Bilateral Infiltrating Ductal Breast Carcinoma with Gastric Metastasis: A Rare Case
Dr Anusheel Anchal Vasnik 1*, Dr Pradeep Chandrakar 2, Dr. Vivek Choudhary 3
- Senior Resident, Radiation Oncology, Regional Cancer Center, Raipur.
- Professor, Radiation Oncology, Regional Cancer Center, Raipur.
- Professor and HOD, Radiation Oncology, Regional Cancer Center, Raipur.
*Correspondence to: Dr Anusheel Anchal Vasnik, Senior Resident, Radiation Oncology, Regional Cancer Center, Raipur.
Copyright.
© 2025 Dr Anusheel Anchal Vasnik, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 October 2025
Published: 01 November 2025
Abstract
Approximately 25% of female cancer cases are breast cancer in India, with high incidence between 25 yrs and 40 yrs. Bilateral breast cancer is usually rare and presence of gastric metastasis is even rarer. When such patients presents with signs and symptoms of metastatic disease as the chief complaint, it is very difficult to find out primary. We report a case of a forty-year-old woman, who presented with complains of dysphasia and vomiting after having meals since one month. Her Endoscopy and biopsy outside suggested gastric carcinoma. On Preliminary examination at our centre revealed that the patient has bilateral breast lumps with multiple lymph nodes in bilateral cervical and axillary regions. Multiple biopsies were taken and IHC was performed from both gastric and breast tissue which concluded our final diagnosis as infiltrating ductal carcinoma breast with gastric metastasis.
Keywords: breast, carcinoma, gastric, dysphagia, IHC, infiltrating ductal carcinoma.
Bilateral Infiltrating Ductal Breast Carcinoma with Gastric Metastasis: A Rare Case
1. Background
Metastatic breast carcinoma is quite frequent in Indian scenarios, especially among women from high socioeconomic strata. As per the ICMR data published in 2020, breast carcinomas account for 57%, only after cervix – uteri cancer (60%) of the total cancer burden in India.[1] In our institute, 10.68% patients of carcinoma breast have been registered in the last 10 years. Globally breast cancer is the commonest cancer in females and now has surpassed cervical cancer as the leading cause of global cancer incidence in year 2020, with an estimated of 2.3 million new cases, representing 11.7% of all cancer cases.[2] Over the last 26 years, the age-standardized incidence rate of BC in females increased by 39.1%, with the increase observed in every state of the country, from 1990 to 2016. [3,5] As per the Globocan data 2020, in India, breast cancer accounted for 10.6% (90408) of all deaths and 13.5% (178361) of all cancer cases.[4] Gastric metastasis from other sites is rare, but together with malignant melanoma and lung cancer, breast cancer seems to have the greatest capacity to metastasize in the gastrointestinal tract.[6] Radiological and endoscopic findings are nonspecific, and may be hard to distinguish from primary gastric cancer and non-Hodgkin’s lymphoma. In such conditions we need to rely on endoscopic guided biopsy with histopathology and immunohistochemistry for the final diagnosis.
2. Case Report
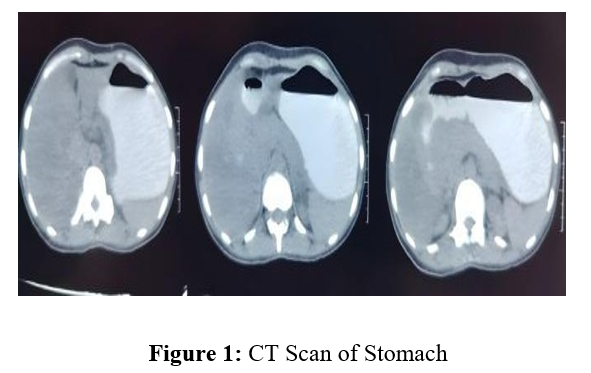
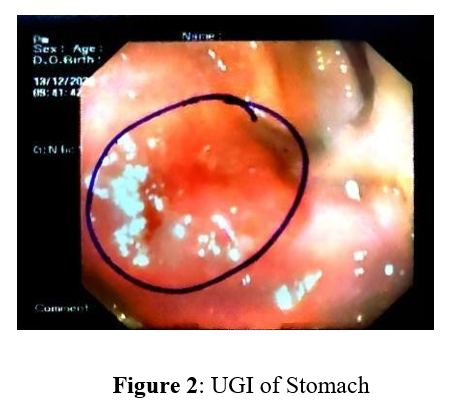
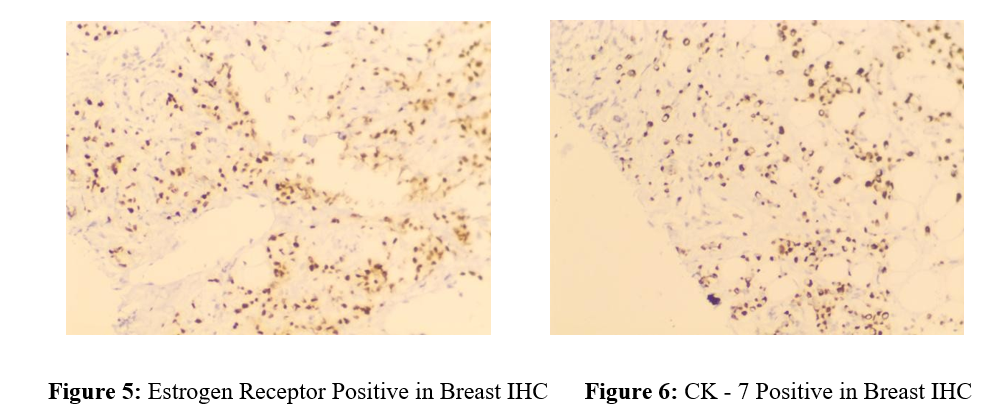
A forty-year-old female came with abdominal pain, vomiting after meals, fever and loss of appetite since six months. She went to a gastroenterologist, where endoscopy revealed ulcers in her stomach, with stricture in duodenum and sigmoid colon. Biopsy from stomach ulcers revealed diffuse infiltrating adenocarcinoma of signet ring phenotype. She was referred to our centre for further management as gastric cancer. On thorough clinical examination, well defined lump were found in both breast with multiple bilateral axillary lymph nodes. There were bilateral cervical, upper, middle, lower jugular and supraclavicular lymph nodes. Sonography also confirmed same finding. Her CECT scan of abdomen revealed circumferential thickening involving ileo – caecal junction and caecum with multiple para-aortic lymph nodes. Bilateral adenexa were bulky and non – enhancing. Lung showed no abnormality.
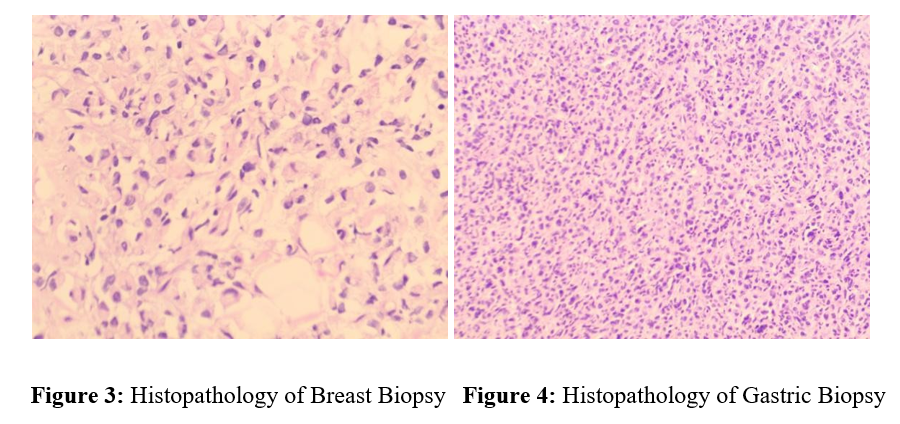
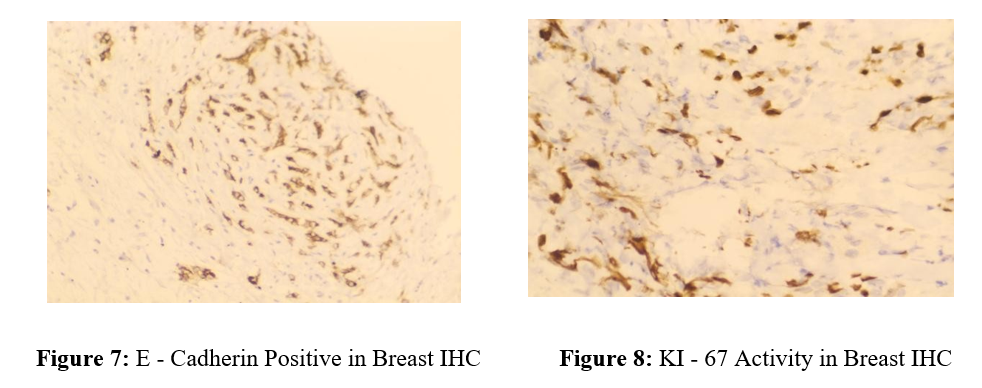
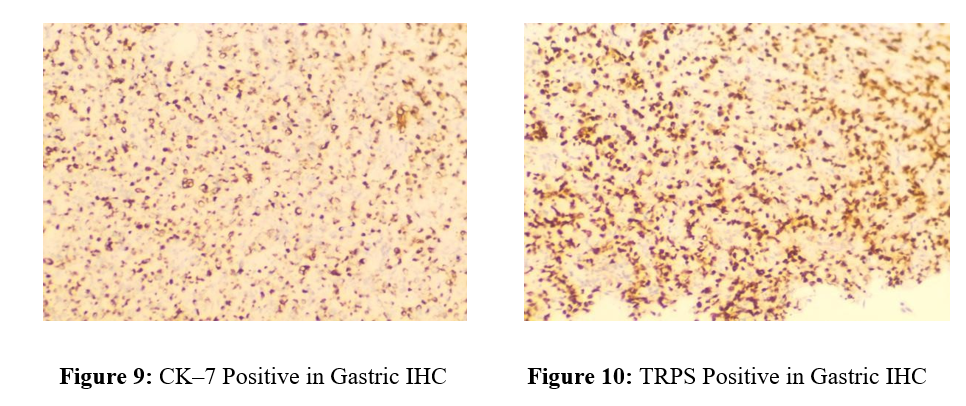
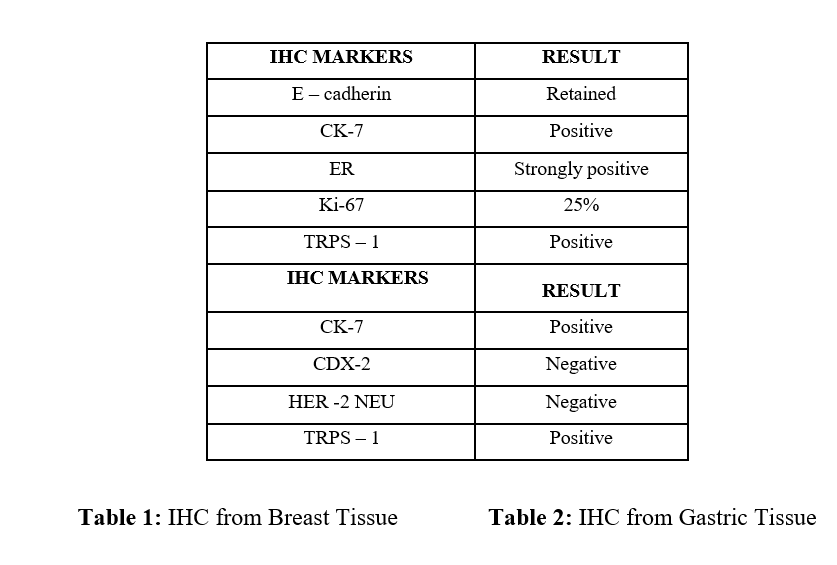
Biopsy from bilateral breast lumps and left axillary lymph node revealed invasive breast carcinoma with features highly suspicious of invasive lobular carcinoma. Due to unusual findings, IHC was sent. IHC from breast biopsy was positive for E-cadherin, CK-7, TRPS and Estrogen Receptors whereas Ki-67 was 25%. IHC from gastric biopsy was positive for CK-7 and TRPS but negative for CDX-2 and Her-2 Neu. Consequently, the diagnosis arrived as infiltrating ductal carcinoma breast with gastric metastasis. The patient was started on chemotherapy as metastatic breast cancer with injection albumin bound Paclitaxal (260mg/m2) and injection Carboplatin (AUC-6). The patient is under chemotherapy and doing better than before.
3. Discussion
Our patient was initially suspected as gastric carcinoma. After clinical evaluation and further investigations, it was finally concluded as breast carcinoma with gastric metastasis. It’s because carcinoma breast shows a similar picture of signet ring cells as primary gastric carcinoma which makes it difficult to diagnose. Furthermore primary gastric carcinoma can also metastasize to breast which can further complicate the diagnosis.[7] Only IHC finding has confirmed diagnosis.
The incidence of breast cancer metastasis to the stomach in long term follow up and postmortem cases has been estimated at 2-18%.[8]
Our patient presented with complains of anorexia, weight loss, vomiting after meals and abdominal pain which makes them indistinguishable from primary gastric carcinoma. XU et al, also confirmed that dull aching abdominal pain was most common symptom and localized to epigastric region which may mimic peptic ulcer disease and relives after eating. .[7] Gastric metastasis can occur synchronously with other sites of metastasis, so it’s very important to thoroughly examine the patients which may provide accurate diagnosis to the clinician.[9]
Our patient had diffuse infiltration of submucosa and muscularis propria giving a picture of linitus plastica in contrast enhanced CT scan, which is the most common pattern of breast cancer metastasis. Diffuse intramural infiltration imitating linitus plastica in gastric metastasis patients was reported to be 78% by Madeya and Borsch.[10] Our findings was consolidated by the findings of Cormeir et al, which concluded that linitus plastica is the most common pattern of involvement in gastric metastasis.[11].
On upper GI endoscopy, multiple ulcers were present in the stomach which coincide with the findings of Giovanni et al, where ulcerative lesion or polypoidal and extrinsic mass lesions were common findings.[12] Diagnostic imaging rarely helps the patient’s diagnosis. Upper GI endoscopy with deep biopsy is considered as the best modality to identify such metastasis. [6,12]
Our patient’s histopathology and IHC confirmed the diagnosis of infiltrating ductal carcinoma breast with gastric metastasis which is rare, as other studies show that gastric metastasis is more frequent with infiltrating lobular carcinoma (65.4%) than infiltrating ductal carcinoma (24.4%).[5] Taal et al, reported 83% patients of primary lobular carcinoma had gastric metastasis.[13] Borsch et al, observed there is distinct pattern of metastasis in both varieties. Infiltrating lobular carcinoma metastatize to gastrointestinal tracts, peritoneum, gynecological organs whereas infiltrating ductal carcinoma prefers lung, liver and bones making it much more unlikely.[10]
Morphologically, it is very difficult to distinguish between signet ring cell appearances of primary gastric carcinoma and breast carcinoma. However, CHU et al, observed breast signet-ring cell carcinoma may show some morphological differences from gastric and colonic signet-ring cell carcinoma. In breast a single, well-circumscribed univacuolated intra – cytoplasmic lumina, with a central eosinophilic inclusion were seen, whereas in other signet-ring cell carcinoma the cells have extended, globoid, and optically clear cytoplasmic acid mucin that pushes the nuclei against the cell membrane.[14]
In many studies, high percentage of metastatic breast carcinomas are positive for estrogen receptors- ER (72%), progestin receptors- PG (33%), for Gross Cystic Disease Fluid Protein GCDFP 15 (78%) and for cytokeratin 5/6 (61%), whereas primitive gastric cancers are negative for all these biological markers.[15,16,17]
IHC in breast biopsy was positive for estrogen receptors, CK-7 and TRPS whereas Ki-67 came out to be 25%. Also E-cadherin was retained proving it to be infiltrating ductal carcinoma breast. Whereas IHC on gastric biopsy was negative for CDX-2 and positive for CK-7 and TRPS – 1, proving that primary breast tumor and their metastases are phenotypically similar. Primary gastric carcinoma is more frequently positive for CK20 (50%), MUC 2 (54%), MUC5AC (71%), MUC 6 (39%), DAS-1 (43%) and CDX2 (67%) compared with metastatic breast cancer, which shows negativity for all these markers except MUC2, which is positive in 25% of cases. [15,16,17]
The type of therapy that is given to the patient depends upon the age, clinical presentation, availability of therapeutic options and quality of life discussion. A study by Mclemore et al reported the overall median survival of 28 months in 73 patients with gastrointestinal metastasis from breast cancer, also predicting treatment with chemotherapy or targeted therapy having a positive effect on survival whereas advanced age of diagnosis and gastric metastasis having a negative impact.[18]
Surgery being a debatable treatment option in such patients, is only reserved for solitary nodular lesion or in cases of obstruction, bleeding or perforation. Radiotherapy doesn’t have a major role either in such patients and is reserved for palliative management.
In conclusion gastric metastasis from breast cancer is rare. In such cases patients coming with primary gastric carcinoma should undergo a thorough clinical and radiological examination. Complete Histopathological and immunohistochemical analysis is required for the final diagnosis of metastatic breast carcinoma. Palliative and hormonal chemotherapy used in hormone positive breast carcinomas are the most helpful choices of treatment in such cases.
References
1. Mathur P, Sathishkumar K, Chaturvedi M, Das P, Sudarshan KL, Santhappan S, Nallasamy V, John A, Narasimhan S, Roselind FS, Icmr-Ncdir-Ncrp Investigator Group. Cancer statistics, 2020: report from national cancer registry programme, India. JCO global oncology. 2020 Jul;6:1063-75.
2. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians. 2021 May;71(3):209-49.
3. International Agency for Research on Cancer. India Source: Globocan 2020.[cited 11 June 2021].
4. Mehrotra R, Yadav K. Breast cancer in India: Present scenario and the challenges ahead.
World Journal of Clinical Oncology. 2022 Mar 3;13(3):209.
5. Madhav MR, Nayagam SG, Biyani K, Pandey V, Kamal DG, Sabarimurugan S, Ramesh N, Gothandam KM, Jayaraj R. Epidemiologic analysis of breast cancer incidence, prevalence, and mortality in India: Protocol for a systematic review and meta-analyses. Medicine. 2018 Dec;97(52).
6. Ismael AT, Jalal JA, Hussein S, Jawhar NM, Shafeek MY, Abdulrazaq R. Metastatic Breast Cancer to Stomach Mimicking Primary Gastric cancer. Innd 2 Hawler Pharmaceutical Sciences Conference: HPSC 2019 November 13-14, 2019 2019 Nov 13
(p. 60).
7. Boutis AL, Andreadis C, Patakiouta F, Mouratidou D. Gastric signet-ring
adenocarcinoma presenting with breast metastasis. World journal of gastroenterology: WJG. 2006 May 5;12(18):2958.
8. Jones GE, Strauss DC, Forshaw MJ, Deere H, Mahedeva U, Mason RC. Breast cancer metastasis to the stomach may mimic primary gastric cancer: report of two cases and review of literature. World Journal of Surgical Oncology. 2007 Dec;5(1):1-6.
9. Xu L, Liang S, Yan N, Zhang L, Gu H, Fei X, Xu Y, Zhang F. Metastatic gastric cancer from breast carcinoma: A report of 78 cases. Oncology letters. 2017 Oct 1;14(4):4069-77.
10. Madeya S, Börsch G. Gastrointestinal metastases of breast carcinoma. Gastrointest Endosc. 1993 Jan-Feb;39(1):103-4. doi: 10.1016/s0016-5107(93)70029-2. PMID: 8267696.
11. Cormier WJ, Gaffey TA, Welch JM, Welch JS, Edmonson JH. Linitis plastica caused by metastatic lobular carcinoma of the breast. InMayo Clinic Proceedings 1980 Dec 1 (Vol. 55, No. 12, pp. 747-753).
12. De Palma GD, Masone S, Rega M, Simeoli I, Donisi M, Addeo P, Iannone L, Pilone V, Persico G. Metastatic tumors to the stomach: clinical and endoscopic features. World journal of gastroenterology: WJG. 2006 Dec 12;12(45):7326.
13. Taal BG, Peterse H, Boot H. Clinical presentation, endoscopic features, and treatment of gastric metastases from breast carcinoma. Cancer: Interdisciplinary International Journal of the American Cancer Society. 2000 Dec 1;89(11):2214-21.
14. Chu PG and Weiss LM: Immunohistochemical characterization of signet-ring cell
carcinomas of the stomach, breast, and colon. Am J Clin Pathol 121: 884-892, 2004.
15. O'Connell FP, Wang HH, Odze RD. Utility of immunohistochemistry in distinguishing primary adenocarcinomas from metastatic breast carcinomas in the gastrointestinal tract. Archives of pathology & laboratory medicine. 2005 Mar 1;129(3):338-47.
16. Krishnamurthy S. Utility of immunohistochemistry in distinguishing primary
adenocarcinomas from metastatic breast carcinomas in the gastrointestinal tract. Breast Diseases. 2006;16(4):355-6.
17. Ghirarduzzi A, Sivelli R, Martella E, Bella M, De Simone B, Arcuri MF, Zannoni M, Del Rio P, Sianesi M. Gastric metastasis from breast carcinoma. Report of three cases,
diagnostic-therapeutic critical close examination and literature review. Annali Italiani di Chirurgia. 2010 Mar 1;81(2):141-6
18. McLemore EC, Pockaj BA, Reynolds C, Gray RJ, Hernandez JL, Grant CS, Donohue JH. Breast cancer: presentation and intervention in women with gastrointestinal metastasis and carcinomatosis. Annals of surgical oncology. 2005 Nov;12:886-94.