Primary Gastrointestinal Non-Hodgkin’s Lymphoma Presenting as Pyrexia of Unknown Origin: A Rare Case Report
Primary Gastrointestinal Non-Hodgkin’s Lymphoma Presenting as Pyrexia of Unknown Origin: A Rare Case Report
Dr. Murtaza Makasarwala *
*Correspondence to: Dr. Murtaza Makasarwala, Consultant Robotic Advanced Laparoscopic GI and Laser surgeon, Shalby Hospital, Adajan, near navyug college, Surat-395009, India.
Copyright
© 2025 Dr. Murtaza Makasarwala. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 13 May 2025
Published: 19 May 2025
DOI:https://doi.org/10.5281/zenodo.15686626
Abstract
Background: Primary gastrointestinal non-Hodgkin’s lymphoma (PGINHL) is a rare form of lymphoma that primarily involves the gastrointestinal (GI) tract without systemic lymphadenopathy or bone marrow involvement. It can rarely present as pyrexia of unknown origin (PUO), posing a diagnostic challenge.
Case Presentation: We report a 48-year-old male who presented with PUO and vague lower abdominal discomfort. Imaging revealed aneurysmal dilatation of the distal ileum with perilesional lymphadenopathy. Fine Needle Aspiration Cytology (FNAC) confirmed the diagnosis of lymphoma. The patient underwent surgical resection of the involved bowel segment followed by adjuvant immunochemotherapy using the R-CHOP regimen.
Conclusion: PGINHL should be considered in the differential diagnosis of PUO, particularly in the absence of infectious foci. Surgical resection followed by immunochemotherapy remains the cornerstone of treatment for small bowel PGINHL.
Keywords: Pyrexia of Unknown Origin, Primary Gastrointestinal Lymphoma, DLBCL, Small Bowel Lymphoma, R-CHOP.
Primary Gastrointestinal Non-Hodgkin’s Lymphoma Presenting as Pyrexia of Unknown Origin: A Rare Case Report
Introduction
Pyrexia of unknown origin (PUO) is a perplexing clinical scenario that continues to challenge physicians despite advances in diagnostic technologies. Initially defined by Petersdorf and Beeson in 1961, PUO refers to a condition in which a patient presents with a fever exceeding 38.3°C on multiple occasions for more than three weeks, with no established diagnosis after one week of hospital-based investigations. Although the original definition has since evolved, PUO remains a diagnostic enigma and often acts as a harbinger of rare or atypical disease processes. The etiological spectrum of PUO includes infections, malignancies, non-infectious inflammatory diseases, and miscellaneous or undiagnosed conditions. Among these, malignancies account for a significant proportion of cases, with lymphomas being one of the most commonly implicated neoplastic causes.
Non-Hodgkin’s lymphoma (NHL) is a heterogeneous group of lymphoid malignancies that can arise in both nodal and extranodal tissues. Primary gastrointestinal non-Hodgkin’s lymphoma (PGINHL) is a rare extranodal manifestation of NHL, defined by lymphoma originating in the gastrointestinal (GI) tract without evidence of systemic or widespread nodal disease at the time of diagnosis. It accounts for approximately 10–15% of all NHLs and 30–40% of extranodal lymphomas. Among the segments of the GI tract, the stomach is the most frequently involved site, followed by the small intestine, particularly the ileum due to its abundant lymphoid tissue in Peyer’s patches.
Despite being the second most common extranodal site, small bowel lymphomas are often misdiagnosed or diagnosed late, largely due to their non-specific and insidious presentation. While some patients may present with overt gastrointestinal symptoms such as abdominal pain, weight loss, or GI bleeding, others—like in the case we present—may manifest with vague symptoms or isolated systemic features like fever. This atypical presentation makes the diagnostic process particularly challenging, often delaying appropriate intervention.
In developing countries like India, where infectious etiologies such as tuberculosis dominate the differential diagnosis of PUO, the possibility of an underlying malignancy is often considered late. However, early consideration of neoplastic causes, especially when infectious and autoimmune causes have been excluded, can significantly improve patient outcomes by enabling timely diagnosis and treatment.
This article presents a rare case of PGINHL of the small bowel in a 48-year-old male who initially presented with PUO. The absence of classic gastrointestinal symptoms, combined with the subtlety of physical and laboratory findings, posed a diagnostic challenge. Through detailed radiological evaluation, targeted biopsy, and histopathological analysis, the diagnosis of diffuse large B-cell lymphoma (DLBCL) of the ileum was established. The patient was successfully treated with surgical resection followed by standard immunochemotherapy. This case highlights the importance of maintaining a broad differential when evaluating PUO and underlines the critical role of multimodal diagnostics and treatment in managing rare presentations of gastrointestinal lymphomas.
Case Presentation
A 48-year-old man presented with high-grade, intermittent fever for two weeks, accompanied by chills, generalised weakness, and vague lower abdominal pain. Additional complaints included recent onset of cough and dysuria. The patient had a history of COVID-19 infection and acute limb ischemia five months prior and was on antiplatelet and anticoagulant therapy.
On examination, he was pale, with mild right iliac fossa tenderness. No peripheral lymphadenopathy or organomegaly was noted. Laboratory findings revealed:
- Hemoglobin: 7.4 g/dL
- WBC: 8,900/mm³
- Platelets: 3.18 × 10?/mm³
- Elevated ESR: 80 mm/hr
- CRP: 260.6 mg/L
- Procalcitonin: Normal (0.28 ng/ml)
Septic screens and chest X-ray were unremarkable. Abdominal ultrasonography revealed a heterogeneous pelvic mass with air pockets. Contrast-enhanced CT (CECT) of the abdomen showed aneurysmal dilatation of the distal ileum with perilesional bulky lymphadenopathy.
Colonoscopy was inconclusive due to the inaccessibility of the distal ileal lesion. Ultrasound-guided FNAC revealed atypical lymphoid cells suggestive of lymphoma.
Management and Outcome
The patient received empirical antibiotics and antipyretics initially. After exclusion of infectious causes, antibiotics were discontinued. He underwent exploratory laparotomy which revealed a 6 × 5 cm distal ileal mass located 30 cm from the ileocecal junction with associated mesenteric lymphadenopathy. An en-bloc resection of the involved ileal segment with ileoascending anastomosis was performed.
Histopathological examination revealed sheets of large atypical lymphoid cells with vesicular nuclei and prominent nucleoli, consistent with diffuse large B-cell lymphoma (DLBCL). Immunohistochemistry showed:
- CD20 positivity
- High Ki67 proliferation index (95%)
- Dim MUM1 reactivity
These findings confirmed a diagnosis of DLBCL, non-germinal center type.
Bone marrow examination was normal, fulfilling Dawson’s criteria for PGINHL. The patient was started on R-CHOP chemotherapy and reported significant improvement during follow-up, with weight gain and complete resolution of symptoms.
Investigations:
The patient had a normal blood count, with a high hemoglobin level, white cell count, and platelets. His renal and liver function tests were normal, but his inflammatory markers were elevated. His septic workup was negative, and his procalcitonin was normal. An ultrasound abdomen revealed a well-defined mass with air pockets and enlarged lymph nodes, suggesting an abscess. A contrast enhanced CT scan further characterized the lesion, showing a long concentric bowel wall thickening of the distal ileum and surrounding bulky lymphadenopathy.
Figs. 1a and b. CECT abdomen axial and coronal images respectively showing aneurysmal dilatation of distal ileum marked with arrow.
Diagnosis and Treatment
A patient was diagnosed with abdominal tuberculosis, small bowel lymphoma, and a rare small bowel adenocarcinoma. The patient's colonoscopy revealed normal terminal ileum and a distal ileal lesion, but ultrasound guided trans-abdominal fine needle aspiration cytology (FNAC) showed atypical lymphoid cells with high nuclear atypia, suggesting lymphoma. Treatment included antipyretics, empirical antibiotics, and iron therapy. After excluding infective aetiologies, intravenous antibiotics were stopped and only antipyretics were continued. Due to high suspicion of small bowel lymphoma, the patient underwent Exploratory Laparotomy. Intraoperatively, a large distal ileal tumor was found, and enbloc resection with ileoascending anastomosis was performed.
Fig. 2. Post-surgery specimen showing large distal ileal tumour of size 6 × 5 cm (white arrow) about 30 cm from IC junction with large mesenteric lymph node deposits (red arrow).
The post-surgery histopathology report indicated non-Hodgkin's lymphoma, while microscopic examination showed large atypical lymphoid cells, typical of diffuse large B cell lymphoma (DLBCL). Immunohistochemistry confirmed the lymphoma's type and grade, with diffuse reactivity for CD20 and a high Ki67 proliferation index, suggesting non-germinal center type of DLBCL. The lymphoma's non-germinal center type was further confirmed through IHC.
Fig. 3. High power histopatological images showing monotonous infiltrate of large atypical lymphoid cells with scant cytoplasm and vesicular nuclei suggestive DLBCL.
Fig. 4a. IHC images showing diffuse reactivity for CD20 with (b) high Ki67 proliferation index of 95%. (c) Also dim nuclear reactivity for transcription factor MUM1, suggestive of DLBCL non-germinal centre type.
After surgery, the patient is afebrile and doing well, gaining weight without abdominal pain or constipation. A bone marrow examination confirmed normal PGINHL, and he started the first cycle of adjuvant immunochemotherapy R-CHOP regimen.
Discussion
Pyrexia of Unknown Origin (PUO) remains a complex clinical syndrome with a wide range of potential etiologies. Despite advances in diagnostic modalities, cases involving neoplastic causes such as lymphomas can remain elusive until advanced imaging and histopathological evaluation are performed. This case of Primary Gastrointestinal Non-Hodgkin’s Lymphoma (PGINHL) highlights the necessity of maintaining a high index of suspicion for malignancies when evaluating persistent, unexplained fevers.
Lymphomas are the second most common neoplastic cause of PUO, with diffuse large B-cell lymphoma (DLBCL) being the most common histological subtype. Gastrointestinal involvement by lymphoma may often remain clinically silent or present with vague, non-specific symptoms such as abdominal discomfort, weight loss, or anorexia, which can easily be mistaken for infectious or inflammatory gastrointestinal diseases. PUO may be the only early sign, as was the case with our patient.
PGINHL of the small bowel is particularly rare, comprising only a small subset of all gastrointestinal lymphomas. The distal ileum is more frequently involved, likely due to its abundant lymphoid tissue (Peyer’s patches). Diagnosis is often delayed due to the inaccessibility of the small intestine with routine endoscopic methods and the absence of overt mass effects or gastrointestinal bleeding in early stages.
Dawson's criteria, originally proposed in 1961, are still relevant for distinguishing PGINHL from secondary involvement of the GI tract in systemic lymphoma. Our patient met all these criteria, including the absence of peripheral and mediastinal lymphadenopathy, normal bone marrow and peripheral smear, and isolated involvement of the distal ileum with contiguous mesenteric nodes.
Surgical exploration remains both a diagnostic and therapeutic modality in many cases. Although endoscopic biopsy may be effective in gastric or colonic lymphomas, small bowel lesions are frequently discovered incidentally or during surgery for complications such as obstruction, perforation, or severe hemorrhage. In our case, surgery allowed complete excision of the mass, alleviation of symptoms, and provided adequate tissue for diagnosis and typing.
Histopathology combined with immunohistochemistry (IHC) confirmed a high-grade DLBCL, non-germinal center type, characterized by CD20 positivity and a high Ki-67 proliferation index, indicating aggressive biological behavior. This subtype is known for a less favorable prognosis compared to germinal center types but responds well to R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone), the current standard of care for DLBCL.
Several studies support the superiority of multimodality treatment over either surgery or chemotherapy alone. Surgical resection not only relieves symptoms but also reduces tumor bulk, potentially improving chemotherapy effectiveness and reducing risks such as perforation during cytoreduction. Adjuvant chemotherapy helps control microscopic disease and reduce recurrence rates. The role of radiotherapy remains controversial and is generally reserved for localized, inoperable lesions or residual disease.
Postoperative follow-up of our patient showed complete resolution of systemic symptoms, improved nutritional status, and good tolerance to the first cycle of R-CHOP, which is encouraging and consistent with outcomes reported in the literature.
Conclusion
Primary gastrointestinal non-Hodgkin’s lymphoma, though rare, should be considered in the differential diagnosis of pyrexia of unknown origin, especially when common infectious and inflammatory causes have been excluded. Clinicians must be vigilant and adopt a systematic, multidisciplinary approach that includes advanced imaging, histological confirmation, and when necessary, surgical exploration.
This case reinforces several critical clinical lessons:
• PUO can be the initial and sole presentation of serious underlying malignancy.
• Thorough evaluation including imaging and biopsy is essential when routine investigations yield no diagnosis.
• PGINHL, especially in the small bowel, often necessitates surgical management due to diagnostic limitations and risk of complications.
• Multimodal therapy, including surgical resection followed by R-CHOP chemotherapy, remains the mainstay of treatment and offers excellent prognosis when instituted early.
Early recognition and timely intervention are vital to improve outcomes and reduce morbidity in such complex cases.
References
[1] Cardona DM, Layne A, Lagoo AS. Lymphomas of the gastro-intestinal tract - Pathophysiology, pathology, and differential diagnosis. Indian J Pathol Microbiol. 2012;55(1):1.
[2] Unger M, Karanikas G, Kerschbaumer A et al. Fever of unknown origin (FUO) revised. Wien Klin Wochenschr. 2016;128:796–801.
[3] Pannu AK, Golla R, Kumari S et al. Aetiology of pyrexia of unknown origin in north India: Trop Doct. 2020;51(1):34–40.
[4] Ghimire P, Wu G-Y, Zhu L. Primary gastrointestinal lymphoma. World J Gastroenterol. 2011;17(6):697–707.
[5] Lightner AL, Shannon E, Gibbons MM et al. Primary gastrointestinal non-Hodgkin’s lymphoma of the small and large intestines: a systematic review. J Gastrointest Surg. 2015;20(4):827–39.
[6] Tatar C, Yavas M, Akkus O et al. Intestinal perforation that developed after chemotherapy in a patient diagnosed with non-Hodgkin lymphoma: A case report and review of literature. Int J Surg Case Rep. 2017;39:321–3..
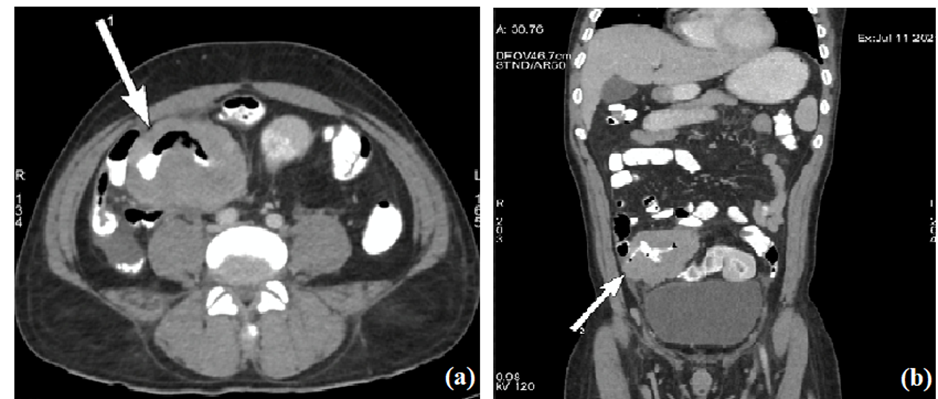
Figure 1

Figure 2
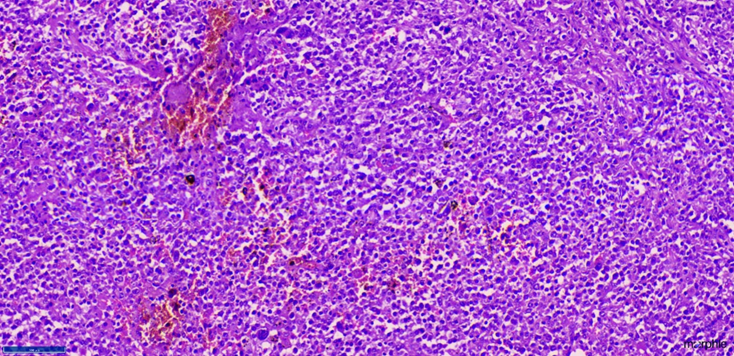
Figure 3
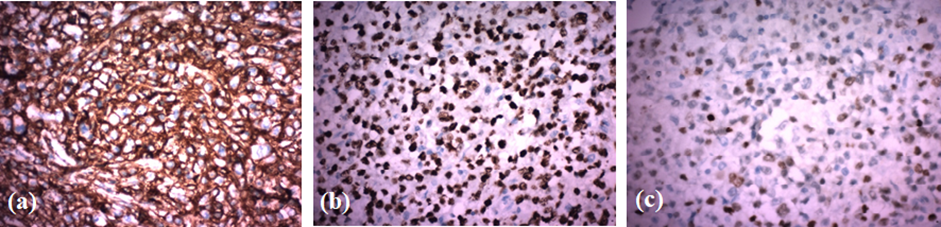
Figure 4