Ultrahypofractionated Radiotherapy in Early Breast Carcinoma-A Tertiary Cancer Centre Experience
Ultrahypofractionated Radiotherapy in Early Breast Carcinoma-A Tertiary Cancer Centre Experience
Dr.Priya Philip DMRT,DNB1*, Dr.A.N.Vaidhyswaran MD,DMRT2 , Dr.Aswin.A.N MD3 , Dr.Smruthi DNB4
1. Associate Consultant, Department of Radiation Oncology, Kauvery Hospital, Alwarpet, Chennai, Tamil Nadu, India.
2. Senior Consultant, Head and Director, Department of Radiation Oncology, Kauvery Hospital, Alwarpet, Chennai, Tamil Nadu, India.
3. Senior Consultant, Department of Radiation Oncology, Kauvery Hospital, Alwarpet, Chennai, Tamil Nadu, India.
4. Registrar, Department of Radiation Oncology, Kauvery Hospital, Alwarpet, Chennai, Tamil Nadu, India.
*Correspondence to: Dr.Priya Philip DMRT,DNB, Department of Radiation Oncology, Kauvery Hospital, Luz Church road, Mylapore, Chennai, Tamil Nadu, India.PIN code-600018
Copyright.
© 2025 Dr.Priya Philip This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 June 2025
Published: 16 June 2025
DOI:https://doi.org/10.5281/zenodo.15686581
Abstract
AIM: Carcinoma breast is a major public health problem today being the most commonly occurring cancer in women and second most common cancer worldwide. Conventional fractionation regimen for adjuvant radiotherapy was a total dose of 45 to 50 Gy in 25 fractions or daily doses of 1.8 Gy to 2 Gy, patients were treated from Monday to Friday for a total duration of treatment being five weeks. With the introduction of UK START trials (START A and START B), hypofractionated radiotherapy schedules came into practice, thus shortening the treatment period to three weeks. In 2020, the five year results of ultra hypofractionated radiotherapy for 1 week versus 3 weeks (FAST FORWARD trial) were published. The multicentre, randomised phase three trial proved non inferiority of 26Gy in 5 fractions schedule compared to the standard 40Gy in 15 fractions schedule in terms of local control and normal tissue toxicity for adjuvant radiotherapy in early breast cancer patients.The aim of our study is to highlight the feasibility of ultrahypofractionated radiotherapy in Indian scenario with respect to tumour control and normal tissue toxicity.
PATIENTS AND METHODS: The data of 50 female patients with early breast cancer (Stage I & II) treated in our hospital from April 2022 to December 2023 were analysed. The median age of the patients was 59years (30-86). 54% of the patients were left sided and 46% of the patients were right sided cancers. 74% of the patients were hormone positive.43 (86%) underwent Breast Conservation Surgery (BCS) and 7(14%) underwent Mastectomy with axillary surgery .11(25.5%) patients among the BCS group received Tumour Bed Boost(10Gy in 5 fractions). All the patients received a dose of 26 Gy in 5 fractions with or without boost dose according to the protocol using 3D conformal therapy field in field technique. The patients were followed up for tumour control and normal tissue toxicity.
RESULTS : All the 50 patients (100%) developed Grade I skin reactions and 8 (16%) patients had mild breast discomfort. No major acute toxicities were encountered during the treatment and follow-up. The breast cosmesis was well maintained and there was no evidence of disease recurrence during the follow-up period. All the patients are being constantly followed up for late toxicities.
CONCLUSION: Ultrahypofractionated radiotherapy for early breast cancer is a feasible modality in our Indian scenario. Acute toxicities were not seen except mild erythema, we need to follow-up the patients for any late toxicities before making this protocol as the standard of care in our setting.
Keywords: Ultrahypofractionated radiotherapy, FAST FORWARD, Early breast cancer, Breast conservation surgery, mastectomy, Tumour bed boost
Ultrahypofractionated Radiotherapy in Early Breast Carcinoma-A Tertiary Cancer Centre Experience
Introduction
Carcinoma breast is a major public health problem today being the most commonly occurring cancer in women and second most common cancer worldwide. According to the Globocan data 2022, breast cancer accounted for 11.6% of all cancer cases and 6.9% of all death. (1) Population based cancer registries provide information of the cancer burden in India. According to the data,breast cancer accounted for 21.8% of the total cancer burden in women as measured by DALYs (Disability-Associated Life Years). According to the projections, the burden of female breast cancer in India in 2025 is expected to be 5.6 million DALYs. (2).Multidisciplinary approach to breast cancer is needed to reduce the incidence, morbidity and mortality due to the disease. This comprises of educational programs for preventive measures, screening programs for early detection and availability of comprehensive cancer care facilities for women all over the nation.
All patients with early breast carcinoma undergo breast conservation surgery.If systemic therapy is warranted, patients receive neoadjuvant chemotherapy prior to surgery which is currently the standard of care.Triple negative,Her-2-neu positive,high risk hormone positive patients need chemotherapy.Clinically high risk but genomically low risk patients can avoid systemic therapy.These patients need to undergo tests like Mammaprint or Oncotype Dx to be considered as low risk for recurrence(3).Some patients prefer mastectomy.Early breast carcinoma patients who undergo lumpectomy and axillary surgery requires adjuvant radiotherapy to the whole breast. Conventional fractionation regimen was a total dose of 45 to 50 Gy in 25 fractions or daily doses of 1.8 to 2 Gy.Patients were treated from Monday to Friday for a total duration of five weeks. With the introduction of UK START trials (START A and START B), hypofractionated radiotherapy schedules came into practice, thus shortening the treatment period to three weeks.(4) During and after the COVID pandemic era, hypofractionated radiotherapy is the treatment of choice for many sites. In 2020 , the five year results of ultra hypofractionated radiotherapy for 1 week versus 3 weeks (FAST FORWARD trial) were published. The multicentre, randomised phase three trial proved non inferiority of 26Gy in 5 fractions schedule compared to the standard 40Gy in 15 fractions schedule in terms of local control and normal tissue toxicity for adjuvant radiotherapy in early breast cancer patients. (5)
Materials and Methods
At our institute, we retrospectively analysed the case records of 50 patients with early breast cancer who underwent either breast conservation surgery or mastectomy ,followed by adjuvant radiotherapy with 26 Gy in five fractions schedule with or without a boost dose of 10Gy in five fractions to the lumpectomy cavity from the period of April 2022 to December 2023 .The study was approved by the Institute Ethics Committee -IEC number-ECR/966/INST/TN2017/RR-21(The Institutional Ethics Committee,functions as per the requirements of the ICH-GCP,ICMR 2019,NCDT 2019 guidelines and SOPs).The patient characteristics,surgery,chemotherapy and radiotherapy details were abstracted from the case records.Female patients aged more than 18 years with histopathologically proven invasive carcinoma breast ,who underwent breast conservation surgery or mastectomy along with axillary surgery ,stages pT1-3N0-1 M0 ,ECOG performance status 0-2.50 patients who presented in radiation oncology department between April 2022 and December 2023 were selected for the study.
Immobilization technique:
All the patients underwent immobilization using custom made thoracic thermoplastic device in supine position with arms abducted. Shoulders and arms were immobilized using either arm rest or vacloc device.
CT simulation:
All patients underwent CT simulation on GE revolution 128 slice machine with or without intravenous contrast. Borders of the breast or chestwall were marked with lead wires. Simulation CT was taken in 2.5mm slices from upper neck to mid abdomen.A full 3D set of outlines covering the area of interest were obtained.
Delineation of target volumes and organs at risk:
The clinical target volume and planning target volumes were contoured primarily according to ESTRO guidelines.(6,7)Organs at risk were contoured based on RTOG guidelines. Modifications were made according to the fast forward planning pack.(8)
Contouring of target volumes:
CTV-whole breast: the CTV includes soft tissues of the whole breast from 5 mm below the skin surface posteriorly upto the deep fascia, excluding muscle and underlying rib cage. The posterior margin does not extend beyond the deep fascia and should be 5 mm anterior to the lung/chest wall interface. CTV-whole breast should not extend beyond the edges of the visible/palpable breast in medial and lateral directions. CTV-chestwall: encompasses the skin flaps and includes the soft tissues down to the deep fascia, excluding the underlying muscle and rib cage. CTV-boost : tumour bed marked by surgical clips or seroma cavity along with areas of abnormal breast architecture.Indications for lumpectomy boost selected were young age(<50 years),high grade and positive margins.PTV-whole breast: CTV-whole breast+10mm margin. PTV is cropped 5mm from skin surface and 5mm from the lung surface.PTV-chestwall: CTV-chestwall+10mm margin .The PTV is then cropped 5 mm inside the skin or along the skin and 5 mm from the lung surface for dose reporting purposes. PTV-boost: CTV-boost+10mm margin.The region extending outside the PTV-whole breast is cropped (Picture 1 and Picture 2).
Picture 1-Planning target volume in chestwall radiotherapy case
Picture 2-Planning target volume in whole breast radiotherapy case
Contouring of normal organs:
Ipsilateral lung: the whole lung is contoured as a single structure.It excludes the main airways and vasculature.
Heart: the heart is contoured in its entirety including the pericardium.It does not include the major blood vessels.The contour extends superiorly upto the slice where the right pulmonary artery and pulmonary trunk are seen as separate structures.(9)
Radiotherapy planning and plan evaluation
Beam arrangements:
A forward planning 3D-CRT technique was used for radiotherapy planning.The treatment planning software was Eclipse version 13.6 with AAA algorithm. A primary pair of tangential beams with a field in field technique using a few subfields of variable beam weightage were utilised to get a homogenous dose distribution and conformity. Photons beams of 6MV energy were used in all our cases. The isocentre was placed at the centre of whole breast PTV or on the centre of the tumour bed. Weightage of beams were modified and adjusted so that adequate dose coverage was ensured to the target volume without creating hotspots outside.MLC shaping helps in shielding of heart and lung( Picture 3).
For the boost planning multiple mini tangential and oblique subfields were used.
Picture 3-Radiotherapy beam arrangements
Dose prescription
Target volumes:PTV breast and PTV-chestwall-26Gy in 5 fractions,5.2Gy per fraction.Duration of treatment was one week.The boost dose to lumpectomy cavity was 10Gy in 5 fractions ,so the total duration for treatment was two weeks.
Normal organs at risk:
The main organs considered were ipsilateral lung and heart.The dose constraint was given as V8Gy≤15% for ipsilateral lung.For heart the constraints were V1.5Gy≤30% and V7Gy≤5%.
An alternative was also suggested regarding the mandatory and optimal dose to the organs at risk.It is given below:
(Table-1)
Table-1:Dose constraints for organs at risk
|
|
Mandatory |
Optimal |
|
Ipsilateral lung |
V30%≤17% |
V30%≤15% |
|
Heart |
V25%≤5% V5%≤25% |
|
Plan evaluation
Multiple plans were made for each patient ensuring maximum dose coverage to the planning target volume,minimizing dose to heart and lung according to the fast forward protocol.The ideal dose coverage for 95% of the target volume is 95% of the dose. The best plan was selected by the radiation oncologist and was executed (Picture 4).
Picture 4-95% dose distribution curve
The following criteria for dose coverage were given as per the fast forward planning pack protocol to get the optimum results.(Table-2).The final decision is taken by the oncologist prioritising normal tissue dose constraints over the target coverage constraints. Medical physicists aimed at reducing the amount of lung and heart in the treated area by MLC shielding on the tangential fields and also by shifting the field borders according to the particular case without compromising the position of the area of interest.(8)
Table-2:Criteria for plan evaluation
|
|
MANDATORY |
OPTIMAL |
|
LOWER LIMIT |
V95%≥90% |
V95%≥95% |
|
UPPER LIMIT |
V105%≤7% V107%≤2% Dmax≤110% |
V105%≤5% |
Treatment execution and daily treatment verification
The patients were treated on Varian truebeam 120 MLC machine.Barrier film spray was used on the breast or chestwall skin prior to each treatment session as per the department protocol aiming at reduction of acute radiation dermatitis. Daily onboard image verification was ensured with KV images and cone beam CT scan (Picture 5).Portal images were also taken to confirm the central lung distance from the posterior edge of the tangential field.Patients were educated well on skin care during the course of radiotherapy and during the follow up period.On the final day of radiotherapy,patients were clinically assessed along with photographic documentation .All patients were advised to apply betamethasone ointment all over the irradiated area two times daily for two weeks.
Picture 5-Daily onboard imaging
Follow up
All patients were followed up at regular intervals.First review after the completion of treatment was at 4 weeks ,followed by every three months for the first two years.Every time the patient was evaluated for any pain,discomfort or skin changes and recorded.
Results
Our retrospective analysis included 50 early breast cancer patients among which 43 patients had undergone breast conservation surgery and 7 had mastectomy.The median age of the patients was 59 years (30 to 86 years of age). 54% of the patients were left sided and 46% of the patients were right sided cancers. 32 patients received chemotherapy either neoadjuvantly or adjuvantly.Out of the 43 patients who underwent whole breast radiotherapy,11 patients received a lumpectomy cavity boost to a dose of 10Gy in 5 fractions.
The distribution of our patient data are as follows:
Table -3:Distribution of patients stage-wise
|
Breast cancer stage |
Number of patients (%) |
|
I |
18(36%) |
|
IIA |
23(46%) |
|
IIB |
9(18%) |
Table -4:Age distribution of patients
|
Age distribution |
Number of patients(%) |
|
≤ 40 years |
2(4%) |
|
41-50 years |
7(14%) |
|
51-60 years |
15(30%) |
|
61-70 years |
19(38%) |
|
> 70 years |
7(14%) |
Table-5:Number of patients receiving whole breast vs chestwall radiotherapy
|
Number of patients receiving radiation to whole breast(%) |
Number of patients receiving radiation to chestwall(%) |
|
43(86%) |
7(14%) |
Table-6:Distribution of patients based on hormone receptors and Her-2-neu status
|
Hormone receptor status |
Number of patients(%) |
|
HR positive,Her-2-neu-negative |
37(74%) |
|
HR positive,Her-2-neu-positive |
2(4%) |
|
HR negative,Her-2-neu-positive |
4(8%) |
|
Triple negative |
7(14%) |
Table-7:Patients who received chemotherapy
|
Patients received chemotherapy (%) |
Patients did not receive chemotherapy(%) |
|
32(64%) |
18(36%) |
Patients were taken for radiotherapy treatment once all the criteria regarding the target volume coverage and normal tissue constraints were met.All 50 patients received adjuvant radiotherapy to a dose of 26Gy in 5 fractions to the breast or chestwall over a period of 5 days along with daily image guidance.10patients received a boost dose of 10Gy in 5 fractions to the lumpectomy cavity.
Patients were evaluated for any skin changes,breast or chestwall pain and discomfort.Photographic records were made before the initiation and at the end of treatment.Radiation induced skin reactions were graded according to the CTCAE v5.0 criteria.(10).All patients are on regular follow up till date.
Observation
All patients tolerated the radiotherapy treatment with minimal toxicity.Patients had grade I skin reactions at the end of course.The skin became normal in colour and texture within two months.Few patients had slight breast discomfort or heaviness temporarily.None of the patients had local or distal recurrence during the study period.(Table 8 Table 9,Table 10)
Table 8:Acute toxicity during radiotherapy treatment
|
Acute toxicity |
Number of patients (%) |
|
Radiation dermatitis-grade I/ II |
50(100%) |
|
Radiation dermatitis-grade III/IV |
(0%) |
|
Breast or chestwall pain or tenderness |
(0%) |
|
Breast heaviness or discomfort |
8(16%) |
Table 9: Late toxicity after radiotherapy course
|
Late toxicity |
Number of patients(%) |
|
Fibrosis |
(0%) |
|
Pain or edema |
(0%) |
|
Hyperpigmentation |
(0%) |
Table 10: Late breast related events
|
Event |
Number of patients(%) |
|
Ipsilateral or contralateral tumour recurrence |
(0%) |
|
Distal relapse |
(0%) |
Discussion
Carcinoma breast has become the most common malignancy in women all around the world.In the earlier times,lung cancer presented a higher incidence which is now exceeded by breast cancer.Many epidemiological studies and statistics have revealed that the disease burden caused by breast cancer globally will continue to increase and cross almost 2 million by the year 2030(11).Over the last 26 years, the age-standardised incidence rate of breast cancer in females increased by 39.1% (95% uncertainty interval, 5.1 to 85.5) from 1990 to 2016, with the increase observed in every state of the country.(12)Recent trends show that a higher proportion of the disease occurs at a younger age in Indian women, as compared to the Western population.
Early breast cancer includes DCIS, I,IIA,IIB stages .In the recent times more women present in early stages due to awareness about screening tests and self evaluation.Breast cancer has become a curable disease in a good number of patients,due to advancements in treatment modalities and systemic therapy including targeted therapy.Breast cancer patients occupy majority of any cancer department and large number of patients are being treated at any time.Adjuvant radiotherapy after lumpectomy forms an important part of breast conservation strategy.Breast irradiation prevents the need for mastectomy along with substantial decrease in local recurrence.High risk patients with tumours ≥ 5cm, ≥ 4 positive axillary lymph nodes and high grade of anaplasia benefit from radiotherapy after mastectomy in terms of locoregional control and overall survival.(13).Earlier trials of breast radiotherapy used conventional fractionation regimen of a total dose of 45 to 50 Gy given in 1.8 to 2Gy daily doses over 5 weeks. (14)(15).It was the international standard of practice since 1980s.
In a randomized trial J Roger Owen et al described that breast carcinoma is more sensitive to fraction size and the sensitivity is similar to late reacting normal tissues . Thus simpler treatment schedules can be used with fewer, larger fractions without compromising effectiveness or safety.(16) .Several trials came with multiple fractionation schedules using larger fraction size and lesser number of fractions assessing the safety profile and tumour control rates comparing to the conventional regimen.
The UK standardisation breast radiotherapy trial A (START A) tested two dose levels of a 13-fraction schedule against the standard regimen with the aim of measuring the sensitivity of normal and malignant tissues to fraction size. 2236 women with early breast cancer (pT1-3a pN0-1 M0) at 17 centres in the UK were randomly assigned after primary surgery to receive 50 Gy in 25 fractions of 2·0 Gy versus 41·6 Gy or 39 Gy in 13 fractions of 3·2 Gy or 3·0 Gy over 5 weeks.The primary endpoints of the study were locoregional relapse, late normal tissue effects and quality of life.After a median follow up of 5·1 years,the local recurrence rates of 13 fraction regimens were comparable with 25 fraction regimen.Photographic and patient self-assessments suggested lower rates of late adverse effects after 39 Gy than with 50 Gy. The hypothesis that breast cancer and the dose-limiting normal tissues respond similarly to change in radiotherapy fraction size was hence reconfirmed in the study. A lower total dose in a smaller number of fractions could offer similar rates of tumour control and normal tissue damage as the international standard fractionation schedule of 50 Gy in 25 fractions. (17).START B trial compared 50 Gy in 25 fractions of 2·0 Gy over 5 weeks or 40 Gy in15 fractions of 2·67 Gy over 3 weeks and the findings were similar .Local tumour control rates were similar and the late normal tissue effects were better with hypofractionated schedule(18)
Danish hypo trial was a non inferiority trial aimed at analysing the breast induration after hypofractionated radiotherapy.The cosmetic outcome and patient satisfaction noticed were better with the 40Gy schedule(19).Sooner hypofractionated radiotherapy protocol was adopted world wide and is the current schedule practised everywhere.Studies continued with further lesser fractions and larger fraction size,reducing 15 days course to 5 days course.
Fast trial compared conventional regimen of 50Gy in 25 fractions to weekly once 5 fraction regimens of 28.5Gy and 30 Gy in low risk patients(pT1-T2N0) aged ≥50 years,who underwent breast conservation surgery during the study period of 2004-2007.The results of 10 years were published.The primary end point was change in photographic breast appearance at 2 and 5 years; secondary end points were physician assessments of normal tissue effects and local tumour control. Most common effect was breast shrinkage.It increased over time along with telengectasia,but breast edema decreased gradually.Normal tissue effects were higher for 30Gy in 5 fractions patients ,but that of 28.5Gy in 5 fractions were compared to the 50Gy patients.Thus results confirm that once weekly five fraction schedule of adjuvant breast radiotherapy is radiobiologically comparable to a conventionally fractionated regimen for normal tissue adverse effects.(20)
In 2020 ,results of fast forward breast radiotherapy was published.It was a randomised phase 3,multicentre non inferiority trial based in UK comparing one week radiotherapy schedule delivering 27 Gy and 26 Gy in five fractions to the conventionally used three week schedule of 40Gy in 15 fractions to breast or chestwall after surgery.The aim of the trial was to establish that the one week radiotherapy was non inferior in terms of local control and safe considering the toxicity profile.Patients above 18 years with invasive carcinoma breast,stages (pT1–3, pN0–1, M0) after breast conservation surgery or mastectomy were selected for study. At a median follow-up of 71?5 months, HR was 0?86 for 27 Gy in five fractions and 0?67 for 26 Gy in five fractions compared to 40Gy in 15 fractions for primary endpoint (ipsilateral breast tumour relapse). At the end of study period of 5 years, moderate or severe normal tissue effects in the breast or chest wall was 9?9% for 40 Gy patients,15?4%) for 27 Gy patients and 11?9% for 26 Gy patients.Odds ratios were 1?55 for 27 Gy in five fractions and 1?12 for 26 Gy in five fractions comparing to 40 Gy patients.Patient and photographic assessments showed higher normal tissue effect risk for 27 Gy versus 40 Gy but not for26 Gy versus 40 Gy.It proved that fast forward protocol was non inferior within absolute safety margin of 1.6%, while taking 2 % as the IBTR for 3 week radiotherapy(5)
In 2020 and afterwards,need for shorter fractionated schedules became a necessity due to COVID pandemic.Adoption of fast forward protocol into our department programme was favourable in many aspects.In our institute experience, there has been a steady increase in cases of breast cancer patients over the past few years.Due to better awareness among general public,more early stage cancers are being detected recently.Also most of the patients prefer surgeries preserving the breast and cosmesis.This warrants adjuvant radiotherapy to the whole breast for majority of the breast cancer patients.Hypofractionated regimens come as a boon for the patients and radiation oncology staff.One week radiation course is truly beneficial for patients who appear for treatment from distant places.Patients prefer shorter treatment protocols due to financial and social reasons.Clinical evaluation also showed that the radiation treatment is well tolerated by patients than other regimes.Both acute and late effects are much lesser.Local control rates are not compromised.Hence we suggest that ultrahypofractionted radiotherapy by fast forward protocol is an excellent option for early breast cancer patients undergoing adjuvant radiotherapy.When the regional nodal irradiation substudy results are published ,we can treat locally advanced breast carcinoma too by the protocol in the future.
Conclusion
Ultrahypofractionated radiotherapy as an adjuvant treatment for early carcinoma of breast is well tolerated by the patients with minimal toxicity.Long term follow up is advised to evaluate the chronic implications of the treatment.
References
1. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024 May 4;
2. Kulothungan V, Ramamoorthy T, Sathishkumar K, Mohan R, Tomy N, Miller GJ, et al. Burden of female breast cancer in India: estimates of YLDs, YLLs, and DALYs at national and subnational levels based on the national cancer registry programme. Breast Cancer Res Treat. 2024;
3. Riedel F, Hoffmann AS, Moderow M, Heublein S, Deutsch TM, Golatta M, et al. Time trends of neoadjuvant chemotherapy for early breast cancer. Int J Cancer. 2020 Dec 1;147(11):3049–58.
4. Haviland JS, Owen JR, Dewar JA, Agrawal RK, Barrett J, Barrett-Lee PJ, et al. The UK Standardisation of Breast Radiotherapy (START) trials of radiotherapy hypofractionation for treatment of early breast cancer: 10-year follow-up results of two randomised controlled trials. Lancet Oncol. 2013 Oct;14(11):1086–94.
5. Murray Brunt A, Haviland JS, Wheatley DA, Sydenham MA, Alhasso A, Bloomfield DJ, et al. Hypofractionated breast radiotherapy for 1 week versus 3 weeks (FAST-Forward): 5-year efficacy and late normal tissue effects results from a multicentre, non-inferiority, randomised, phase 3 trial. The Lancet. 2020 May 23;395(10237):1613–26.
6. Offersen B V., Boersma LJ, Kirkove C, Hol S, Aznar MC, Biete Sola A, et al. ESTRO consensus guideline on target volume delineation for elective radiation therapy of early stage breast cancer. Radiotherapy and Oncology. 2015 Jan 1;114(1):3–10.
7. Kaidar-Person O, Vrou Offersen B, Hol S, Arenas M, Aristei C, Bourgier C, et al. ESTRO consensus guideline for target volume delineation in the setting of postmastectomy radiation therapy after implant-based immediate reconstruction for early stage breast cancer. Radiotherapy and Oncology. 2019 Aug 1;137:159–66.
8. Planning Pack for the FAST-Forward Trial A guide to outlining, planning & verifying FAST-Forward patients. 2013.
9. Radiotherapy Treatment Planning and Delivery SCOPE 1: Study of Chemoradiotherapy in Oesophageal Cancer Plus or Minus Erbitux A randomised phase II/III multi-centre clinical trial of definitive chemo-radiation, with or without Cetuximab, in carcinoma of the oesophagus RADIOTHERAPY GUIDANCE and PROCEDURES Version 3.0, 9 th. 2008.
10. Behroozian T, Milton LT, Shear NH, McKenzie E, Razvi Y, Karam I, et al. Radiation dermatitis assessment tools used in breast cancer: A systematic review of measurement properties. Vol. 29, Supportive Care in Cancer. Springer Science and Business Media Deutschland GmbH; 2021. p. 2265–78.
11. DeSantis C, Siegel R, Bandi P, Jemal A. Breast cancer statistics, 2011. CA Cancer J Clin. 2011 Nov;61(6):408–18.
12. Dhillon PK, Mathur P, Nandakumar A, Fitzmaurice C, Kumar GA, Mehrotra R, et al. The burden of cancers and their variations across the states of India: the Global Burden of Disease Study 1990–2016. Lancet Oncol. 2018 Oct 1;19(10):1289–306.
13. Overgaard M, Nielsen HM, Tramm T, Højris I, Grantzau TL, Alsner J, et al. Postmastectomy radiotherapy in high-risk breast cancer patients given adjuvant systemic therapy. A 30-year long-term report from the Danish breast cancer cooperative group DBCG 82bc trial. Radiotherapy and Oncology. 2022 May 1;170:4–13.
14. Whelan TJ. Use of conventional radiation therapy as part of breast-conserving treatment. Vol. 23, Journal of Clinical Oncology. 2005. p. 1718–25.
15. Fisher B, Bauer M, Margolese R, Poisson R, Pilch Y, Redmond C, Fisher E, Wolmark N, Deutsch M, Montague E, et al. Five-year results of a randomized clinical trial comparing total mastectomy and segmental mastectomy with or without radiation in the treatment of breast cancer. N Engl J Med. 1985 Mar 14;312(11):665-73. doi: 10.1056/NEJM198503143121101. PMID: 3883167.
16. Owen JR, Ashton A, Bliss JM, Homewood J, Harper C, Hanson J, et al. Articles Eff ect of radiotherapy fraction size on tumour control in patients with early-stage breast cancer after local tumour excision: long-term results of a randomised trial. 2006; Available from: http://oncology.thelancet.comVol
17. Articles The UK Standardisation of Breast Radiotherapy (START) Trial A of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial. Available from: http://oncology.thelancet.com
18. The UK Standardisation of Breast Radiotherapy (START) Trial B of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial. Available from: www.thelancet.com
19. Offersen B V, Alsner J, Nielsen HM, Jakobsen EH, Mette ;, Nielsen H, et al. Hypofractionated Versus Standard Fractionated Radiotherapy in Patients With Early Breast Cancer or Ductal Carcinoma In Situ in a Randomized Phase III Trial: The DBCG HYPO Trial. J Clin Oncol [Internet]. 2020;38:3615–25
20. Brunt AM, Haviland JS, Sydenham M, Agrawal RK, Algurafi H, Alhasso A, et al. Ten-year results of fast: A randomized controlled trial of 5-fraction whole-breast radiotherapy for early breast cancer. Journal of Clinical Oncology. 2020 Oct 1;38(28):3261–72.
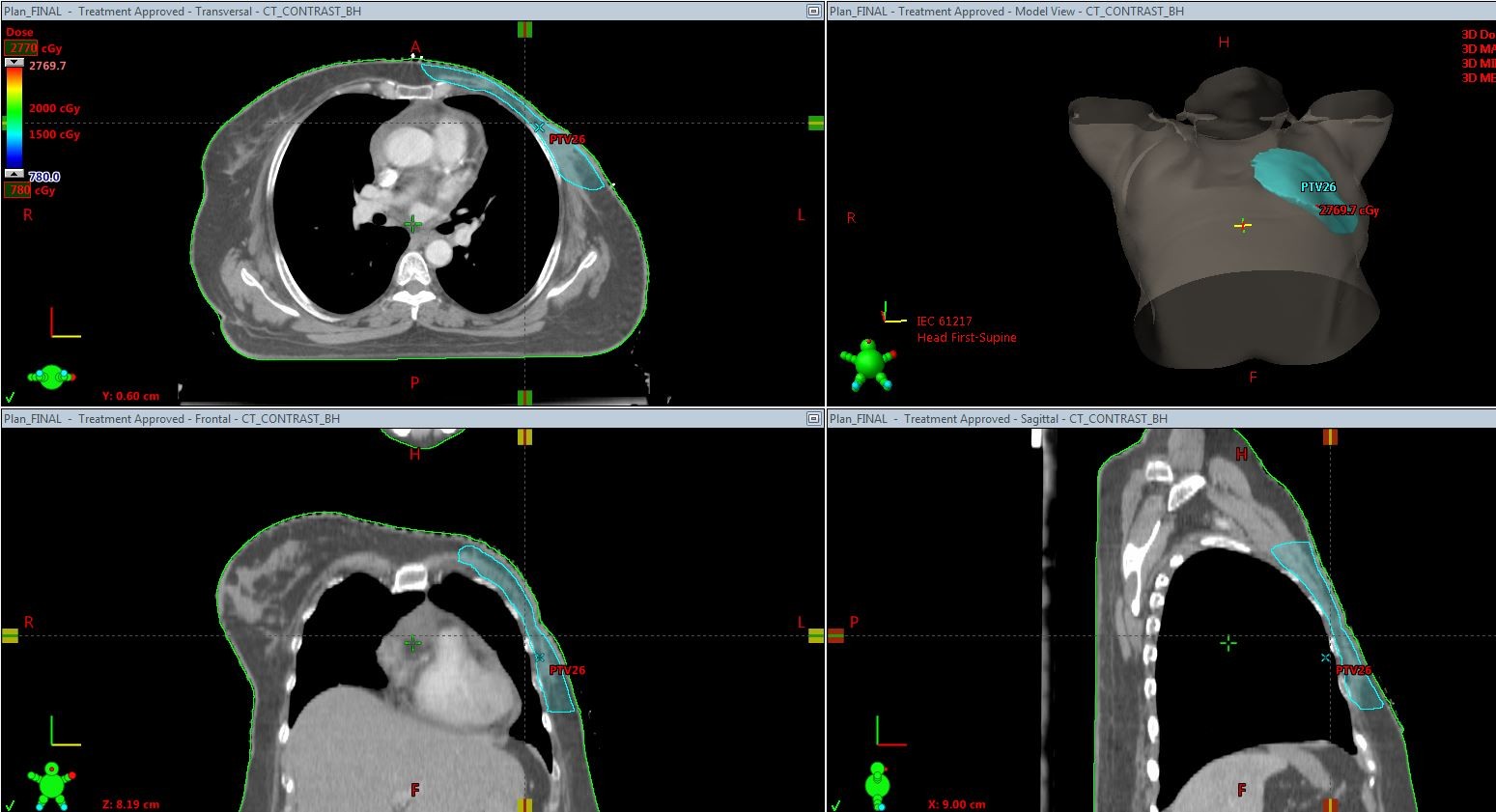
Figure 1
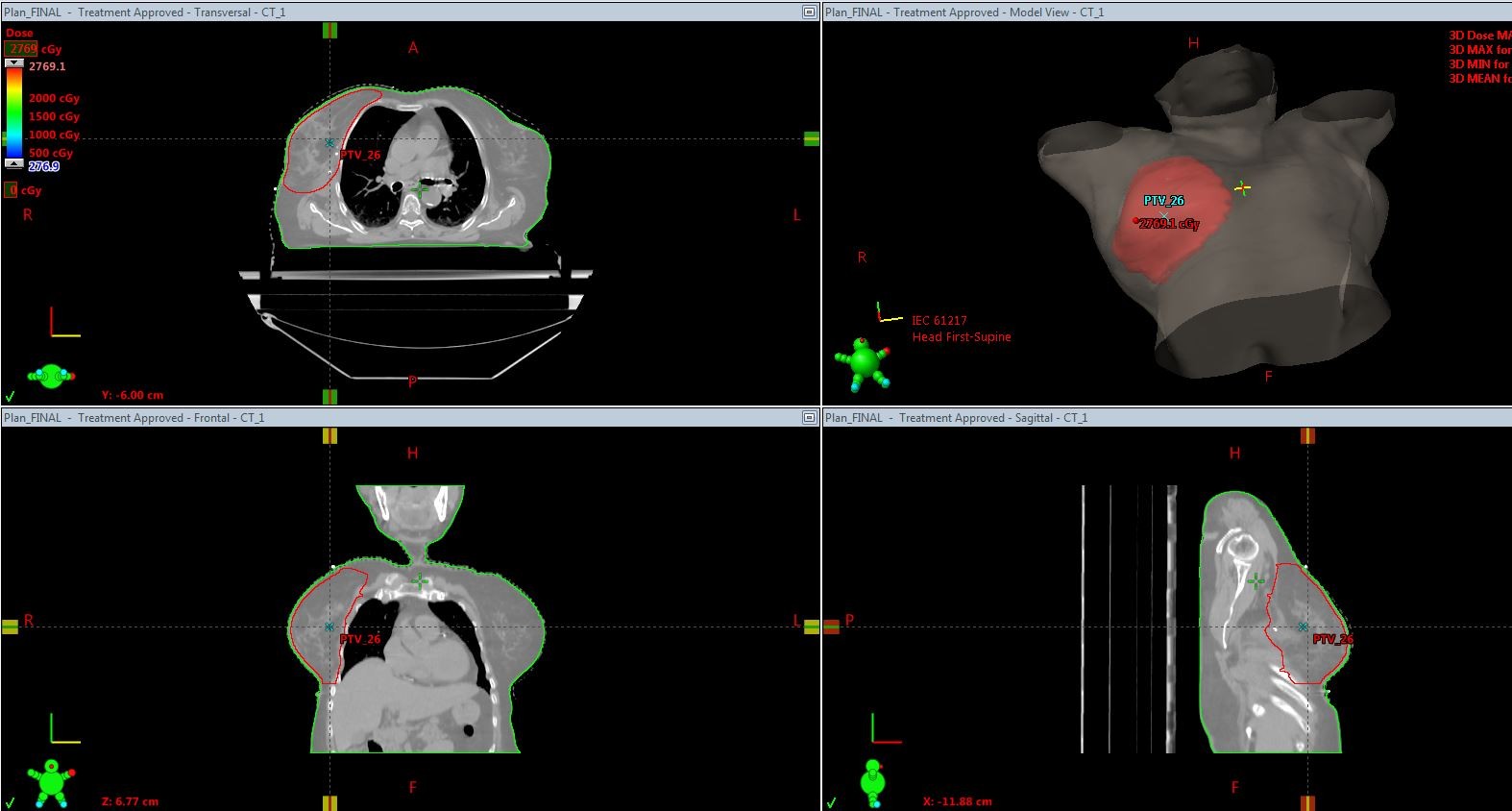
Figure 2
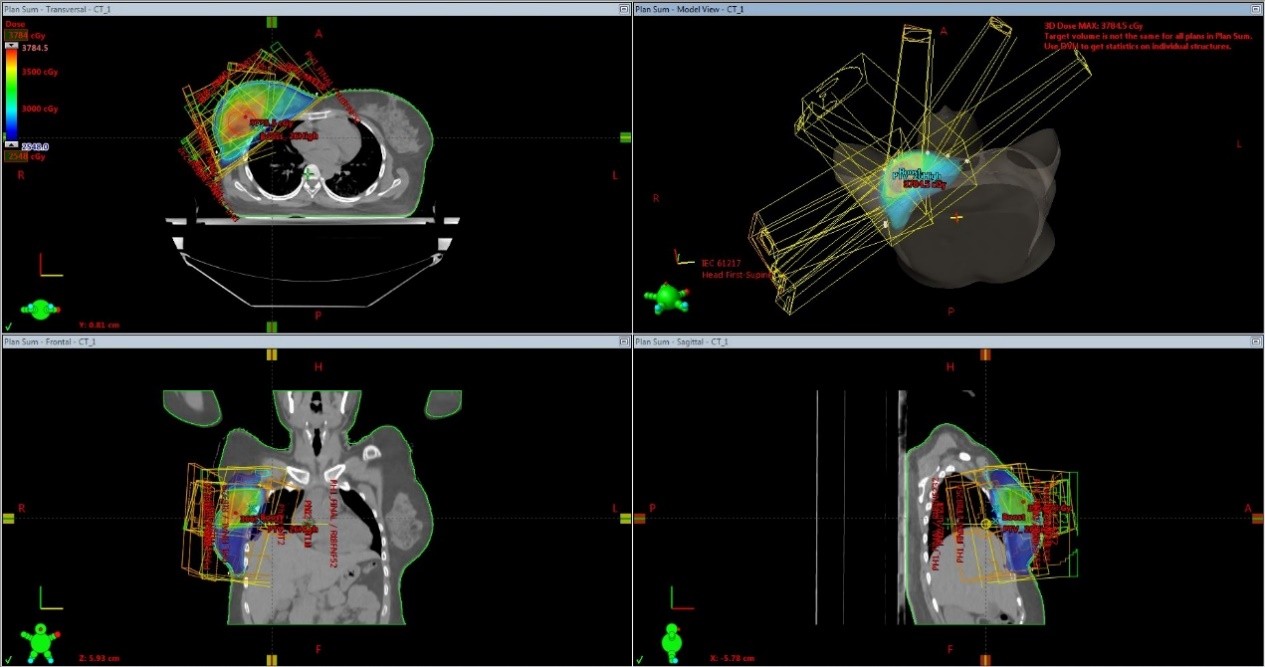
Figure 3
Figure 4
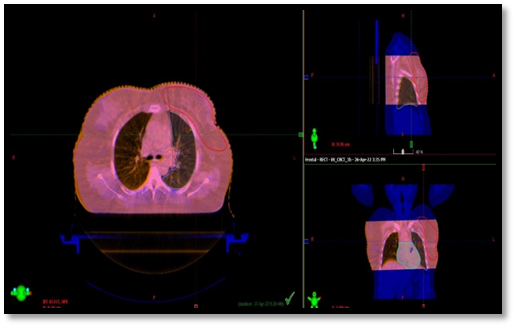
Figure 5