Endometriosis of the Sigmoid Colon Presenting as Colitis or Malignancy with Bowel Obstruction: Two Surgical Case Reports.
Endometriosis of the Sigmoid Colon Presenting as Colitis or Malignancy with Bowel Obstruction: Two Surgical Case Reports.
Valeriia Skurtol 1*, Giovanni D. Giannotti 2, Timothy J. Heilizer 3, Omid Rouhi 4, Zaria Giannotti Frye5
1. Valeriia Skurtol, MD, Resident of Family Medicine Program, Prime Health St. Mary, Chicago, IL
2. Giovanni D. Giannotti, MD, FACS, FSSO, General Surgeon and Fellowship-Trained Surgical Oncologist, St. Mary Hospital, Chicago, IL
3. Timothy J. Heilizer, MD, Colon & Rectal Surgeon, Chicago, IL
4. Omid Rouhi, MD, PhD, Medical Director of Pathology, Prime Health St. Mary, Chicago, IL
5. Zaria Giannotti Frye, Medical Student at The University of Illinois Urbana-Champaign.
*Correspondence to: Valeriia Skurtol, MD, Resident of Family Medicine Program, Prime Health St. Mary, Chicago, IL.
Copyright
© 2025 Valeriia Skurtol. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 20 May 2025
Published: 02 June 2025
Endometriosis of the Sigmoid Colon Presenting as Colitis or Malignancy with Bowel Obstruction: Two Surgical Case Reports.
Background
Endometriosis is a chronic gynecological condition characterized by the presence of endometrial-like tissue outside the uterus, often causing pain, infertility, and gastrointestinal symptoms like constipation. While intestinal involvement is less common, it can, in rare cases, lead to bowel obstruction. The prevalence of intestinal endometriosis ranges from 3% to 37% of all cases, with bowel obstruction due to endometriosis being particularly rare, occurring in 0.1% to 0.7% of cases. The most common sites of intestinal involvement include the ileum 38.3%, rectosigmoid 34.5%, ileocecal junction and appendix 14.9%, and rectum 10.2%. (1)
We present two cases whose endometriosis involved the sigmoid colon, mimicking as a colitis or malignancy with primary bowel obstruction, required surgival interventions and histopathology confirmation to the origin of tissue.
Case Presentation
Case 1
A 44-year-old woman presented to the emergency department with diffuse abdominal pain for four days, accompanied by vomiting. She had a limited gynecological history but a significant history of chronic constipation, previously managed with Miralax.
An initial CT scan showed an irregular soft tissue mass with luminal narrowing in the sigmoid colon, causing, raising concern for colonic obstruction, possibly due to malignancy.
An initial colonoscopy demonstrated a non-traversable extrinsic stenosis at the sigmoid colon. A laparoscopic procedure was performed, including lysis of extensive adhesions and creation of a loop transverse colostomy. A follow-up colonoscopy via the ostomy confirmed severe extrinsic stenosis (4 mm internal diameter), and abnormal mucosa was noted.
Definitive surgery included laparoscopic sigmoid and rectal resection with mobilization of the splenic flexure. Final pathology revealed endometriosis involving the rectosigmoid colon with no malignancy. The mass measured 4.2 × 1.6 × 1.5 cm, involving the submucosa and muscularis propria. The patient was discharged after recovery with complete resolution of symptoms.A second case:
Case 2
A 35-year-old woman presented to the emergency department presented with acute abdominal pain for 2 days and bright red blood per rectum to ED. Has history of dysmenorrhea and chronic constipation managed with OTC medication and alpha thalassemia. She previously used a NuvaRing and recently had a Paragard IUD placed.
CT imaging showed sigmoid colon wall thickening, a 2.0 × 1.6 × 1.0 cm intramural abscess, and free adnexal fluid, raising suspicion for colitis or inflammatory bowel disease with possible gynecologic etiology.
A robotic-assisted sigmoid colectomy, appendectomy, and lysis of adhesions were performed using the da Vinci® system. Intraoperatively, extensive adhesions and black speck-like endometrial implants were visualized throughout the pelvis. The sigmoid colon was indurated and adherent to the uterus and adnexa. The appendix also appeared indurated and was removed.
Histopathology confirmed endometriosis in both the sigmoid colon and appendix. The patient recovered well postoperatively and was discharged on postoperative day five, with complete resolution of her symptoms. She was referred for further gynecologic management of endometriosis.
Conclusions
Endometriosis involving the large bowel is exceedingly rare, and diagnosing bowel obstruction due to endometriosis preoperatively is challenging. Although, bowel obstruction due to endometriosis should be considered in reproductive-aged women presenting with gastrointestinal symptoms, especially in those with a history of dysmenorrhea or cyclic worsening of constipation.
Background
Endometrial tissue typically occurs in the peritoneum, ovaries, fallopian tubes, and other pelvic organs. Large bowel occlusion due to endometriosis is rare, with a prevalence of 0.1% to 0.7%. In this report, we describe a case where endometrial tissue infiltrated the sigmoid colon and appendix, presenting as bowel colitis with sympoms and radiographic findings of obstruction.
Case Report
A 35-year-old woman with a history of dysmenorrhea and chronic constipation presented with acute abdominal pain to ED . Her symptoms on presentation diffuse abdominal pain, nausea, vomiting, diarrhea, chills, and bright red blood per rectum. She had a history of alpha thalassemia, dysmenorrhea fo that she was initially on NuvaRing since 2018, later switching to ParagardIUD placed 2024. Patient was complaining for consitpaiton with mild relief from magnesium citrate and prune juice and other OTC medications. A CT scan of abodmen with conatrast revealed sigmoid colonic wall thickening with small intramural abscess measuring up to 2.0 x 1.6 x1.0 cm., concerning for colitis of infectious or inflammatory origin and adnexal free fluid, raising the possibility of gynecological pathology. CBC remarkable for mildly low white count of 13.4, CMP was normal.
A robotic sigmoid colon resection, appendectomy, and lysis of adhesions were performed using the da Vinci® system. Extensive adhesions were noted throughout the abdominal wall. During surgery, endometriosis was identified macroscopically, by OB-GYN, descirbe as black specks. There was evidence of endometriosis throughout the pelvis. The sigmoid colon found to be indurated and adherent to the uterus and adnexa, afther adheiolysis the colon resected and sent to pathology. Appendix apearred also indurated.
Histopathological examination revealed endometrial tissue in both the appendix and sigmoid colon. The patient was discharged five days postoperatively without complications, and her bowel symptoms resolved. Follow-up was recommended for ongoing management of endometriosis.
Fig. 1 Abdominal computed tomography showed irregularly enhanced wall thickening with suspected intrmural abcess measuring up to 2.0 cm of the sigmoid colon (white-black arrow). tranverse view
Fig. 2 Abdominal computed tomography showed irregularly enhanced wall thickening of mass in the sigmoid colon (white-black arrow). Sagital view
Fig. 3 Resected specimen of sigmoid colon with black peaks (black arrow)
Fig. 4 Histopathological examination showed endometrial glands in the middle of muscle layer of sigmoid colon (×100) (Stars pointed)
Fig. 5 Histopathological examination showed endometrial gland in the middle of muscle layer of sigmoid colon in diffrent slides (×100) (arroows pointed)
Discussion
Endometriosis is a chronic condition defined by the presence of functional endometrial tissue consisting of glands and stroma outside the uterus. It affects 4 to 17% of women of reproductive age (7), or roughly 10% (190 million) of women and girls globally (8). Gastrointestinal involvement occurs in 3%-37% of cases (9). Common clinical presentations include pelvic pain, infertility, and dyspareunia, but it may also be nonspecific (5).
The term endometriosis was first introduced by John Sampson in 1927, who described the presence of endometrial glands and stroma within ovarian cysts, commonly referred to as “chocolate cysts” or ovarian endometriomas (11). His foundational work laid the basis for understanding the ectopic behavior of endometrial tissue and remains central to the modern conceptualization of the disease.
The most widely accepted pathophysiological explanation is Sampson’s theory of retrograde menstruation (1940), which proposes that endometrial tissue refluxes through the fallopian tubes during menstruation, subsequently implanting on pelvic organs. (4).
In our last case, patient had a longstanding history of dysmenorrhea and constipation that worsened with her menstrual cycle. She had never been pregnant and had used hormonal contraception for extended periods to manage her symptoms. The cyclical nature of her gastrointestinal complaints—particularly the recurrence of pain with menstruation—served as a key diagnostic clue. However, involvement with large bowel occlusion is remains rare, with a prevalence of 0.1-0.7% (1, 9). In rare instances, transmural endometriosis can lead to intestinal perforation (10), involving sites such as the colon and appendix.
Preoperative diagnosis is challenging due to overlapping clinical presentations with other GI conditions, including inflammatory bowel disease, neoplasms, and colitis. Imaging workup may be inconclusive and may sometimes mimicking infectious or inflammatory colitis. Gastrointestinal endometriosis is usually found as an incidental finding during abdominal exploration. Diagnostic laparoscopy is considered the gold standard for diagnosing endometriosis, with or without histologic verification (2).
In our case, robotic surgery allowed for the effective resection of concerning lesions and removal of the source of inflammation (6), with the tissue sent to histopathology for confirmation of the diagnosis. Intraoperatively, the OB-GYN was able to confirm the diagnosis by identified classic endometriotic implants—described as "black specks" in the pelvic area (Fig. 3). It is now also called pigmented endometrial plaques due to the accumulation of old blood, which typically appears as black or dark-colored spots. These are referred to as "powder-burn lesions," containing hemosiderin-laden tissue embedded with inactive endometriotic glands and fibrous stroma (3).
The diagnosis was confirmed with histopathology (Fig. 4-5), showing endometrial glands within the muscular layer of the sigmoid colon. Postoperatively, the patient made a full recovery, reporting no further abdominal symptoms. Ongoing postoperative management of endometriosis includes hormonal therapy with an IUD which was placed in 2023. The patient continues follow-up visits with her OB-GYN for further care and symptom control.
Conclusions
These cases underscore the rare but significant occurrence of endometriosis involving the sigmoid colon, presenting with symptoms and imaging findings that can closely mimic colitis or colorectal malignancy. Accurate diagnosis requires a high level of suspicion, especially in women with a history of dysmenorrhea or chronic gastrointestinal symptoms. A combination of clinical evaluation, imaging, and definitive histopathological confirmation is essential. While surgical resection may be necessary for diagnosis or when conservative management fails, long-term gynecologic follow-up is crucial to address underlying endometriosis and reduce the risk of recurrence.
References
1. Mu?at F, P?duraru DN, Bolocan A, Constantinescu A, Ion D, Andronic O. Endometriosis as an Uncommon Cause of Intestinal Obstruction-A Comprehensive Literature Review. J Clin Med. 2023 Oct 6;12(19):6376. doi: 10.3390/jcm12196376. PMID: 37835020; PMCID: PMC10573381.
2. Agarwal, Sanjay K. et al. Clinical diagnosis of endometriosis: a call to action. American Journal of Obstetrics & Gynecology, Volume 220, Issue 4, 354.e1 - 354.e12
3. Freddy J. Cornillie, Didier Oosterlynck, Joseph M. Lauweryns, Philippe R. Koninckx, Deeply infiltrating pelvic endometriosis: histology and clinical significance, Fertility and Sterility; Volume 53, Issue 6, 1990, Pages 978-983, ISSN 0015-0282
4. Quinn M. Endometriosis: the consequence of neurological dysfunction? Med Hypotheses. 2004;63(4):602-8. doi: 10.1016/j.mehy.2004.03.032. PMID: 15325003.
5. Lin YH, Kuo LJ, Chuang AY, Cheng TI, Hung CF. Extrapelvic endometriosis complicated with colonic obstruction. J Chin Med Assoc. 2006 Jan;69(1):47-50. doi: 10.1016/S1726-4901(09)70111-X. PMID: 16447927.
6. Lin YH, Kuo LJ, Chuang AY, Cheng TI, Hung CF. Extrapelvic endometriosis complicated with colonic obstruction. J Chin Med Assoc. 2006 Jan;69(1):47-50. doi: 10.1016/S1726-4901(09)70111-X. PMID: 16447927.
7. Bianchi A, Pulido L, Espín F, Hidalgo LA, Heredia A, Fantova MJ, Muns R, Suñol J. Endometriosis intestinal. Estado actual [Intestinal endometriosis. Current status]. Cir Esp. 2007 Apr;81(4):170-6. Spanish. doi: 10.1016/s0009-739x(07)71296-4. PMID: 17403352.
8. WHO. Endomentriosis. 24 March 2023
9. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertil Steril. 1997 May;67(5):817-21. doi: 10.1016/s0015-0282(97)81391-x. PMID: 9130884.
10. Floberg J, Bäckdahl M, Silferswärd C, Thomassen PA. Postpartum perforation of the colon due to endometriosis. Acta Obstet Gynecol Scand. 1984;63(2):183-4. doi: 10.3109/00016348409154658. PMID: 6730932.
11. Edited by Liselotte Mettler, Ibrahim Alkatout, Jörg Kecksteinc and Ivo Meinhold-Heerleind. Endometriosis: A concise practical guide to current diagnosis and treatment. 2018, Journal of the Turkish-German Gynecological Association.

Figure 1
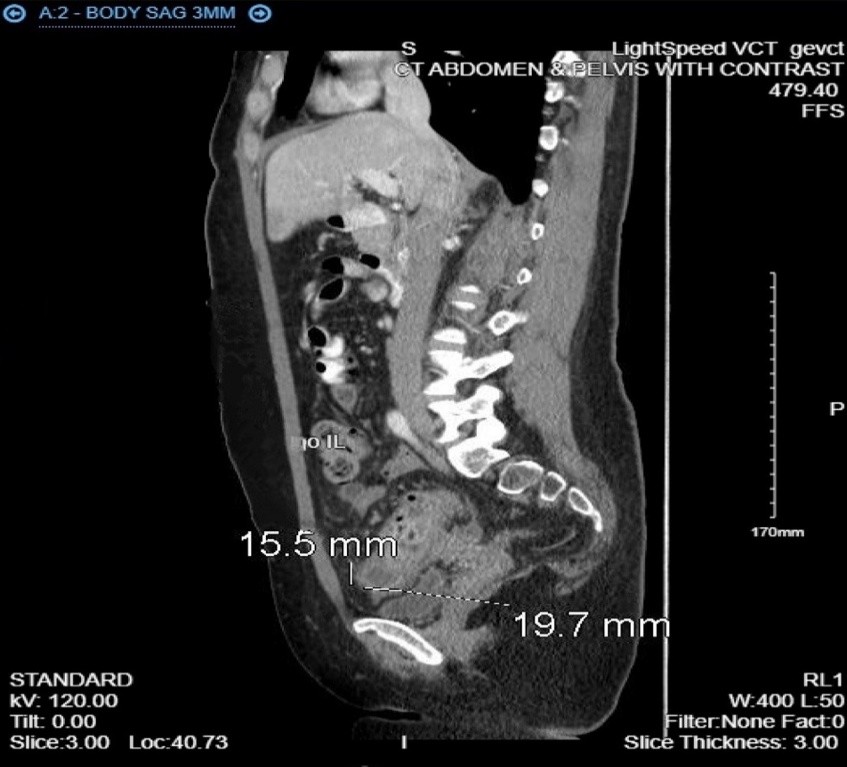
Figure 2
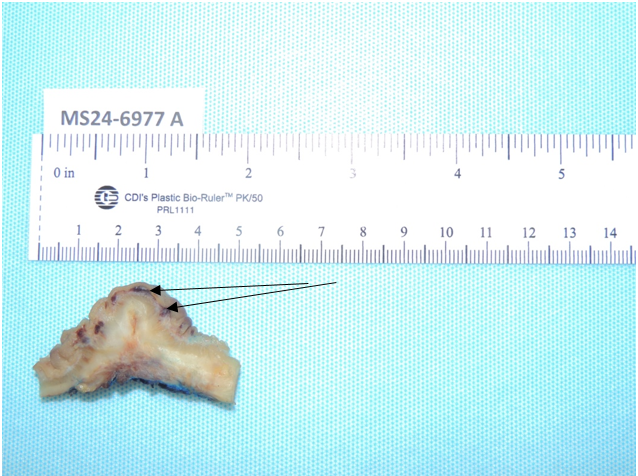
Figure 3
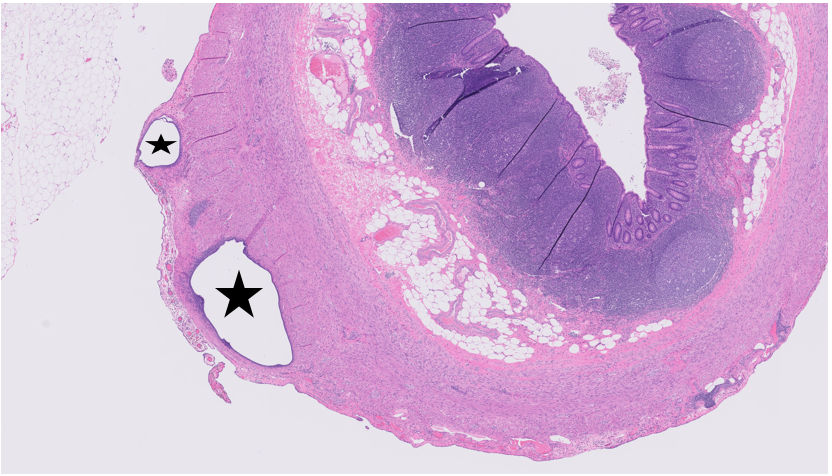
Figure 4
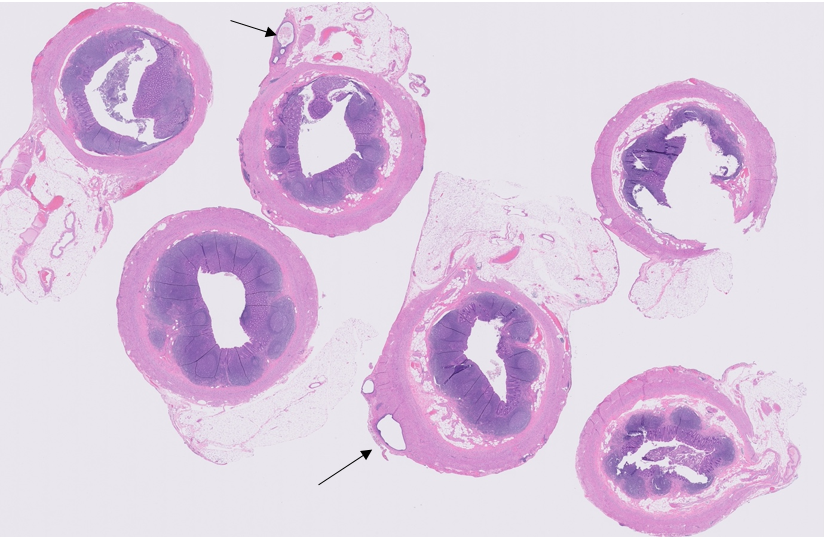
Figure 5