Injury Pattern of Pediatric Trauma in an Integrated Trauma Center in UAE
Injury Pattern of Pediatric Trauma in an Integrated Trauma Center in UAE
Mumtaz Ibrahim1* ,Nadeem Haider1 , Amer Kiani1, Nejamaldin Kheber1, Alhasan Ahmed Al-fikri2, Bashir Saddig2 , Ammar Al-Mashhadi1,3
1 Sheikh Khalifa Medical City, Ajman, UAE.
2 Ajman University, Ajman, UAE.
3 Department of Women's and Children's Health, Uppsala University, Sweden.
*Correspondence to: Mumtaz Ibrahim, Department of Surgery, Sheikh Khalifa Medical City Ajman, United Arab Emirates.
Copyright
© 2025 Mumtaz Ibrahim. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 April 2025
Published: 07 May 2025
DOI:https://doi.org/10.5281/zenodo.15387860
Abstract
Background: Injury is an important cause for morbidity and mortality in the pediatric population and exhibits complex injury patterns in this age group.
Objective: Identify the injury pattern of children admitted to Sheikh Khalifa Medical City, Ajman.
Research Methodology: A retrospective review of pediatric trauma. This study includes 507 pediatric trauma patients. The data included information on demographics, mechanism of injury, pattern of injury, hospitalization period, ICU stay, Glasgow Coma Scale, treatment modality and 30-day mortality. Data was entered and analyzed using SPSS version 25.0.
Result: Among 507 pediatric trauma patients, 71.4% were males and the mean age was 5.42+3.625 years. Majority of the patients experienced. Falls were the most common mode of injury (54.6%) followed by road traffic accidents (26.6%). Head was involved in 54.0% patients. Hospital admission and treatment was required by 18.3% patients. The mean hospital stay was 2.91+9.729 days and 30-day mortality was 0.6%.
Conclusion: This study concluded that majority of injuries occurred due to falls among male pediatric patients aged between 4 to 8 years.
Keywords: Injury, pediatric, trauma, mechanism, region involved, mortality.
Injury Pattern of Pediatric Trauma in an Integrated Trauma Center in UAE
Introduction
The pediatric trauma is linked to significant morbidity as well as mortality;[1] and remains a public health care issue worldwide. The traumatic injuries due to all causes result in 8.4 to 9.3 percent mortality among children.[2] According to WHO more than 6 million children aged less than 15 years die from injuries per year.[3] In America, about one-third of pediatric population (22 million children) experience injuries of various types, every year. In the European Union, about 6000 children (0–14 years old) die annually as a result of injuries.. Trauma is responsible for 21.26% pediatric injuries in China with death rate 28.12 / 100,000 children.[4] Considering the premature death burden and the years lived along with disabilities, the common injuries in this population are among significant causes of DALYs (disability adjusted life-years).[5] The non-fatal injuries also cause long hospital stays and could have long-term economic as well as societal consequences regarding disability rehabilitation, care responsibility and earnings loss.[6]
The pattern and causes for pediatric injuries are influenced by patient age, sex, socio-economic as well as environmental factors. Among children, injuries occur due to several reasons such as RTAs (road traffic accidents), falls from the height at home or in playground, burn and during delivery.[7] Road accidents, drowning, falls, burns and poisoning are responsible for 60% of all mortalities caused by pediatric trauma.[2]
A study carried out by Cintean et al. (2023) assessed epidemiology, patterns as well as mechanisms for pediatric trauma. During study 12,508 children were included. Amongst his patients, 2924 sustained lacerations & superficial tissue injury, 2703 had fractures, 320 joint dislocations, 5151 bruises, 76 burns, 1284 distortions and 50 other kinds of injuries were managed. Most common reasons regarding fractures were falls, sports-related and leisure activities. Among 700 children who experienced fractures, 25.9% required surgery. Among all patients, 8.8% were hospitalized for one day and the in-hospital mortality rate was 0.03%.[8]
A study conducted by Sadoway and teammates (2024) demonstrated that out of 1258 injuries, the pediatric trauma rate was 41.7 / 100,000. The blunt trauma was responsible for 86.2 percent of injuries while motor vehicle accidents were most commonly observed cause (35.6%). The mortality rate among patients was 17.2%.[9]
Almalki and fellows (2023) undertook a study to evaluate the epidemiology for pediatric trauma in Makkah. During study children aged up to 14 years were enrolled. Falling from the height was most commonly observed injury mode in both genders (41.8%). In most cases, children were admitted to surgical ward (75.7%) and others were treated in emergency room without admission (15.4%).[10]
A study undertaken by Su and coworkers (2024) included 4568 underage trauma patients (3093 males and 1475 females). Among patients aged between 0-6 years, the maximum number of injuries was noticed. Falls were the major trauma cause, responsible for 52.78 percent. With regards to main injured body parts, limbs and skin were most commonly affected (60.22%), followed by, head and neck region (32.03%).[11]
As the trauma burden, pattern, mode and site of injury, as well as outcome varies from region to region and also in the different age groups, it is essential to understand these characteristics to formulate effective injury prevention strategies.[12] Therefore, current study was carried out to identify the injury pattern of children admitted to Sheikh Khalifa Medical City, Ajman.
Materials and Methods
A retrospective review of pediatric trauma. During study 507 pediatric trauma patients were included. The data was obtained from Trauma Registry of Sheikh Khalifa Medical City, Ajman between the period from 01 January 2018 to 31 December 2023.
Inclusion Criteria:
- All pediatric patients aged 0-13 years, following trauma admitted to the Pediatric Unit or PICU.
Exclusion Criteria:
- Severely injured patients who died at the scene of injury or arrived dead to the hospital.
- Patients with mild injuries who were treated and discharged from the Emergency Department.
Data Collection:
The data was collected from the health information system (HIS) available in the hospital. The data was collected regarding variables such as demographic, mechanism of injury, pattern of injury, hospitalization period, ICU stay, Glasgow Coma Scale, treatment modality (conservative or surgery) and 30-day mortality.
Data Analysis:
The collected data was analyzed statistically using SPSS (Statistical Package for Social Sciences) version 25.0. For quantitative variables mean and standard deviation (SD) were calculated and for qualitative variables, frequency and percentages were calculated. Data was presented in tables and graphs for both quantitative and qualitative variables. Chi-square test was used to estimate the association between age and injury patterns. P-value <0.05 was considered significant.
Results
Table-1 demonstrates that among 507 pediatric trauma patients, 192 (37.9%) were 0-3 years old, 201 (39.6%) were 4-8 years old and 114 (22.5%) were 9-13 years old while the mean age was 5.42+3.625 years. Out of 507 patients, 362 (71.4%) were males and 145(28.6%) were females.
Table-2 depicts that among 507 patients, majority experienced fall 277(54.6%), followed by, RTA 135(26.6%), MVA 31(6.1%), MVC 27(5.3%), burns 16(3.2%), unclear mechanism 13(2.6%) and assault 8(1.6%).
Among our cohort of patients, head was involved in 275(54.0%), followed by, face 70(13.8%), upper extremity 58(11.5%), abdomen 45(8.9%), chest 27(5.3%), lower extremity 20(3.9%) and back 13(2.6%). Sixty-five patients (12.8%) were admitted to PICU while majority 442 (87.2%) were managed on the pediatric ward.
The table also highlights those 15 patients (2.9%) had GCS score 3-8 and 12 (2.4%) had a score between 9-12 while most of the patients had GCS score 13-15. The mean GCS score of patients was 14.50+1.885. Out of 507 patients, 414 (81.7%) received conservative treatment while 93 (18.3%) required surgical treatment.
The mean hospital stay of patients was 2.91+9.729 days. However, the majority 459 (90.5%) of the patients had hospital stay 1-5 days and 35 patients (6.9%) stayed between 6-10 days while 13 (2.6%) patients had hospital stay of more than 10 days.
Amongst our group of patients, 25(4.9%), 271(53.5%) and 211(41.6%) had L1, L2 and L3 trauma levels, respectively.
Result shows that among the 507 patients, the 30-day mortality was 3(0.6%) while the remaining significant proportion 504(99.4%) had no 30-day mortality.
Table-3 indicates the correlation between injury pattern and child’s age. Among 192 patients who were 0-3 years old, 2 experienced assaults (how can a 2 year old be assaulted?), 11 burns, 4 unclear Mechanism, 138 fall, 9 MVA, 7 MVC and 21 patients experienced RTA. Among 201 patients who were 4-8 years old, 4 experienced assaults, 3 burn, 5 mix????, 90 fall, 12 MVA, 14 MVC and 73 patients experienced RTA. Among 114 patients who were 9-13 years old, 2 experienced assaults, 2 burns, 4 unclear Mechanism, 49 fall, 10 MVA, 6 MVC and 41 patients experienced RTA. The result was found statistically significant (P=0.000).
Table further revealed that among 192 patients who were 0-3 years old, the region involved was abdomen, back, chest, upper extremity, face, head and lower extremity for 10, 2, 10, 15, 18, 130 and 7 patients, respectively. For the 201 patients who were 4-8 years old, abdomen, back, chest, upper extremity, face, head and lower extremity were involved 20, 6, 9, 22, 33, 100 and 11 patients, respectively. Among the 114 patients who were between the age of 9-13 years old, the region involved was abdomen, back, chest, upper extremity, face, head and lower extremity for 15, 5, 8, 21, 19, 44 and 2 patients, respectively. The result was found statistically significant (P=0.000).
Table-1: Demographic data
|
|
Frequency |
Percentage |
|
Age |
||
|
0-3 years |
192 |
37.9 |
|
4-8 years |
201 |
39.6 |
|
9-13 years |
114 |
22.5 |
|
Total |
507 |
100.0 |
|
Mean+SD |
5.42+3.625 |
|
|
Gender |
||
|
Male |
362 |
71.4 |
|
Female |
145 |
28.6 |
|
Total |
507 |
100.0 |
|
Nationality |
||
|
Emirati |
224 |
44.1 |
|
Non-Emirati |
283 |
55.9 |
|
Total |
507 |
100.0 |
Figure-1: Gender
Figure-2: Nationality
Table-2: Injury pattern
|
|
Frequency |
Percentage |
|
Mechanism of injury |
||
|
Assault |
8 |
1.6 |
|
Burn |
16 |
3.2 |
|
Unclear mechanisms |
13 |
2.6 |
|
Fall |
277 |
54.6 |
|
MVA (Motor Vehicle Accident) |
31 |
6.1 |
|
MVC (Motor Vehicle Collision) |
27 |
5.3 |
|
RTA (Road Traffic Accident) |
135 |
26.6 |
|
Total |
507 |
100.0 |
|
Region involved |
||
|
Abdomen |
45 |
8.9 |
|
Back |
13 |
2.6 |
|
Chest |
27 |
5.3 |
|
Upper extremity |
58 |
11.5 |
|
Face |
70 |
13.8 |
|
Head |
274 |
54.0 |
|
Lower extremity |
20 |
3.9 |
|
Total |
507 |
100.0 |
|
PICU admission |
||
|
Yes |
65 |
12.8 |
|
No |
442 |
87.2 |
|
Total |
507 |
100.0 |
|
GCS |
||
|
3-8 |
15 |
2.9 |
|
9-12 |
12 |
2.4 |
|
13-15 |
480 |
94.7 |
|
Total |
507 |
100.0 |
|
Mean+SD |
14.50+1.885 |
|
|
Treatment modality |
||
|
Conservative |
414 |
81.7 |
|
Surgery |
93 |
18.3 |
|
Total |
507 |
100.0 |
|
Hospital stay |
||
|
1-5 days |
459 |
90.5 |
|
6-10 days |
35 |
6.9 |
|
>10 days |
13 |
2.6 |
|
Total |
507 |
100.0 |
|
Mean+SD |
2.91+9.729 |
|
|
Trauma level |
||
|
L1 |
25 |
4.9 |
|
L2 |
271 |
53.5 |
|
L3 |
211 |
41.6 |
|
Total |
507 |
100.0 |
|
30-Day Mortality |
||
|
Yes |
3 |
0.6 |
|
No |
504 |
99.4 |
|
Total |
507 |
100.0 |
Figure-3: Mechanism of injury
Table-3: Correlation between injury pattern and child’s age
|
|
Age groups |
Total |
||
|
0-3 years |
4-8 years |
9-13 years |
||
|
Mechanism of Injury |
||||
|
Assault |
2 |
4 |
2 |
8 |
|
Burn |
11 |
3 |
2 |
16 |
|
Unclear mechanisms |
4 |
5 |
4 |
13 |
|
Fall |
138 |
90 |
49 |
277 |
|
MVA |
9 |
12 |
10 |
31 |
|
MVC |
7 |
14 |
6 |
27 |
|
RTA |
21 |
73 |
41 |
135 |
|
Total |
192 |
201 |
114 |
507 |
|
P-value = 0.000 |
||||
|
Region involved |
||||
|
Abdomen |
10 |
20 |
15 |
45 |
|
Back |
2 |
6 |
5 |
13 |
|
Chest |
10 |
9 |
8 |
27 |
|
Upper extremity |
15 |
22 |
21 |
58 |
|
Face |
18 |
33 |
19 |
70 |
|
Head |
130 |
100 |
44 |
274 |
|
Lower extremity |
7 |
11 |
2 |
20 |
|
Total |
192 |
201 |
114 |
507 |
|
P-value = 0.000 |
||||
Discussion
Injury is an important cause for morbidity and mortality in pediatric population and exhibits complex injury patterns. Present study was carried out to identify the injury pattern among children admitted to Sheikh Khalifa Medical City, Ajman. To acquire appropriate outcomes, a group of 507 pediatric trauma patients was included in the study and found that most of the patients were 0-8 years old and the mean age of patients was 5.42+3.625 years. A similar study carried out by Jones and coworkers (2019) showed almost comparable results that mean age of the patients was 6.4+5.2 years.[12] But the results of another study conducted by Alansari and associates (2023) indicated that mean age of pediatric trauma patients was 9.3 years.[2]
Majority of the patients were males (71.4%).The results of a study undertaken by Kunwar and collaborators (2020) also confirmed that most of the patients (58.2%) were males and 41.8% were female patients.[13] This is mostly thought to be due to the more active and aggressive nature of male subjects.
Among these trauma patients, majority experienced fall (54.6%), followed by, RTA (26.6%), MVA (6.1%), MVC (5.3%), burn (3.2%) and assault (1.6%). The results of a study performed by Dagnaw and teammates (2022) highlighted that most prevalent causes of trauma were falls (37.3%) and road traffic accidents (24.2%).[14]
A study by Yaseen et al (2023) indicated that injury pattern among 54.4%, 31.1%, 9.0%, 3.3% and 2.2% patients were road traffic injuries, falls from height, poisoning, burns and electrocution, respectively.[3] In their study Fylli et al. (2023) reported that among pediatric trauma patients the most prevalent cause was head injury (64.3%).[15]
A recent study undertaken by Su and comrades (2024) elucidated that falls were the most significant cause for pediatric trauma (52.8%).[11]
The findings of our study further revealed that among majority of patients, the region involved was head (54.0%), followed by, face (13.8%), upper extremity (11.5%), abdomen (8.9%), chest (5.3%), lower extremity (3.9%) and back (2.6%).
In a study, Alansari and companions (2023) reported that the most commonly region involved was head (38.8%), followed by, chest (19.9%), abdomen (13.0%), pelvis (10.3%), upper extremity injury (15.7%) and lower extremity (18.6%).[2]
Almalki and colleagues (2023) asserted that most involved body parts were extremities (59.0%), followed by, head (34.7%), chest (9.4%), neck (5.1%), pelvis (4.5%), abdominal organs (4.1%), back (2.3%) and eye (1.5%).[10]
It is important to mention here that majority (94.7%) of patients had GCS score 13-15 (mild), 2.4% patients had 9-12 (moderate) and only 2.9% patients had a score between 3-8 (severe).
A virtual study by Alansari and associates (2023) exhibited similar findings that most of the patients (85.7%) had GCS score 13-15 (mild), 4.2% patients had 9-12 (moderate) and 10.1% patients had 3-8 (severe).[2]
Only 12.8% of pediatric patients in our group required PICU admissions compared to work by Onyemaechi and partners (2020) where only 8.3% of patients required ICU admission.[7] Another study undertaken by Almalki and colleagues (2023) indicated that only 5.3% pediatric patients required ICU admission.[10]
Majority (53.5%) had level 2 trauma while 4.9% and 41.6% had trauma level 1 and level 3 trauma respectively. In our study 18.3% of patients required surgical treatment and 81.7% were managed conservatively. Similar results were reported by Ndung'u et al., (2019) who also asserted that most of the patients (71.5%) required conservative and 28.5% were treated with surgical treatment. [16]
However, a study by Onyemaechi and partners (2020) highlighted that 55.9% patients required surgery while 44.1% of patients were treated non operatively.[7] Majority of our patients had a hospital stay of 1-5 days and the with a mean hospital stay was of 2.91+9.729 days. Sadoway and partners (2024) reported a higher mean hospital stay of 7.6 ± 9.1 days.[9]
When 30-days mortality rate was assessed among patients, study demonstrated that the mortality rate was only 0.6% (3 patients). The findings of our study are much better than the study carried out by Schuster et al. (2024) who elucidated that 30-day mortality rate was 19.0%.[17] However, a study conducted by Thakur et al., (2022) reported that mortality rate was 4.3% (39 patients).[18]
This Study also assessed the correlation between injury pattern and child’s age, significant results (P=0.000) were found regarding age with mechanism of injury and region involved. A study performed by Fylli et al. (2023) also showed significant association (P<0.001) of age with mechanism of injury and region involved.[15] Bao and coworkers (2024) also confirmed significant association (P<0.001) of age with mechanism of injury and region involved.[4]
Conclusion
Majority of injuries patterns in our patients occurred due to falls among male pediatric patients whom mainly at age 4 to 8 years. There was significant correlation of age with the mechanism of injury and region involved. Further studies are required to assess a more details about injury patterns of pediatric trauma.
References
1. Madar RT, Goldberg A, Newman N, Waisman Y, Greenberg D, Adini B. A management model for admission and treatment of pediatric trauma cases. Israel J Health Pol Res. 2021; 10: 73. https://doi.org/10.1186/s13584-021-00506-5
2. Alansari AN, Mekkodathil A, Peralta R, Baykuziyev T, Alhussaini NWZ, Asim M, et al. Patterns, mechanism of injury and outcome of pediatric trauma at a level 1 trauma centre: a descriptive retrospective analysis. Front Pediatr. 2023; 11: 1084715. https://doi.org/10.3389/fped.2023.1084715
3. Yaseen TM, Hussain S, Fazal A, Zulfiqar A. Pediatric injury patterns presenting at a tertiary care hospital emergency department. Pak J Med Health Sci. 2023; 17(1): 463-5. https://doi.org/10.53350/pjmhs2023171463
4. Bao Y, Ye J, Hu L, Guan L, Gao C, Tan L. Epidemiological analysis of a 10 year retrospective study of pediatric trauma in intensive care. Scientific Rep. 2024; 14: 21058. https://doi.org/10.1038/s41598-024-72161-0
5. Amato S, Culbreath K, Dunne E, Sarathy A, Siroonian O, Sartorelli K, et al. Pediatric trauma mortality in India and the United States: a comparison and risk-adjusted analysis. J Ped Surg. 2023; 58: 99-105. https://doi.org/10.1016/j.jpedsurg.2022.09.036
6. McAleese T, Brent L, O’Toole P, Synnott K, Quinn N, Deasy C, et al. Paediatric major trauma in the setting of the Irish trauma network. Injury. 2021; 52: 2233-43. https://doi.org/10.1016/j.injury.2021.05.032
7. Onyemaechi NO, Bisi-Onyemaechi AI, Nduagubam OC. Epidemiology and pattern of paediatric injuries in a developing country: an analysis of 170 injuries. Malawi Med J. 2020; 32(2): 95-100. https://doi.org/10.4314/mmj.v32i2
8. Cintean R, Eickhoff A, Zieger J, Gebhard F, Schütze K. Epidemiology, patterns, and mechanisms of pediatric trauma: a review of 12,508 patients. Eur J Trauma Emerg Surg. 2023; 49: 451-9 https://doi.org/10.1007/s00068-022-02088-6
9. Sadoway A, Kinden R, Erdogan M, Kureshi N, Johnson M, Green RS, et al. Epidemiology and factors associated with mortality among pediatric major trauma patients in Nova Scotia: A 17-year retrospective analysis. Injury. 2024; 55: 111484. https://doi.org/10.1016/j.injury.2024.111484
10. Almalki MM, Almalki ME, Alsulaimani N, Tariq S, Alqahtani T, Baalaraj F, et al. Epidemiology of pediatric trauma in Makkah, Kingdom of Saudi Arabia. An observational cohort study. Saudi Med J. 2023; 44(1): 808-14. https://doi.org/10.15537/smj.2023.44.8. 20230292
11. Su ZY, Zhu YF, Wang XY, Wang WT, Wu K, Wang LY, et al. Child and adolescent trauma epidemiology: in sights from a comprehensive retrospective review of 4568 pediatric trauma cases. J Biosci Med. 2024; 12: 550-9. https://doi.org/10.4236/jbm.2024.1212041
12. Jones S, Tyson S, Young M, Gittins M, Davis N. Patterns of moderate and severe injury in children after the introduction of major trauma networks. Arch Dis Child. 2019; 104: 366-71. http://dx.doi.org/10.1136/archdischild-2018-315636
13. Kunwar A, Manjhi B, Saurabh A, Shekhar S. Epidemiology and pattern of paediatric trauma in one of the biggest trauma centres of India. Int J Res Orthop. 2020; 6: 1077-81. http://dx.doi.org/10.18203/issn.2455-4510.IntJResOrthop20203061
14. Dagnaw Y, Fenta B, Yetwale A, Biyazin T, Sayih A, Dessalegn N, et al. Mechanisms, pattern and outcome of pediatrics trauma at Agaro General Hospital, Southwest Ethiopia, 2021. Health Serv Res Manag Epidemiol. 2022; 9: 1-8. https://doi.org/10.1177/23333928221101975
15. Fylli C, Schipper IB, Krijnen P. Pediatric trauma in the Netherlands: incidence, mechanism of injury and in-hospital mortality. World J Surg. 2023; 47: 1116-28. https://doi.org/10.1007/s00268-022-06852-y
16. Ndung'u A, Sun J, Musau J, Ndirangu E. Patterns and outcomes of paediatric trauma at a tertiary teaching hospital in Kenya. Afr J Emerg Med. 2019; 9: S47-51. https://doi.org/10.1016/j.afjem.2018.12.004
17. Schuster A, Klute L, Kerschbaum M, Kunkel J, Schaible J, Straub J, et al. Injury pattern and current early clinical care of pediatric polytrauma comparing different age groups in a level I trauma center. J Clin Med. 2024; 13: 639. https://doi.org/10.3390/jcm13020639
18. Thakur N, Jaiswal V, Singh A, Kumar N, Misra M, Tiwari S, et al. Epidemiology and pattern of injury of pediatric trauma patients in level l trauma centre of Northern India. Trauma. 2022; 26(1): 15-9. https://doi.org/10.1177/14604086221111202.
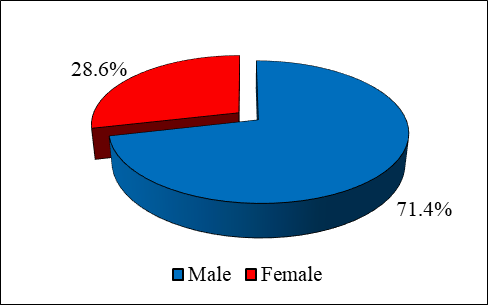
Figure 1
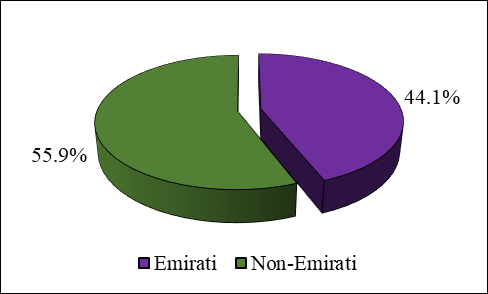
Figure 2
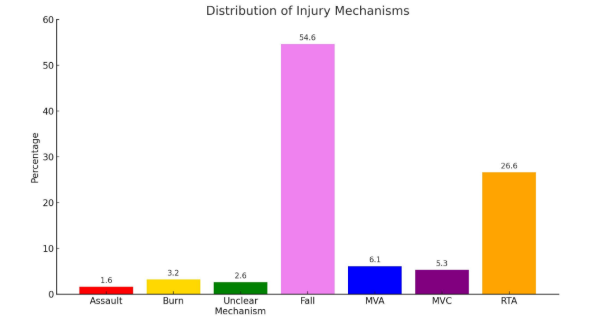
Figure 3