monitoring. J Pediatr Surg 1991; 29:299–300.
22. Christie DI, O’Grady LR, Mack DV. Incompetent lower esophageal sphincter and gastroesophageal reflux in recurrent and acute pulmonary disease of infancy and childhood. J Pediatr 1978; 93:23–27
23. Malfroot A, Vandenplass Y, Verlinden M, et al. Gastroesophageal reflux and unexplained chronic respiratory disease in infants and children. Pediatr Pulmonol 1987; 3:208–213.
24. Balistreri WF, Farrel MK. Gastro esophageal reflux in infants. N Engl J Med 1983; 309:790–792.
25. Burton DM, Pransky SM, Katz RM, et al. Pediatric airway manifestations of gastro esophageal reflux. Ann Otol Rhinol Laryngol 1992; 101:742–749
26. Leonidas JC. Gastro esophageal reflux in infants: role of the upper gastrointestinal series. AJR Am J Roentgenol 1984; 143:1350–1351
27. Van den Abbeele T, Bruhier N, Narcy P. Severe laryngeal manifestations of gastro- esophageal reflux in children. Pediatr Pulmonol 1997; 16(suppl): 237–238.
28. Contencin P, Narcy P. Gastroesophageal reflux in infants and children: a pharyngeal pH monitoring study. Arch Otolaryngol Head Neck Surg 1992; 118:1028– 1030.
29. Belmont JR, Grundfast K. Congenital laryngeal stridor (laryngomalacia): etiologic factors and associated disorders. Ann Otol Rhinol Laryngol. 1984; 93: 430-437.
30. Holinger LD, Konior RJ. Surgical management of severe laryngomalacia. Laryngoscope. 1989; 99:136-142.
31. Benjamin BN, Gray SD, Bailey CM. Neonatal vocal cord paralysis. Head Neck 1993; 15(2): 169-172.
32. Mayer S, Laura N, Gerald Z, Joseph A. Pediatric intrathoracic large airway obstruction: Diagnostic and therapeutic considerations. Pediatr Emergency Care. 1994; 10:313-2.
33. Yalç1n E, Do ru D, Özçelik U, Kiper N. Airway malacia disorders in children. Chest. 2006; 130:304.
34. Husby S, Agertoft L, Mortenson S, Pedersen S. Treatment of croup with nebulized steroid (budesonide): a double bind, placebo controlled study. Arch Dis Child 1993; 63: 352-355.
35. Klassen P, Feldman E, Watters K, Sutcliffe T, Rowe C. Nebulized budesonide for children with mild-to-moderate croup. N Engl J Med 1994; 331: 285-289.
36. Godden CW, Campbell MZ, Hussey M, Cogswell JJ. Double blind placebo controlled trial of nebulized budesonide for croup. Arch Dis Child 1997; 76: 155-158.
37. Klassen P, Feldman E, Watters K, Sutcliffe T, Rowe C. Nebulized budesonide for children with mild-to-moderate croup. N Engl J Med 1994; 331: 285-289.
38. Husby S, Agertoft L, Mortenson S, Pedersen S. Treatment of croup with nebulized steroid (budesonide): a double bind, placebo controlled study. Arch Dis Child 1993; 63: 352-355.
39. Godden CW, Campbell MZ, Hussey M, Cogswell JJ. Double blind placebo controlled trial of nebulized budesonide for croup. Arch Dis Child 1997; 76: 155-158.