A Comparative Study on the efficacy and safety of discharge patient with Chest Tube attached to simple Drain Bag Versus Heimlich Valve.
A Comparative Study on the efficacy and safety of discharge patient with Chest Tube attached to simple Drain Bag Versus Heimlich Valve.
Dr. Muhammad Raza *, Dr. Ahmed Mohamed Abdelfattah1, Dr. Ali Raza Uraizee2, Dr. Syed Humayoon Sarwat3
- MS (Cardiothoracic Surgery), Specialist Thoracic Surgeon, Al-Noor Specialist Hospital, Makkah, Kingdom of Saudi Arabia. ORCID: 0009-0005-9732-788X
- Consultant Thoracic Surgeon, Al-Noor Specialist Hospital, Makkah, Kingdom of Saudi Arabia. ORCID: 0009-0002-3589-2275
- Consultant Thoracic Surgeon, Al-Noor Specialist Hospital, Makkah, Kingdom of Saudi Arabia. ORCID: 0009-0001-0006-2717
Correspondence to: Dr. Muhammad Raza MBBS, MRCS (Ireland), FCPS (Thoracic Surgery) Thoracic Surgery Specialist, Al-Noor Specialist Hospital, Makkah, Kingdom of Saudi Arabia. ORCID: 0000-0001-6413-8592
Copyright
© 2024 Dr. Muhammad Raza. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 June 2025
Published: 19 June 2025
Abstract
Background: Chest tubes are commonly used to manage pleural diseases such as pneumothorax, empyema, and malignant effusions. Early discharge of stable patients with chest tubes in situ has gained popularity, especially in resource-limited settings. Two primary ambulatory drainage methods are the Heimlich valve and the simple drain bag. However, the choice between them often depends on cost, availability, and patient compliance.
Objective: To evaluate the efficacy, safety, and practicality of discharging patients with a chest tube attached to a simple drain bag compared to a Heimlich valve.
Methods: A retrospective observational study was conducted on 32 patients discharged with a chest tube using either a drain bag (n=24) or a Heimlich valve (n=8). Patients were monitored for clinical improvement, complications, and ease of home care. Conditions included primary and secondary spontaneous pneumothorax, tuberculosis-related pneumothorax, pleural effusions due to malignancy, and lung infections.
Results: All patients showed clinical improvement on follow-up. No major complications, readmissions, or infections were reported in either group. Patients discharged with the drain bag reported better compliance and ease of use. The bag, equipped with a bottom valve for fluid drainage and a top vent hole for air release, proved to be a cost-effective alternative to the Heimlich valve.
Conclusion: The drain bag is a safe, inexpensive, and patient-compliant alternative to the Heimlich valve for ambulatory chest drainage, especially in under-resourced healthcare settings.
Keywords: Chest tube, drain bag, Heimlich valve, pneumothorax, ambulatory drainage, low-cost alternative, pleural effusion.
A Comparative Study on the efficacy and safety of discharge patient with Chest Tube attached to simple Drain Bag Versus Heimlich Valve.
Introduction
Chest tube thoracostomy is a vital intervention in the management of various thoracic conditions, including spontaneous pneumothorax, tuberculous pleural disease, empyema, and malignant pleural effusions. Traditionally, patients with chest tubes are retained in hospital until resolution of the underlying pathology. However, with the increasing burden on healthcare systems and a growing trend toward cost-effective care, early discharge of stable patients with chest tubes in situ has become increasingly adopted.
To facilitate outpatient management, various drainage systems have been developed to allow pleural decompression while preserving mobility and reducing infection risk. Among the most widely used devices is the Heimlich valve, a one-way flutter valve that prevents air reentry into the pleural space while allowing egress of air and fluid. Although effective, its cost and availability can be limiting factors, especially in underdeveloped or rural healthcare settings.
An alternative method involves the use of a simple drain bag. These gravity-based bags, when modified with a bottom valve for fluid control and a venting hole at the top to prevent the creation of a one-way air trap, can safely manage pleural drainage in ambulatory patients. The drain bag is not only cost-effective, but also readily available, making it a suitable. Other option is Digital Drain system, evolving now a days, but availability and cost is major issue.
Despite anecdotal reports and sporadic clinical use, there is a lack of systematic data comparing the drain bag to the Heimlich valve in terms of safety, efficacy, and patient satisfaction. In this study, we present our experience from a thoracic unit managing a diverse set of pleural diseases, comparing outcomes between patients discharged with either a modified drain bag or a Heimlich valve.
The goal of this study is to provide clinical insights into the practical advantages of using the drain bag — especially in regions where medical resources are constrained — and to offer evidence supporting its adoption as a standard ambulatory drainage method.
Materials and Methods
Study Design and Setting
This was a retrospective observational study conducted at a tertiary care thoracic surgery center between November 2023 and March 2025. The aim was to compare the efficacy, safety, and patient compliance of two ambulatory drainage systems — a simple drain bag and a Heimlich valve — in patients discharged with indwelling chest tubes.
Patient Selection
A total of 32 patients who underwent chest tube insertion and were subsequently discharged home with either a simple drain bag (n=24) or a Heimlich valve (n=8) were included. These patients had conditions such as tuberculosis-related pneumothorax, primary and secondary spontaneous pneumothorax, malignant pleural effusion, lung abscess, and other pleural diseases requiring prolonged drainage.
Inclusion Criteria
• Adults aged ≥18 years
• Hemodynamically stable at discharge
• Presence of a chest tube with controlled or resolving air leak or fluid drainage
• Willingness and ability to manage drainage at home
• Documented follow-up available Post- discharge Stable patients with mild / resolving air leak for those who refused surgery and planning for air travel back in home country after Pilgrimage activity (Hajj / Umrah)
• Chronic pleural disease with residual dead space / non expansion of lung
Exclusion Criteria
• Patients requiring mechanical ventilation or ICU care
• Massive or uncontrolled air leak
• Coagulopathy or uncontrolled systemic infection
• Non-compliance or inability to manage device at home
• Hemodynamically Unstable with sepsis
Interventions
Patients were grouped based on the drainage system used at discharge:
• Group A (Drain Bag, n=24): A gravity-dependent sterile collection bag with a one-way fluid valve at the base. A small air vent hole was added at the top of the bag to allow pressure equilibration and prevent one-way valve-like behavior.
• Group B (Heimlich Valve, n=8): A standard one-way flutter valve allowing air to escape from the pleural space while preventing reentry.
Both interventions were connected to the standard thoracic chest tube (28–32 Fr) and secured appropriately. Instructions on home care, fluid disposal, and signs of complications were given to all patients and caretakers. Follow-up occurred at 7 days or earlier if complications arose.
Outcomes Measured
• Primary Outcomes:
- The primary aim of this study was to assess the safety, feasibility, and short-term compliance of discharging patients with a chest tube using a simple drain bag versus a Heimlich valve.
- Long-term outcomes such as complete resolution of pneumothorax or definitive tube removal were not the primary endpoints, as many patients were lost to follow-up due to travel for personal or religious reasons, and several cases required subsequent surgical management.
• Secondary Outcomes:
o This study was to evaluate the practical usability and patient experience of two ambulatory chest drainage systems — a simple drain bag and a Heimlich valve — in patients discharged with indwelling chest tubes.
o Key Outcomes Assessed
o Handling and Compliance
o Ease of device management by patients or caretakers
o Willingness to follow drainage instructions
o Adherence to advice during the discharge period
o Tolerance and Comfort
o Patient-reported experience of carrying the device
o Physical discomfort, mobility limitations, or social inconvenience
o Familiarity and Acceptability
o Whether patients or their families were more familiar with the device (e.g., IV-style drain bags vs. flutter valve)
o Influence of visual design or cultural factors on device preference
o Complications
o Any early adverse events such as infection, tube blockage, dislodgment, or leakage during the ambulatory period
Data Collection and Analysis
Demographic and clinical data including age, diagnosis, intervention type, and discharge condition were extracted from patient records. Descriptive statistics were used to summarize findings. Continuous variables were reported as means ± standard deviations, while categorical variables were presented as counts and percentages. Due to the small sample size, statistical significance testing was not performed, but comparative descriptive analyses were conducted to assess trends between groups.
Figure 1
Figure 2
Drain bag is safe alternative to Heimlich valve when used alone, it contains valve at base where tube meets collection area
Results
A total of 32 patients were included in this observational study. Patients were divided into two groups based on the intervention device used during discharge: simple drain bag (n=24) and Heimlich valve (n=8). All patients were adults with various underlying causes of pneumothorax or pleural disease, including tuberculosis-associated pneumothorax, spontaneous pneumothorax, infectious causes, and malignant effusions.
Table 1: Distribution of Interventions
|
Intervention Type |
Number of Patients |
|
Drain Bag |
24 |
|
Heimlich Valve |
8 |
Observation: Drain bags were used in 75% of the patients, highlighting their wider availability and cost-effectiveness, especially in resource-limited settings.
Table 2: Patient Age Statistics by Intervention
|
Intervention |
Total Patients |
Mean Age |
Min Age |
Max Age |
|
Drain Bag |
24 |
39.9 |
26 |
74 |
|
Heimlich Valve |
8 |
29.4 |
21 |
54 |
Observation: The Heimlich valve was more commonly used in younger patients, while the drain bag was favored in older or more comorbid individuals.
Table 3: Condition on Discharge by Intervention
|
Intervention |
Improved |
|
Drain Bag |
24 |
|
Heimlich Valve |
8 |
Observation: All patients in both groups were clinically stable and discharged in an improved condition. No deterioration was observed during the short-term follow-up.
Table 4: Disease Distribution by Intervention Type
|
Disease |
Drain Bag |
Heimlich Valve |
|
Tuberculosis persistent pneumothorax |
2 |
1 |
|
Tuberculous effusion |
2 |
0 |
|
Secondary Spontaneous Pneumothorax |
2 |
1 |
|
Primary Spontaneous Pneumothorax (reluctant for surgery) |
1 |
2 |
|
Recurrent Primary Spontaneous Pneumothorax |
2 |
2 |
|
Malignant Pleural Effusion (Lung Carcinoma) |
4 |
0 |
|
Multiple systemic comorbidities (e.g., CKD, CLD, HF) with pleural effusion |
2 |
0 |
|
Pneumonia leading to secondary spontaneous pneumothorax |
3 |
0 |
|
Bullous lung disease with pneumothorax |
2 |
0 |
|
Ruptured lung abscess |
2 |
0 |
|
Persistent air leak |
1 |
1 |
|
Pneumothorax with bilateral bronchiectasis |
1 |
1 |
Observation:
• The drain bag group predominantly included patients with infectious, malignant, or comorbid causes of pneumothorax or effusion.
• The Heimlich valve group was used primarily for younger patients with primary or recurrent spontaneous pneumothorax, often reluctant to undergo surgery.
• Most of the patients discharge with ambulatory devices either bag or valve were those who were having spontaneous pneumothorax or mild air leak and were unwilling for surgery, on follow up air leak resolved, allowing for safe removal of chest tube. However, some patients required surgical intervention.
• Patients with tuberculosis either effusion or pneumothorax once clinical stable and cleared by infectious disease were safely discharged with bag and shows improvement on follow-up.
• Patients having multiple co-morbidities (e.g., chronic liver disease, chronic kidney disease and heart failure) who were not surgical candidate were discharged on bag and follow-up shows improvement.
• Patients with pneumothorax or pleural effusion due to malignancy or tuberculosis discharge with ambulatory devices (either bag or valve) were able to perform religious pilgrimages (Hajj / Umrah) safely and traveleed internationally back to home country safely.
• No major complications were noted in either group during discharge or follow-up.
• Drain bag group showed good compliance and tolerated home care well.
• In cases where Heimlich valve was not available or was cost-prohibitive, the drain bag served as a reliable, inexpensive alternative.
Figure 3
Figure 4
Figure 5
Figure 6
Figure 7
Discussion
This study demonstrates that both the simple drain bag and the Heimlich valve are safe and viable options for ambulatory chest tube management in selected patients. Among the 32 patients studied, all showed clinical improvement at discharge, and no significant device-related complications or readmissions were recorded during short-term follow-up.
The drain bag group (n=24) demonstrated particularly favorable outcomes in terms of compliance, handling, and comfort. Modifications such as a top venting hole and bottom valve allowed safe and controlled drainage. Its design familiarity also contributed to better acceptance among patients and caregivers with minimal clinical background.
While the Heimlich valve (n=8) is an effective one-way valve system, its use was more frequent in young patients with spontaneous pneumothorax, some of whom declined surgical treatment. However, its higher cost and limited availability in certain settings can restrict use.
This study reflects a unique patient population, many of whom were pilgrims or international travelers requiring early discharge and air travel clearance. For these patients, the modified drain bag allowed for safe temporary management of their condition before continuing definitive care in their home countries.
It’s important to clarify that this study did not aim to assess long-term outcomes, such as pneumothorax resolution or recurrence. Many patients were discharged as part of a planned staged treatment, with surgery or tube removal arranged later.
Additionally, no complications such as infection, tube blockage, or dislodgement were noted in either group. All patients were either followed until tube removal or referred for definitive surgery once lung re-expansion was confirmed.
While encouraging, these results should be interpreted with the understanding that this was a non-randomized, single-center study with a modest sample size. Larger, prospective, and randomized trials would help validate these findings across diverse patient populations and healthcare environments.
Conclusion
In this comparative study of 32 patients, we found that the modified drain bag offers a safe, cost-effective, and patient-compliant alternative to the Heimlich valve for ambulatory chest drainage.
Though conducted in a well-equipped tertiary center, the findings also support the bag’s utility in resource-limited environments, based on the authors' prior experiences in such settings. The drain bag performed particularly well in cases where early discharge and air travel were necessary, and where patients required a familiar and easy-to-use system.
With proper training and follow-up, the drain bag can reduce hospital stays and support continuity of care across diverse health systems. It is a practical and flexible solution that deserves broader consideration in clinical practice — both in advanced care hospitals and in settings with limited access to commercial drainage valves.
References
1. Bauman JW, et al. Ambulatory management of pneumothorax with a one-way valve device. Chest. 1995;107(2):699–703. doi:10.1378/chest.107.2.699
2. Chan SS, et al. Outpatient chest tube management of spontaneous pneumothorax using a Heimlich valve: a safe and cost-effective option. Emergency Medicine Journal. 2002;19(2):164–167. doi:10.1136/emj.19.2.164
3. Gibson GJ, et al. Management of pleural disease: a review. BMJ. 2008;336(7652):1222–1226. doi:10.1136/bmj.39542.617572.BE
4. Tokuda Y, et al. Use of portable chest tube drainage with Heimlich valve in treating pneumothorax in resource-limited settings. Rural and Remote Health. 2009;9(3):1191.
5. Light RW. Pleural Diseases. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2013
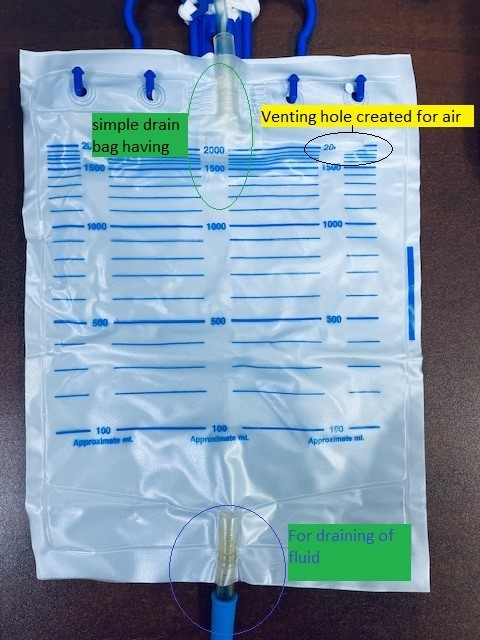
Figure 1
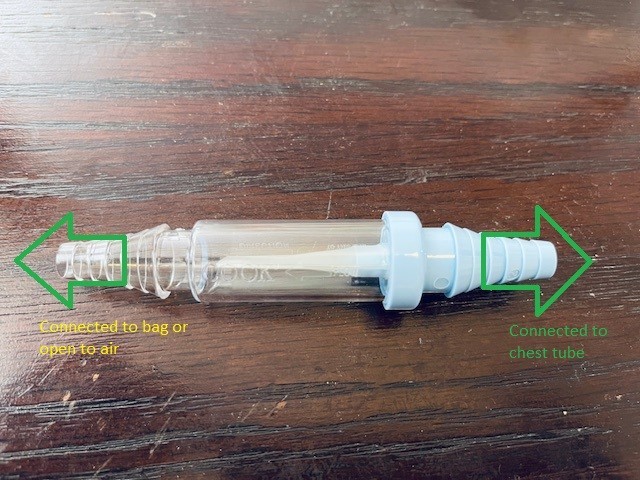
Figure 2
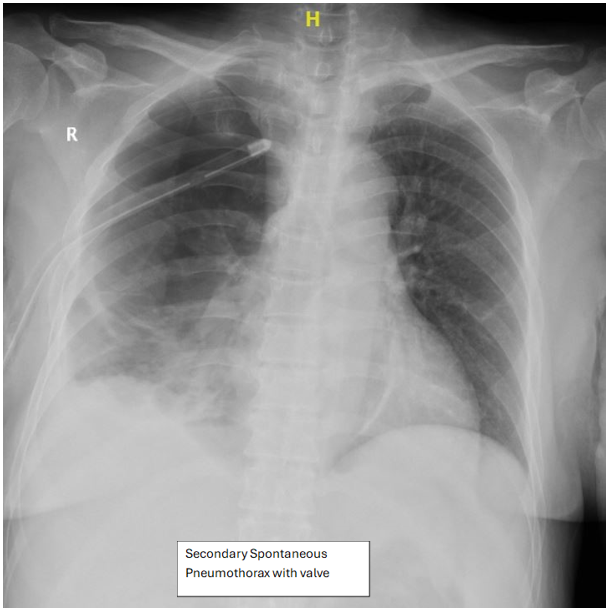
Figure 3
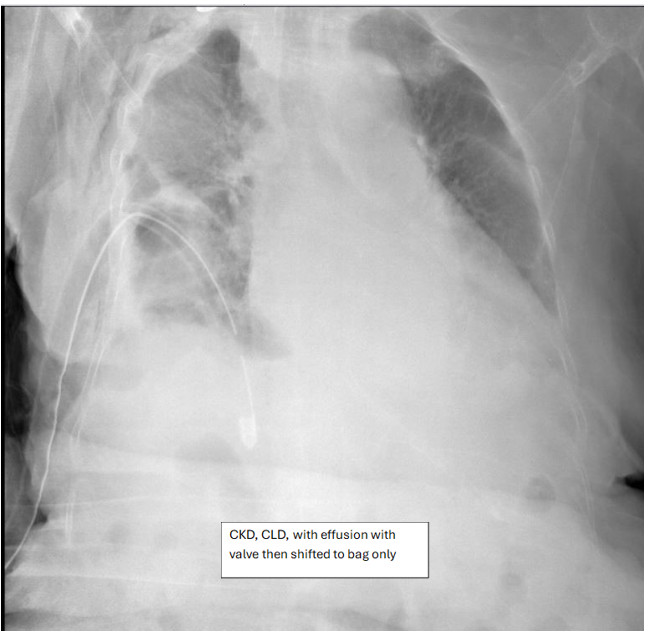
Figure 4
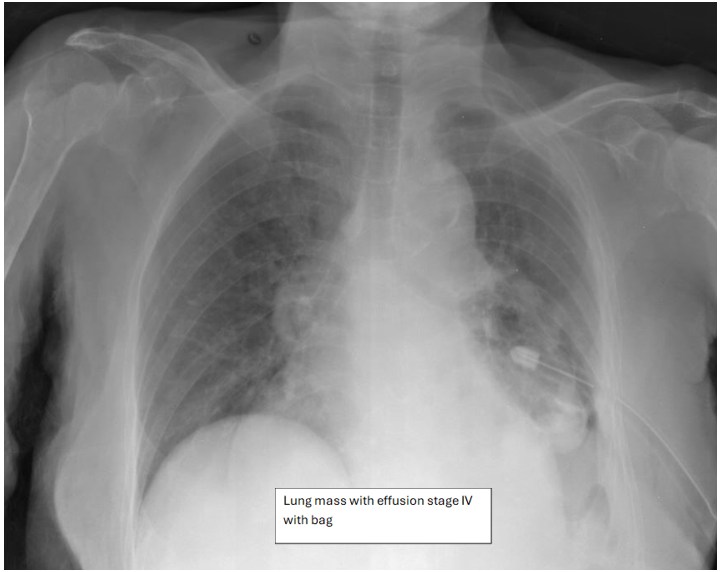
Figure 5
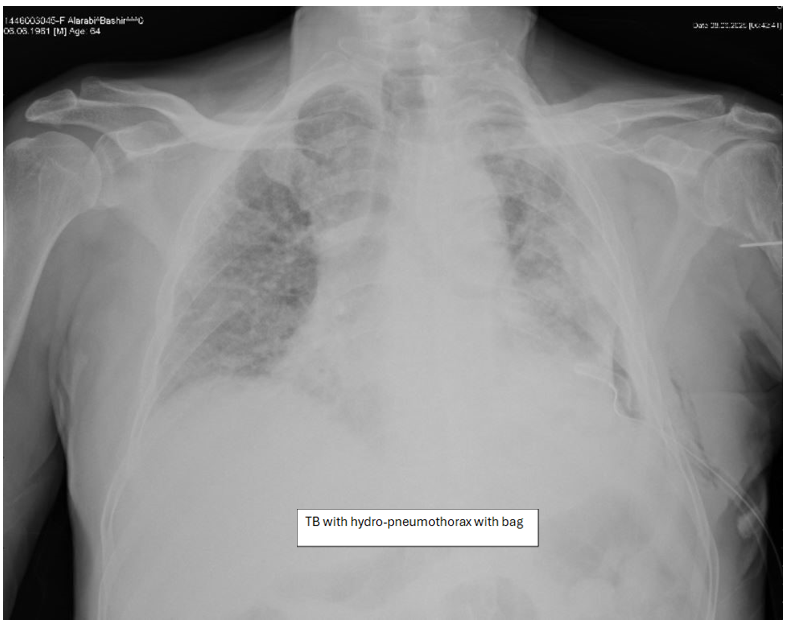
Figure 6
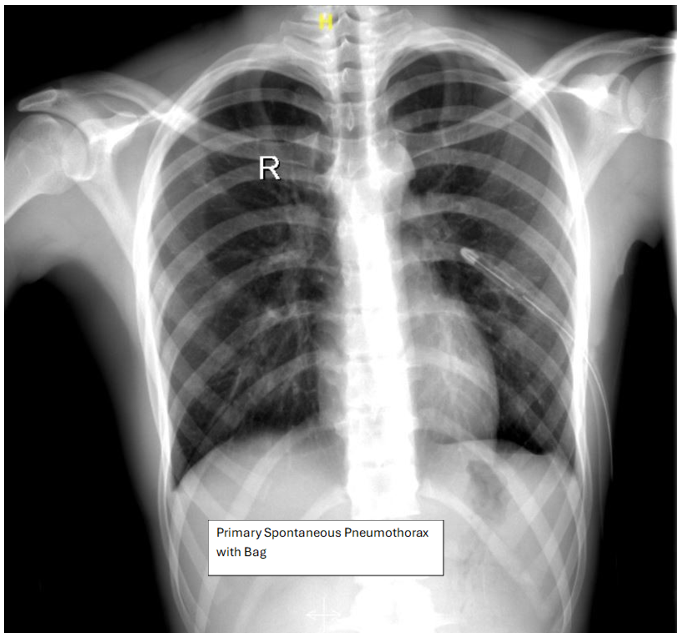
Figure 7