Comparative Study of the Feto-Maternal Outcomes in term Pregnancy with Meconium-Stained Amniotic Fluid and with Clear Amniotic Fluid.
Comparative Study of the Feto-Maternal Outcomes in term Pregnancy with Meconium-Stained Amniotic Fluid and with Clear Amniotic Fluid.
Dr. Yesha Jayesh Thakker1, Dr. Manvi Verma2*, Dr. Sunil Sharma3, Dr. Shriya Ladiwala4
1. Senior Resident, Department of Obstetrics & Gynaecology, MGM Institute of Health Sciences, Kamothe, Navi Mumbai.
2. Assistant Professor, Department of Obstetrics & Gynaecology, MGM Institute of Health Sciences, Kamothe, Navi Mumbai
3. Professor & Head of Department, Department of Obstetrics & Gynaecology, MGM Institute of Health Sciences, Kamothe, Navi Mumbai
4. Junior Resident, Department of Obstetrics & Gynaecology, MGM Institute of Health Sciences, Kamothe, Navi Mumbai.
*Correspondence to: Dr Manvi Verma, Assistant Professor, Department of Obstetrics and Gynecology, MGM Institute of Health Sciences, Kamothe, Navi Mumbai.
Copyright
© 2025 Dr. Yesha Jayesh Thakker. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 May 2025
Published: 19 May 2025
Abstract:
Background: Meconium stained amniotic fluid is associated with adverse neonatal outcomes. Proper diagnosis and management is crucial.
Aim: To compare the neonatal and maternal outcomes in term pregnancies associated with meconium-stained amniotic fluid versus with clear amniotic fluid.
Methods: The study was carried out in the Department of Obstetrics and Gynaecology, MGM Women’s and Children Hospital, Kalamboli, Navi Mumbai over a period of one and half years. The feto-maternal outcomes was compared between 55 cases of meconium-stained amniotic fluid and 55 cases of clear amniotic fluid
Results: The study observed a total of 4569 deliveries in our institution during the study period. The number of cases with meconium staining of amniotic fluid was 125, giving the incidence rate of MSL as 2.74%. For analysis purpose, we included 55 cases of meconium staining of liquor and 55 cases with clear amniotic fluid. MSL was associated with unfavourable maternal and neonatal outcomes and was observed to be positively correlated with increasing maternal age and period of gestation. More number of babies had fetal distress in MSL group, thereby requiring resuscitation and NICU admissions. MSL was also associated with development of Meconium aspiration syndrome and neonatal mortality. As MSL was associated with increased incidence of fetal distress, we also observed higher caesarean section rate in this group.
Conclusion: Meconium-stained liquor should not be taken lightly nor is there a need for alarm. The diagnosis of Meconium-stained liquor should alert the obstetrician to potential fetal distress and encourage increased vigilance in managing such cases by close feto-maternal monitoring.
Keywords: Meconium stained liqour, MSAF, meconium stained amniotic fluid, NICU
Comparative Study of the Feto-Maternal Outcomes in term Pregnancy with Meconium-Stained Amniotic Fluid and with Clear Amniotic Fluid.
Introduction
Meconium, the first intestinal contents of a developing fetus and the newborn's initial bowel movement, can appear green, brown, or yellow. [1] The correlation between MSAF with fetal outcomes and associated risk factors has been thoroughly researched. Meconium-stained amniotic fluid (MSAF) is linked to higher rates of operative births, adverse neonatal outcomes, and increased NICU admissions. However, careful labor management, including continuous fetal heart rate monitoring, can help minimize unnecessary cesarean sections in pregnancies with MSAF. [2] While fetal stress near delivery can sometimes trigger meconium expulsion, full-term newborns typically pass their first meconium within the first day after birth. [3]
The observation of meconium-stained amniotic fluid during delivery necessitates immediate involvement of a neonatal resuscitation team. [4] The presence of meconium-stained amniotic fluid has been found to be a significant predictor of adverse maternal and perinatal outcomes. A substantially higher risk of perinatal asphyxia, nonreassuring fetal heart rate patterns, neonatal sepsis, meconium aspiration syndrome, NICU admission, early neonatal death, operative delivery, and puerperal sepsis in meconium-exposed cases has been found emphasizing the critical need for focused intrapartum and postnatal care for these mothers. [2, 5,6]
Fetal distress, gestational age, delivery by lower uterine segment cesarean section (LUCS), and prolonged labor significantly increase the risk of meconium staining at birth. Recognizing these factors can facilitate early identification of complications and improved management of meconium-stained neonates. [7]
The aim of the study was to compare the neonatal and maternal outcomes in term pregnancies associated with meconium-stained amniotic fluid versus with clear amniotic fluid. The objectives of the study included determination of incidence of meconium-stained amniotic fluid (MSAF) in a low-risk population at term gestation, to determine the incidence of clear stained amniotic fluid in a low-risk population at term gestation and to compare the feto-maternal outcomes in MSAF and clear amniotic fluid.
Materials and Methods
The study was a prospective, observational comparative study conducted in the Department of Obstetrics and Gynaecology, MGM Women’s and Children Hospital, Kalamboli, Navi Mumbai. The study protocol was approved by the Institutional Ethics Committee and informed Consent was taken from all participants.
The sample size was determined as per following calculation:
Cases with regular visits Prevalence (P) = 16%
Q = 100% - P =84%
Random Normal Variate Z = 1.96 for 95% Of Confidence Interval (CI).
Margin of Error = 07%
Sample Size Formula:
n = (z2 pq)/ L2
n = ((1.96)2.16. 84)/ 72
The total sample size (n) came out to be 110, out of which 55 cases of meconium-stained amniotic fluid and 55 cases of clear amniotic fluid were recruited.
Inclusion criteria: All patients with cephalic presentation and meconium stained amniotic fluid after spontaneous or artificial rupture of membrane irrespective of age, parity and stage of labor and patients willing to give written informed consent were included in Study Group A. Patients with clear liquor after spontaneous or artificial rupture of membrane were included in control group B.
Exclusion Criteria Patients with abnormal presentation, multiple gestation, fetal malformation, intrauterine fetal demise, eclampsia, antepartum hemorrhage, gestational age less than 37 weeks and patients who refused to give consent.
Study duration: One and a half years (August 2022 to December 2023)
Written informed consent was taken from all patients. After recruitment, the patients' age, complete medical and surgical history, past obstetrical history, menstrual history, history of current pregnancy, age, gravidity, and parity were noted and recorded in a pre-formed proforma. General examination was done including pulse, blood pressure, oedema, pallor, jaundice, dehydration and temperature. Systemic examination of cardiovascular and respiratory system was done and abnormal findings, if any were noted. Obstetric examination was done noting the height of fundus, amount of amniotic fluid, presentation, position, uterine contraction, fetal heart rate, pelvic status. Uses of any medication like oxytocin, sedatives, analgesics or any transfusions was also noted. When MSAF appeared along with rupture of membranes, it was collected for clinical gradation before vaginal examination. MSAF was collected by introducing Sim’s speculum under aseptic precautions and material was taken into a clear test tube for clinical classification and gradation based on consistency and color. Then, a thorough vaginal examination was performed to evaluate the condition of cervix and station of fetal head, to exclude cord prolapse and note the colour and consistency of amniotic fluid. Amniotc fluid was categorized as thin meconium stained when it had a greenish yellow color and thick meconium stained when it had a thick consistency with dark green, tarry black, or muddy color. Cases where there had been a rupture of membrane with clear amniotic fluid were taken as controls.
Immediately after birth, the baby’s mouth, nostrils were cleaned by suction catheter. APGAR score of newborn was assessed at one minute and five minutes. When the baby's Apgar score was seven or higher, it was considered to be in good condition without being asphyxiated. When the score fell below 4, it was deemed severely asphyxiated; in between (score 4 to 6) it was termed moderately asphyxiated. Resuscitation was taken into consideration based on the need as assessed by the APGAR score while consulting a pediatrician. Normal babies who did not experience any postnatal difficulties were handed over to their mother. Babies were kept in the NICU if they showed any sign of asphyxia within 24 hours. If a baby who was initially handed over to the mother experienced any complications, it was also taken to the NICU. The reason for mortality and the duration of the neonate and patient's hospital stay were also noted.
The maternal outcome parameters which were recorded were general examination (temperature, pulse, blood pressure, respiratory rate, pallor and edema) and systemic examination (cardiovascular and respiratory system), duration of labour, mode of delivery (Caesarean section/ vaginal delivery), development of chorioamnionitis, sepsis or other complications. The fetal parameters which were recorded were Apgar score at 1 minute and at 5 minutes, resuscitation measures required if any, NICU admission, development of complications like meconium aspiration syndrome, aspiration pneumonia, early neonatal death (within 7 days of birth), septicemia, intrauterine fetal death, fetal distress during labor and hypoxic ischemic encephalopathy.
Statistical Analysis
Mean ± SD was used to represent quantitative data. Percentage was used to express both nominal and categorical data. Quantitative data was evaluated using the t-test; non-parametric data was studied using the Mann Whitney test, and categorical data was analyzed using the chi-square test. Quantitative variable correlation was calculated using the Pearson correlation coefficient. The p-value's significance criterion was set at less than 0.05. Using SPSS software version 26, all analyses were performed.
Results
A total of 4569 deliveries were observed during the study period. The study was a case control study including 55 cases of meconium staining of liquor and 55 cases with clear amniotic fluid. The number of cases with meconium staining of amniotic fluid was 125; giving the incidence rate of MSL as 2.74%. Overall, 58.2% babies were males and 41.8% were females, with no difference between study groups (p-0.07). Incidence of low birth weight among case group was 52.7% as compared to 40% amongst controls, the difference was statistically non-significant (p-0.251).
Analysing the demographic variables, it was found that cases with MSL were significantly younger as compared to cases with clear amniotic fluid (23.04 vs 25.12 years; p - 0.04). (Figure 1) Gestation period in cases with MSL was significantly more as compared to cases with clear amniotic fluid (38.93 vs 37.68 weeks; p - 0.04). (Figure 1)
Fig 1- Comparison between Age, gestational age and cesarean section rate
Requirement of LSCS was observed to be significantly higher in MSL cases (67.3% vs 23.6%; p<0.01). (Figure1 ) Amongst the 37 cases requiring LSCS in MSL group, 33 were cases of fetal distress, 2 had cord prolapse and 2 had non-progression of labor. Amongst 13 cases of LSCS in clear amniotic fluid group, 11 had fetal distress, one had non-progression of labour and one had premature rupture of membranes.
As regards maternal complications, incidence of chorio-amnionitis was 9.1% among mothers with MSL as compared to none in control group while incidence of sepsis was 5.5% and 0% respectively (p-0.028, 0.24). (Table I)
Table I: Maternal complications
|
Maternal Complications |
MSL |
Total |
p-value |
|
|
No |
Yes |
|||
|
Chorio-amnionitis |
0 |
5 |
5 |
0.028 |
|
0.0% |
9.1% |
4.5% |
||
|
Sepsis |
0 |
3 |
3 |
0.24 |
|
0.0% |
5.5% |
2.7% |
||
Regarding, fetal complications, mean APGAR of 7 or below at 5 minutes was seen in 16.4% cases and 9.1% controls (p-0.79). (Table II) Requirement of resuscitation in newborns was seen in 16.4% cases as compared to 7.3% controls, the difference was statistically non-significant (p-0.237). (Table III)
Table II: Distribution of cases as per APGAR score
|
APGAR <= 7 at 5 mins |
MSL |
Total |
|
|
No |
Yes |
||
|
Yes |
5 |
9 |
14 |
|
9.1% |
16.4% |
12.7% |
|
|
No |
50 |
46 |
96 |
|
90.9% |
83.6% |
87.3% |
|
|
Total |
55 |
55 |
110 |
|
100.0% |
100.0% |
100.0% |
|
|
p- value - 0.79 |
|||
Table III: Distribution of cases as per requirement of resuscitation
|
Requirement of Resuscitation |
MSL |
Total |
|
|
No |
Yes |
||
|
No |
51 |
46 |
97 |
|
92.7% |
83.6% |
88.2% |
|
|
Yes |
4 |
9 |
13 |
|
7.3% |
16.4% |
11.8% |
|
|
Total |
55 |
55 |
110 |
|
100.0% |
100.0% |
100.0% |
|
|
p- value 0.237 |
|||
Table IV: Distribution of cases as per neonatal complications
|
Neonatal Complications |
MSL |
Total |
p-value |
|
|
No |
Yes |
|||
|
Fetal Distress |
2 |
9 |
11 |
0.01 |
|
3.6% |
16.4% |
10.0% |
||
|
Aspiration Pneumonia |
0 |
2 |
2 |
0.49 |
|
0.0% |
3.6% |
1.8% |
||
|
MAS |
0 |
5 |
5 |
0.02 |
|
0.0% |
9.1% |
4.5% |
||
|
Sepsis |
0 |
3 |
3 |
0.24 |
|
0.0% |
5.5% |
2.7% |
||
|
HIE |
0 |
0 |
0 |
NA |
|
0.0% |
0.0% |
0.0% |
||
|
IUFD |
0 |
1 |
1 |
1.0 |
|
0.0% |
1.8% |
0.9% |
||
|
Early Neonatal Death |
0 |
3 |
3 |
0.24 |
|
0.0% |
5.5% |
2.7% |
||
Table V: Distribution of cases as per requirement of NICU stay
|
NICU Stay |
MSL |
Total |
|
|
No |
Yes |
||
|
No |
47 |
33 |
80 |
|
85.5% |
60.0% |
72.7% |
|
|
Yes |
8 |
22 |
30 |
|
14.5% |
40.0% |
27.3% |
|
|
Total |
55 |
55 |
110 |
|
100.0% |
100.0% |
100.0% |
|
|
p- value <0.01 |
|||
Discussion
The passing of meconium in pregnancy can be seen as either as a warning sign of fetal impairment or as a normal part of the gastrointestinal system maturing in response to an acute or chronic hypoxic event. The aim of the study was to ascertain the incidence and frequency of MSAF in a low-risk population at term gestation and comparing the neonatal and maternal outcomes in pregnancies with clear amniotic fluid.
Incidence of Meconium-Stained Liquour (MSL)
In present study, the incidence of meconium staining of amniotic fluid was observed as 2.74%. Various authors have found the incidence of meconium stained of amniotic fluid between the range of 10 % and 27%, and it is found to vary with gestational age and obstetric complications. [8-12] The incidence of lower MSAF in present study can be attributed to the inclusion of only low risk pregnancies.
Maternal Parameters
Demography & Gestation Period
Cases with MSL in the present study were significantly younger as compared to cases with clear amniotic fluid (23.04 vs 25.12 years; p - 0.04). However, Addisu D et al observed that mothers over the age of 30 were 5.6 times more likely to develop meconium-stained amniotic fluid during labor compared to those under 30 years [AOR = 5.6, 95% CI = 3.35–9.44]. [13] Another study however found no statistically significant difference between mean age of study and control population when histopathological changes were studied between placentas associated with meconium staining versus clear liquor. [14]
Gestation period in cases with MSL in the current study was significantly more as compared to cases with clear amniotic fluid (38.93 vs 37.68 weeks; p - 0.04).Similar to the current study, Dereje T et al found that late-term pregnancy (GA 41- 41+6 weeks) has 8.82 times higher odds of having MSAF than early-term pregnancy (GA 37 -38+6 weeks) [15] However, Lavie et al concluded that in term pregnancies affected by meconium-stained amniotic fluid (MSAF), adverse neonatal and maternal delivery outcomes occur at similar rates across all gestational ages. Consequently, any term pregnancy with MSAF should be regarded as high risk and managed accordingly. [16] Thus it can be said that the association of age and gestational age with meconium stained amniotic fluid has been found to vary.
Mode of Delivery
Requirement of LSCS in this study was observed to be significantly higher in MSL cases (67.3% vs 23.6%; p<0.01). Amongst the 37 cases requiring LSCS in MSL group, 33 were cases of fetal distress, 2 each had cord prolapse and non-progress of labor. Amongst 13 cases of LSCS in clear amniotic fluid group, 11 had fetal distress and 1 each had non-progress and PROM. Qadir S et al observed incidence of assisted vaginal delivery and cesarean section as 8.5% and 26.4% in controls and 18.8% and 56.2% in MSL group ;fetal distress was more common in MSAF group, leading to higher caesarean section rate in this group. [17] In a study by Rana BB et al, the caesarean section rate in thick meconium cases was 89.28% versus 50 % in moderate MSL cases. However, it was also mentioned that MSAF is not an indication of caesarean section. [18] Thus similar to the finding observed in the present study, majority of studies have found a higher caesarean section rate in meconium stained amniotic fluid group.
Maternal Complications
Incidence of chorio-amnionitis was 9.1% among mothers with MSL as compared to none in control group while incidence of sepsis was 5.5% and 0% in the present study (p-0.028, 0.24). Intraamniotic infection/ inflammation has emerged as an important factor in meconium-stained amniotic fluid in term and preterm gestations, as there is a higher rate of clinical chorioamnionitis and sepsis with patients with these conditions. In patients with clinical chorioamnionitis, the presence of meconium-stained amniotic fluid (MSAF) has been found to be associated with a significantly elevated risk of microbial invasion of the amniotic cavity (19.6% vs. 4.7%; p < 0.05) and bacterial endotoxin (46.9% vs. 4.7%; p < 0.001). Furthermore, MSAF has been characterized by higher concentrations of interleukin (IL)-6, indicating a pronounced intra-amniotic inflammatory response. [19, 20]
Fetal Parameters
Birth Weight
Incidence of low birth weight among case group was 52.7% as compared to 40% amongst controls in the current study (p-0.251). Similar finding has been suggested by Parween et al wherein pregnancies complicated by meconium-stained amniotic fluid (MSAF) have been found to have a higher incidence of instrumental delivery, cesarean delivery, low birth weight, and fetal distress. [2]
APGAR Score
Mean APGAR of 7 or below at 5 minutes was seen in 16.4% cases and 9.1% controls in the present study. The result was however statistically non-significant (p-0.79). Contrary to this, in a study by Masood M et al, it was observed that neonates of 77.4 % women with MSAF had an Apgar score of less than six at one minute. However, neonates of only 50 % the women with clear liquor had an APGAR score less than 6 at the one-minute interval with a significant association (p=0.02) [21]
Fetal Complications
Among neonatal complications, fetal distress (16.4% vs 3.6%; p-0.01) and meconium aspiration syndrome (9.1% vs 0%; p-0.02) were observed to be significantly more among meconium stained liquour cases. Incidence of IUFD and early neonatal death was 1.8% and 5.5% among MSL cases in the current study. NICU stay was required in 40% cases of MSL as compared to 14.5% cases with clear amniotic fluid (p<0.01). The finding can be attributed to higher incidence of respiratory distress in thick meconium stained group babies.
Similarly, Qadir S et al observed that fetal distress in the MSAF group was more common in cases (29.6%) compared to control group (9.3%), also rates of NICU admission were higher in cases (24.5%) which was statistically significant (p<0.001). [17] Addisu D et al has also found that MSAF significantly increases the risk of adverse birth outcomes, including intrapartum fetal death, neonatal sepsis, meconium aspiration syndrome (MAS), and early neonatal death. [22]
Conclusion
Meconium Stained Liquor is associated with unfavourable maternal and neonatal outcomes and was observed to be positively correlated with increasing maternal age and period of gestation. The diagnosis of Meconium-stained liquor should alert the obstetrical to potential fetal distress and encourage increased vigilance in managing such cases by close monitoring.
Ethical Approval: The Study Was Conducted In Accordance With The Ethical Standards Of The Institutional And/Or National Research Committee And With The 1964 Helsinki Declaration And Its Later Amendments Or Comparable Ethical Standards. The Institutional Ethical Approval Letter For The Study Has Been Attached.
Conflict Of Interest: The Authors Declare That They Have No Conflict Of Interest
Informed Consent: Informed Consent Was Obtained From All Individual Participants Included In The Study
Funding: The Logistic Support Was Provided By MGM Hospital Kamothe, No Other Source Of Funding
References
1. Singh A, Mittal M. Neonatal microbiome - a brief review. J Matern Fetal Neonatal Med. 2020 Nov;33(22):3841-8.
2. Parween S, Prasad D, Poonam P et al. Impact of Meconium-Stained Amniotic Fluid on Neonatal Outcome in a Tertiary Hospital. Cureus. 2022 Apr 25;14(4):e24464.
3. Patton L, Neu J. Microbes and the womb: does it matter? In Claud EC, editor, The Developing Microbiome Lessons from early life. Chicago, Academic Press, Elsevier, 2020; 1-20
4. Skelly CL, Zulfiqar H, Sankararaman S. Meconium. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK542240/
5. Addisu D, Mekie M. Adverse Maternal and Perinatal Outcomes of Meconium-Stained Amniotic Fluid in Term Labor at Hospitals in South Gondar Zone, Northwest Ethiopia: A Prospective Cohort Study. Biomed Res Int. 2023 Aug 4;2023:8725161.
6. Tolu LB, Birara M, Teshome T et al. Perinatal outcome of meconium stained amniotic fluid among labouring mothers at teaching referral hospital in urban Ethiopia. PLoS One. 2020 Nov 13;15(11):e0242025.
7. Rafia R, Abid Hossain M, Manisha B et al. Risk Factors Associated with Meconium-Stained Amniotic Fluid in Neonates: A Tertiary Centre Experience from Bangladesh. Acad J Ped Neonatol. 2021; 10(2): 555840.
8. Tantu T, Zewdu D, Degemu F et al. The incidence and determinants of the meconium-aspiration syndrome among mothers with meconium-stained amniotic fluid after emergency cesarean section: A prospective cross-sectional study in a specialized hospital, south Ethiopia. Front Pediatr. 2023 Mar 23;11:1149398.
9. Fanaroff AA. Meconium aspiration syndrome: historical aspects. J Perinatol. 2008 Dec;28 Suppl 3:S3-7.
10. Gupta V, Bhatia BD, Mishra OP. Meconium stained amniotic fluid: antenatal, intrapartum and neonatal attributes. Indian Pediatr. 1996 Apr;33(4):293-7.
11. Dargaville PA, Copnell B; Australian and New Zealand Neonatal Network. The epidemiology of meconium aspiration syndrome: incidence, risk factors, therapies, and outcome. Pediatrics. 2006 May;117(5):1712-21.
12. Unnisa S, B.S. S, Rao S et al. Maternal and fetal out come in meconium stained amniotic fluid in a tertiary centre. Int J Reprod Contracept Obstet Gynecol. 2016;813–7.
13. Addisu D, Asres A, Gedefaw G et al. Prevalence of meconium stained amniotic fluid and its associated factors among women who gave birth at term in Felege Hiwot comprehensive specialized referral hospital, North West Ethiopia: a facility based cross-sectional study. BMC Pregnancy Childbirth. 2018 Oct 30;18(1):429.
14. Mondal TR, Bandyopadhyay G, Mukhopadhyay SG et al. Histopathological Changes of Placenta in Meconium Stained Liquor and Its Relevance in Fetal Distress: A Case Control Study. Turk Patoloji Derg. 2019;35(2):107-18.
15. Dereje T, Sharew T, Hunde L et al. Meconium Stained Amniotic Fluid and Associated Factors among Women Who Gave Birth at Term in Adama Hospital Medical College, Ethiopia. Ethiop J Health Sci. 2023 Mar;33(2):219-26.
16. Lavie A, Fisch S, Reicher L at al. Correlation of Meconium-Stained Amniotic Fluid and Adverse Pregnancy Outcomes between 37 to 39 and 40 to 42 Weeks of Gestational Age. Am J Perinatol. 2024 May;41(S 01):e1591-8.
17. Qadir S, Jan S, Chachoo JA et al.Perinatal and neonatal outcome in meconium stained amniotic fluid. Int J Reprod Contracept Obstet Gynecol. 2017;5(5):1400-5.
18. Rana BB, Airao BB. Fetal outcome and mode of delivery in a patient with meconium-stained amniotic fluid. Int J Reprod Contracept Obstet Gynecol, 2022; 11, 3049–52.
19. Romero R, Yoon BH, Chaemsaithong P et al. Bacteria and endotoxin in meconium-stained amniotic fluid at term: could intra-amniotic infection cause meconium passage? J Matern Fetal Neonatal Med. 2014 May;27(8):775-88.
20. Gallo DM, Romero R, Bosco M et al. Meconium-stained amniotic fluid. Am J Obstet Gynecol. 2023 May;228(5S):S1158-78.
21. Masood M, Shahid N, Bano Z et al. Association of Apgar Score With Meconium Staining of Amniotic Fluid in Labor. Cureus. 2021 Jan 16;13(1): e12744.
22. Addisu D, Mekie M. Adverse Maternal and Perinatal Outcomes of Meconium-Stained Amniotic Fluid in Term Labor at Hospitals in South Gondar Zone, Northwest Ethiopia: A Prospective Cohort Study. Biomed Res Int. 2023 Aug 4;2023: 8725161.
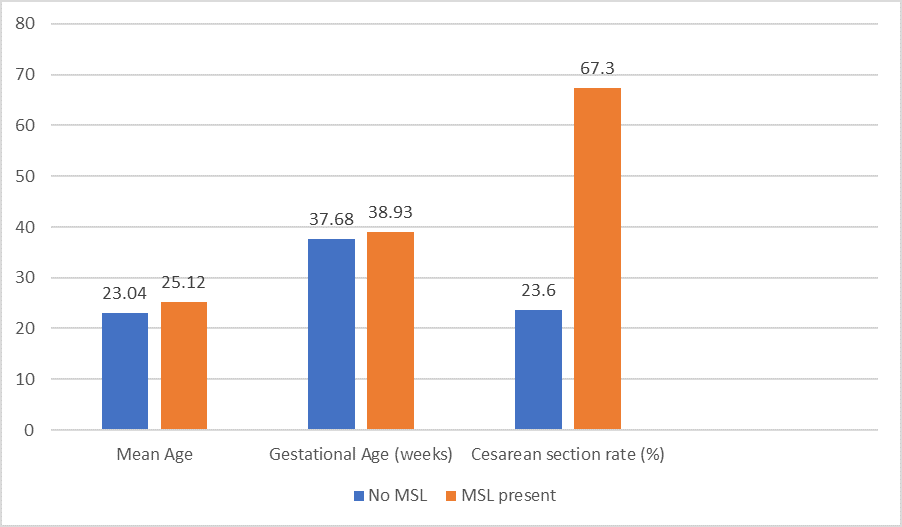
Figure 1