Ectopic Appendicitis in Amyand’s Hernia: Case Report of a Rare Clinical Challenge.
Ectopic Appendicitis in Amyand’s Hernia: Case Report of a Rare Clinical Challenge.
Capuzzo Matteo1*, Montenovo Matteo2, Ballabio Michele3, Bisagni Pietro4
1,2,3,4. Department of General Surgery, Lodi Hospital, Largo Donatori del Sangue 1 26900, Lodi, Lombardia, Italy.
*Correspondence to: Dr. Matteo Capuzzo, Department of General Surgery, Lodi Hospital, Largo Donatori del Sangue 1 26900, Lodi, Lombardia, Italy. ORCID (0000-0002-4653-6762)
Copyright
© 2025 Dr. Matteo Capuzzo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 May 2025
Published: 31 May 2025
DOI:https://doi.org/10.5281/zenodo.15686657
Abstract
Background - Inguinal hernias containing the appendix are rare, but the occurrence of acute appendicitis within the hernia sac is an even more exceptional event that entails a difficult diagnosis and a non-unique surgical treatment.
Case presentation – A male in his seventies presented to the Emergency Department with acute lower abdominal pain and a painful irreducible right inguinal swelling. CT suggested a complicated hernia, while surgery confirmed an Amyand’s hernia containing a gangrenous appendicitis with microperforation. The patient underwent appendicectomy and hernia mesh repair and was discharged after an uneventful postoperative recovery.
Conclusion - Acute appendicitis in an Amyand’s hernia is a rare condition and constitutes both a diagnostic and therapeutic challenge for acute care surgeons.
Keyword: Amyand’s hernia, Acute appendicitis, Mesh repair, Losanoff classification.
Ectopic Appendicitis in Amyand’s Hernia: Case Report of a Rare Clinical Challenge.
Introduction
Amyand’s hernia is a rare condition characterized by protrusion of vermiform appendix within an inguinal hernia sac. Its true scope remains elusive, with an incidence ranging from 0,14% to 1,3% of inguinal hernias [2-11]. Appendix within such hernias can also undergo an acute inflammatory process defining a kind of “ectopic appendicitis”. The reported incidence of this uncommon condition is 0,07-0,13% [15-19]. This clinical scenario represents not only a challenge in its diagnosis, which in most cases is intraoperative, but in its treatment too, that on the one hand requires an urgent control of the septic source and on the other hand an adequate repair of the abdominal wall.
Case Presentation
A patient in his seventh decade of life presented to the Emergency Department with acute pain in the lower abdominal quadrants, associated with painful right-sided inguinal swelling. The patient’s medical history included hypertension and chronic hepatic steatosis complicated by ascites and gastric varices.
On admission, his vital signs were stable: blood pressure was 125/85 mmHg, pulse rate was 80 bpm and body temperature was 37°C. Physical examination revealed a painful, tender and irreducible right inguinal hernia without signs of peritonitis on abdominal palpation. Laboratory tests showed an elevated C-reactive protein (CRP 112.6 mg/L) as the only abnormal finding, with white blood cell (WBC) count at 2,240/µL and neutrophil percentage at 58.1%. An abdominal CT scan revealed caecal protrusion within the inguinal hernia sac, hyperaemia of the colonic wall, free fluid in the hernia sac and ascites in the peritoneal recesses (figure 1 – 3).
Given the suspicion of a strangulated hernia, surgical intervention was indicated and the patient was taken to the operating room. Under general anesthesia, a right inguinotomy was performed as the initial approach, enabling reduction of the hernial sac’s contents into the abdomen. A subsequent laparotomy revealed an Amyand’s hernia, characterized by the protrusion of the appendix into the hernia sac. The appendix was found to be affected by acute inflammation with gangrene and a microperforation at its apex, which was buffered by the hernia sac itself, configuring a type 2 Amyand’s hernia (figure 4).
An appendectomy and adequate abdominal cavity washout were performed. A drainage tube was positioned in the pelvis, and the laparotomy was closed. Finally, the inguinal wall defect was repaired with hernioplasty using a non-absorbable prosthetic mesh via the inguinotomy approach.
The post-operative course was favourable, with progressive improvement in the patient’s clinical condition. The only reported adverse events included mild multifactorial anaemia (Hb 8.7 g/dL) without signs of bleeding, which required transfusion on post-operative day (POD) 1. This led to an immediate and stable recovery of haemoglobin levels (Hb 9.9 g/dL after transfusion of two units of red blood cells). Additionally, abundant ascitic fluid was observed from the abdominal drainage, necessitating the drainage to remain in place until POD 7.
The patient was discharged on POD 9 in good clinical condition.
Histopathological examination confirmed the diagnosis of gangrenous appendicitis, characterized by transmural necrosis, inflammatory infiltration, and loss of mucosal integrity.
Figure 1: CT Scan
Figure 2 : CT Scan
Figure 3: CT Scan
Figure 4
Discussion
Amyand's hernia is a rare condition in which the vermiform appendix protrudes within an inguinal hernia sac. It owes its name to Claudius Amyand (1660–1740), a French surgeon who, in 1735, performed the first documented successful appendectomy on an 11-year-old boy with acute appendicitis confined to an inguinal hernia sac. However, the earliest description of this condition dates to 1731 by De Garengeot [1].
Despite its historical documentation, the true prevalence of Amyand's hernia remains uncertain, with reported incidences ranging from 0.14% to 1.3% of all inguinal hernias [2–11]. This condition affects patients of all ages, with documented cases in individuals ranging from 3 weeks to 92 years old. However, it demonstrates a bimodal distribution, peaking in infants (1 month to 1 year) and the elderly (over 70 years), even if it is more commonly observed in the pediatric population due to anatomical factors. Amyand's hernia is significantly more frequent in males (over 90% of reported cases) and predominantly affects the right side. Left-sided cases are rare and often associated with anatomical anomalies such as situs inversus or intestinal malrotation [12-14].
When the appendix within the hernia sac becomes inflamed, it results in a condition sometimes referred to as “ectopic appendicitis.” The incidence of this uncommon scenario is estimated to be between 0.07% and 0.13%. The exact pathogenesis of Amyand's hernia remains poorly understood, though several theories suggest that the migration of the appendix into the inguinal canal increases its vulnerability to inflammation. Contributing factors include compromised blood supply, ischemia, bacterial overgrowth, and subsequent inflammation [15-19].
Clinically, the presence of a vermiform appendix in an inguinal hernia sac is often unrecognized, as patients typically present with the usual symptoms of an inguinal hernia. However, acute appendicitis within an Amyand's hernia can pose a diagnostic challenge. It commonly manifests as a tender, irreducible inguinal or inguinoscrotal mass that mimics a strangulated inguinal hernia. Local inflammatory signs such as erythema, edema and tenderness are often present. Systemic symptoms of acute appendicitis, including nausea and vomiting, may accompany these findings. However, classical signs such as McBurney's point tenderness and Rovsing's sign are usually absent due to the appendix's ectopic position. Additionally, fever and systemic inflammatory markers (e.g., WBC and CRP) may remain within normal ranges, complicating the differential diagnosis. Imaging modalities such as ultrasonography (US) and computed tomography (CT) scans have improved preoperative diagnosis, though their accuracy remains suboptimal, with pooled analyses indicating a diagnostic reliability of 48–77%. As a result, the diagnosis of Amyand's hernia is often made intraoperatively [2, 13, 15, 20-27].
To guide the surgical management of Amyand's hernia, in 2008 Losanoff and Basson proposed a classification system with four types:
- Type 1: Amyand's hernia with a normal appendix;
- Type 2: Amyand's hernia with acute appendicitis confined to the hernia sac;
- Type 3: Amyand's hernia with acute appendicitis and peritonitis;
- Type 4: Amyand's hernia with acute appendicitis and associated abdominal pathology (e.g., diverticulitis, colon cancer, mucocele, pseudomyxoma peritonei).
In Type 1 cases, hernioplasty with permanent mesh via inguinotomy is recommended, and the decision to perform an appendectomy should be based on factors such as patient age and lifelong risk of developing acute appendicitis. For all other types, urgent appendectomy is essential to ensure adequate septic source control. In cases of significant surgical field contamination (Type 3 and 4), a laparotomy may be required, and the use of prosthetic mesh should be carefully considered due to the high risk of infection [2, 28].
The case we reported is the first to our knowledge of a type 2 Amyand’s hernia in a chirrhotic patient. For this reason it has been a diagnostic and therapeutic challenge, because ascites could constitute a confounding factor for diagnosis on the one hand, and on the other hand cirrhosis could increase patient’s risk for both septic event and hernia recurrence.
Conclusion
Acute appendicitis in an Amyand’s hernia is a rare condition and constitutes both a diagnostic and therapeutic challenge for acute care surgeons, and underlying conditions may complicate its management.
Authors’ Contribution
M.C. and M.M. writing of the first draft, data collection; M.B. and P.B. critical revision and final approval.
Research Support
This research received no external financial or non-financial support.
Relationships
There are no additional relationships to disclose.
Patents and Intellectual Property
There are no patents to disclose.
Other Activities
There are no additional activities to disclose.
References
[1] Michalinos A, Moris D, Vernadakis S (2014) Amyand’s hernia: a review. Am J Surg 207:989–995.
[2] Ivanschuk G, Cesmebasi A, Sorenson EP et al (2014) Amyand’s hernia: a review. Med Sci Monit 20:140–146.
[3] Saylam B, Gu¨lseren MO, C¸ omc¸ali B et al (2013) Amyand’s hernia: really a rare condition. Am Surg 79:443–444.
[4] Cigsar EB, Karadag CA, Dokucu AI (2016) Amyand’s hernia: 11 years of experience. J Pediatr Surg 51:1327–1329.
[5] Erdog?an D, Karaman I?, Aslan MK et al (2013) Analysis of 3776 pediatric inguinal hernia and hydrocele cases in a tertiary center. J Pediatr Surg 48:1767–1772.
[6] Kaymakci A, Akillioglu I, Akkoyun I et al (2009) Amyand’s hernia: a series of 30 cases in children. Hernia 13:609–612.
[7] Okur MH, Karac¸ay S, Uygun I et al (2013) Amyand’s hernias in childhood (a report on 21 patients): a single-centre experience. Pediatr Surg Int 29:571–574.
[8] Sharma H, Gupta A, Shekhawat NS et al (2007) Amyand’s hernia: a report of 18 consecutive patients over a 15-year period. Hernia 11:31–35.
[9] Inan I, Myers PO, Hagen ME et al (2009) Amyand’s hernia: 10 years’ experience. Surgeon 7:198–202.
[10] Cankorkmaz L, Ozer H, Guney C et al (2010) Amyand’s hernia in the children: a single center experience. Surgery 147:140–143.
[11] Gurer A, Ozdogan M, Ozlem N et al (2006) Uncommon content in groin hernia sac. Hernia 10:152–155.
[12] Valioulis I, Papageorgiou I, Ioannidou D (2019) The clinical significance of an incidentally detected open internal inguinal ring. J Pediatr Urol 15:185.e1-185.e5.
[13] Meinke AK (2007) review article: appendicitis in groin hernias. J Gastrointest Surg 11:1368–1372.
[14] Breitenstein S, Eisenbach C, Wille G, et al. Incarcerated vermiform appendix in a left-sided inguinal hernia. Hernia 2005;9:100–2.
[15] Patoulias D, Kalogirou M, Patoulias I (2017) Amyand’s Hernia: an Up-to-date review of the literature. Acta Medica 60:131–134.
[16] Gurer A, Ozdogan M, Ozlem N et al (2006) Uncommon content in groin hernia sac. Hernia 10:152–155.
[17] Laermans S, Aerts R, De Man R. Amyand’s hernia: inguinal hernia with acute appendicitis. JBR-BTR Organe Soc R Belge Radiol SRBR Orgaan Van K Belg Ver Voor Radiol KBVR 2007;90:524–5.
[18] Ali SM, Malik KA, Al Qadhi H. Amyand’s hernia: study of four cases and literature review. Sultan Qaboos Univ. Med. J. May 2012, 12(2):232–236.
[19] Ash L, Hatem S, Ramirez GA, Veniero J. Amyand’s hernia: a case report of prospective CT diagnosis in the emergency department. Emerg. Radiol. June 2005, 11(4):231–2.
[20] Weber RV, Hunt ZC, Kral JG (1999) Amyand’s hernia: etiologic and therapeutic implications of two complications. Surg Rounds 22:552–556.
[21] Constantine S (2009) Computed tomography appearances of Amyand hernia. J Comput Assist Tomogr 33:359–362.
[22] Maizlin ZV, Mason AC, Brown C et al (2007) CT findings of normal and inflamed appendix in groin hernia. Emerg Radiol 14:97–100.
[23] Namdev GH, Sanjay P, Varun S, et al. Amyand’s hernia: a case report. Int Surg J 2020;7:2072.
[24] Morales-Cárdenas A, Ploneda-Valencia CF, Sainz-Escárrega VH, et al. Amyand hernia: case report and review of the literature. Ann Med Surg 2015;4:113–5.
[25] Bhatti SI, Hashmi MU, Tariq U. Amyand’s Hernia: A Rare Surgical Pathology ofvthe Appendix. Cureus, 2018.
[26] Baldassarre E, Centonze A, Mazzei A, Raffaella Rubino. Amyand’s hernia in premature twins. Hernia October 2008, 13(2):229–230.
[27] D’Alia C, Lo Schiavo MG, Tonante a. et al. Amyand’s hernia: case report and review of the literature. Hernia 7, 89–91 (2003).
[28] Losanoff JE, Basson MD (2008) Amyand hernia: a classification to improve management. Hernia 12:325–326.

Figure 1

Figure 2

Figure 3
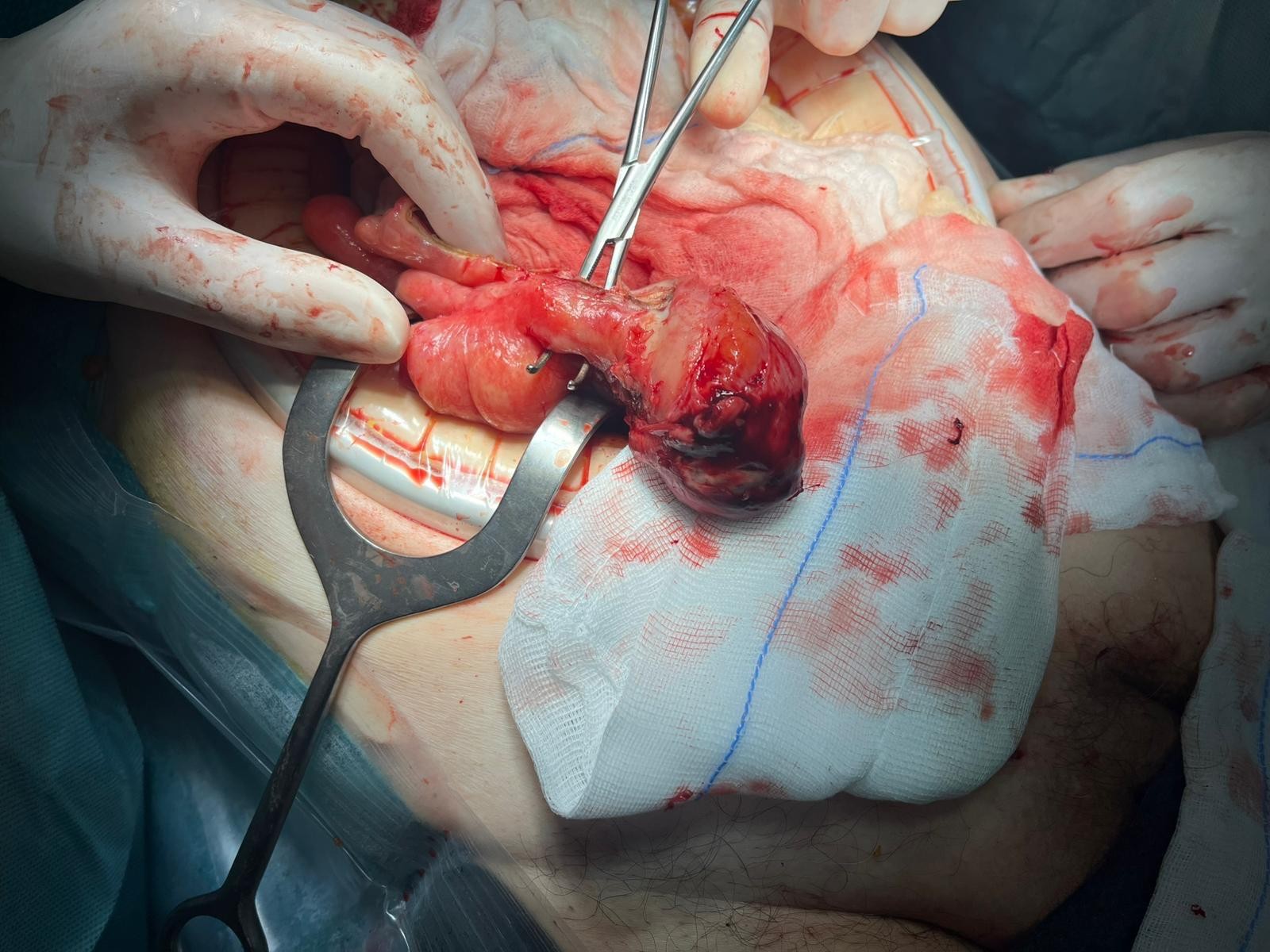
Figure 4