Manuel Ascunce Domenech University Hospital, Camagüey. Elements necessary to Prevent Bile Duct Injury during Cholecystectomy.
Manuel Ascunce Domenech University Hospital, Camagüey.
Elements necessary to Prevent Bile Duct Injury during Cholecystectomy.
Dr. Héctor Alejandro Céspedes Rodríguez*
*Correspondence to: Dr. Héctor Alejandro Céspedes Rodríguez. , General Surgery Specialist, 1st Degree. Instructor. ORCID iD: https://orcid.org/0000-0002-3668-9888
Copyright
© 2025 Dr. Héctor Alejandro Céspedes Rodríguez. . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 June 2025
Published: 19 June 2025
DOI: https://doi.org/10.5281/zenodo.15797731
Abstract
Introduction: Cholecystectomy is the most performed surgery, with bile duct injury being the most feared complication. Objective: To characterize the essential elements in the prevention of bile duct injuries during cholecystectomy according to the access used. Methods: A bibliographic review was conducted in PubMed/Medline using the keywords: Bile duct injury, safe cholecystectomy, prevention of bile duct injury, published between 2010 and 2024. Studies with more than 40 studies, comparative or not, in English, Spanish, and Portuguese were included. The variables studied were: tristructure method, Fisher method, infundibular technique, visualization of Rouviere's sulcus, Lord Ganesha sign, use of intraoperative cholangiography and ultrasound, use of indocyanine green, and changes in strategies. Results: No randomized trials were found. In addition, a group of studies were included that compare Rouviere's sulcus, Lord Ganesha's sign, Strasberg's critical vision, infundibular technique, tristructure identification, Budde and Calot triangle and others that compare the results between different studies where there was a change in strategy, as well as studies where cholangiography, ultrasound and intraoperative indocyanine green were used. Most studies are retrospective. Conclusions: Despite the existence of all the elements previously described, biliary tract injuries are still significant among surgical services. Where the identification and visualization of these methods, strategies and tools as a group can prevent biliary tract injuries.
Keywords: Biliary tract injury, prevention, safe cholecystectomy.
Manuel Ascunce Domenech University Hospital, Camagüey. Elements necessary to Prevent Bile Duct Injury during Cholecystectomy.
Introduction
Cholecystectomy is one of the most frequently performed surgeries: more than 60,000 surgeries are performed annually in Japan and 750,000 in the United States.(1,2) Bile duct injury is the most unfortunate complication of cholecystectomy. cholecystectomy. The morbidity rate is 0.4 to 0.6% for laparoscopic surgery, which is 2 to 3 times higher than that for open surgery (1,2,3,4).
Furthermore, LIVB is associated with significant morbidity and mortality and requires a complex and expensive procedure (1,2,4), with an increase in surgical costs of more than 100% compared to laparoscopic cholecystectomy and an increase in morbidity of 8.8% compared with uncomplicated surgery. Bile duct injury can occur for many reasons, the most common of which is iatrogenic bile duct injury. These are complex clinical situations that occur in apparently healthy patients and are associated with significant morbidity and low, but not insignificant, mortality. (1.4)
The number of biliary tract injuries (BLI) has not decreased despite completion of training, acquisition of more skills and experience, and improvements in the optics of endoscopic equipment. Injuries have been reported even among experienced surgeons who have performed more than 200 laparoscopic procedures and have more than 30 years of experience. It should be noted that approximately 2,000 new cases are reported each year in the United States alone. (2,3) Data on the true incidence of biliary tract injuries are difficult to collect due to surgical negligence and are sometimes intentionally hidden from medical records and documented as anatomical abnormalities.
On the other hand, this serious complication is mainly treated in other centers specialized in this type of surgery. Because surgeons are reluctant to report their complications and are treated in tertiary centers, the true extent of the problem remains uncertain. Based on the above, we pose the following question. What are the key factors that prevent bile duct damage during cholecystectomy?
Method
A bibliographic review was carried out based on the consultation of scientific articles related to the topic (2010-2023). The information sources consulted were Pubmed, Ebsco and SciELO. The full text version was obtained through open access in Pubmed, HINARI and through open access. The information was analyzed and selected in accordance with the theme and declared objectives and was processed using computerized means.
Development
Strategies to prevent bile duct injury during cholecystectomy include the use of work tools, the application of dissection techniques or methods, and changing strategies to prevent this dangerous complication.
Among the methods used we highlight:
Tristructure method and identification of the Budde and Calot triangle: we must identify during LC: Cystic Duct (CC), common hepatic duct and common bile duct. Jean François Calot (1861-1944), French surgeon, his doctoral thesis was called “De la colecystectomy” and was completed in 1890; In it it describes an isosceles triangle given by the cystic artery and duct at its upper and lower limits respectively, and by the hepatic duct medially. International anatomical terminology contemplates the existence of this triangle under the term “cystohepatic trigone”. Calot insisted that "the surgeon must work by sight and not by faith." In 1906, Budde described an anatomical triangle between the CC, the hepatic duct and the liver, and called it the "bile duct triangle." It can be divided into triangle described by Budde (Figure 1) in two sectors, one medial (Critical Triangle) and another lateral (Safety Triangle), its separation limit being a line that goes from the hepatocystic angle, passing through the birth of the cystic artery and reaching the hepatic margin. The identification of the CT constitutes a universal method for safe cholecystectomy for both routes during a cholecystectomy present in the guidelines and score for the safety of this procedure. represented by the “cystic lymph node” or Mascagni node, which is always found lateral to the biliary tree and should form the medial end point of dissection.(3,6,7) Algieri et al.(5) agrees with the above. and they constitute principles of dissection during a cholecystectomy the Cuban school of surgery mentions in its work standards.
Figure1: Budde's triangle and its medial part that constitutes Calot's triangle are observed.
Fischer method (cholecystectomy from bottom to neck): consists of completely separating the gallbladder from the gallbladder bed from the bottom to the infundibulum as in open surgery, hanging from the artery and the CC. This is especially difficult in the case of intrahepatic or highly inflamed vesicles. Separation of the gallbladder from the liver bed also tends to bleed more because it was not previously connected to the cystic artery. This is the basic principle of open cholecystectomy and belongs to the Tokyo guidelines for safe cholecystectomy, but it belongs to Álvarez et al. Arsenal of laparoscopic techniques. (9) In their study on complicated laparoscopic cholecystectomy, their management mentioned performing subtotal cholecystectomy because the incidence of VBL increases when the procedure is performed laparoscopically, but it is not common during laparoscopic cholecystectomy, it is not mentioned in step 6. LC safe in the 2018 Tokyo guidelines by Wakabayashi et al (2) and is not within the 10 steps of the Kankaria score. In a study of 1226 patients undergoing laparoscopic cholecystectomy, Manatakis et al (11) performed the procedure in only 12 patients and ended with cholecystectomy due to insufficient visualization of Strasberg critical visual acuity (CSV).
Infundibular technique: involves dissection and release of Calot's triangle until the artery and cystic duct are exposed and the base of the liver is exposed (Figure 2). Once this view is achieved, these structures can only correspond to the duct and the cystic artery (fig. 3). In cases of aberrant ducts or in cases of highly inflamed vesicles, the exposure of the inner layer of the subserosa, optimizing the critical view. Strasberg et al.(14) report that 80% of VBLs are produced by the premature and early interruption of the CC without the identification and preparation of the anatomical structures having been completed.
Figure 2: Strasberg's critical vision or security is observed.
Figure 3
Over the years, several methods to prevent iatrogenic bile duct injury have been proposed and described in the scientific literature. The critical safety view (CVA) technique was introduced by Strasberg in 1995 and is considered the gold standard for performing a safe cholecystectomy with identification of biliary structures during dissection. Three criteria are required to achieve CVS:
1) The hepatocystic triangle must be cleaned of adipose tissue and fibrotic tissues; CBD and CHD should not be exposed; 2) the lower third of the gallbladder must be separated from the liver bed to expose the cystic plate; and 3) two and only two structures should be seen entering the gallbladder. CVS was conceived not as a way to do LC but as a way to avoid biliary injury. In 2013, Sanford and Strasberg et al.(15) began photographic documentation of the SVC with the aim of increasing safety in laparoscopic cholecystectomy. This photo documentation is for the purpose of qualifying the anterior and posterior vision of the SVC using an established score, using the term "doublet view." Obtaining a satisfactory SVC is also part of other safe cholecystectomy programs, such as the one implemented by the Society of American Gastrointestinal and Endoscopic Surgeons.(16) In 2017, Strasberg et al.(14) stated that they had detected that, after 20 years, many surgeons have little understanding of the criteria required to achieve SVC, especially those who did not have training in implementing SVC in laparoscopic cholecystectomy during their residency, so they opt for simpler methods, such as the infundibular technique, which represents a greater risk of bile duct injury. Another obstacle mentioned is that when VCS is carried out, photographic documentation with the qualification of “paired vision” is generally not carried out. Current evidence shows that with the implementation of VCS the probability of LIVB is 0 to 0.03% and in a Japanese review 0.77% of LVB has been decreased to 0.58 with its implementation. Current data show that the probability of LIVB ranges from 0 to 0.03% after VCS implementation, and in the Japanese study, 0.77% LVB decreased to 0.58 after implementation. A recent work by the Turkish Society of Hepatopancreatic Surgery using the Delphi method attempts to reach a consensus on biliary tract injury. They agreed that it was necessary to develop a critical vision of security; If this cannot be achieved, laparoscopic cholecystectomy should not be performed, but partial cholecystectomy or conversion to open surgery may be performed. Therefore, the lack of identification of the SVC alerts the surgeon and systematically performs the following actions:
1) Intraoperative pause and call a colleague. 2) Use of cholangiography or intraoperative indocyanine green. 3) Conversionorchange of technique.
Visualization of the Sign of Lord Ganesha: This sign, also called the trunk or elephant head (Figure 3), is another measure to prevent this feared complication and this sign is part of the union of the infundibular technique and Strasberg's critical view. . Ashok et al.(17) in their study created a scoring system for safe cholecystectomy where the visualization of the sign of Lord Ganesha is part of it, granting 1 point when it is present, it constitutes one more tool in the arsenal for the prevention of injuries. of the bile duct. Tantia et al.(18) mention the visualization of the elephant trunk as an element to always take into account during a cholecystectomy and its non-visualization is associated with inability to adequately dissect Calot's triangle. Although this sign only contributes one point in this score, its non-visualization indicates an inadequate infundibular technique and critical safety vision, and may be associated with the possibility of an injury to the pathway without a change to an appropriate strategy. (19,20,21)
Figure 4: Rouviere's groove is observed, the green area shows the safe dissection plane.
Visualization of Rouviere's sulcus: Different anatomical landmarks for cholecystectomy have been described: among them, in 1924, Henri Rouvière, French surgeon, this sulcus measures 2 to 5 cm long and is present on the lower surface of the right lobe of the liver, running to the right of the hepatic hilum (Fig. 4). It is easily visible in the majority (80%) of cases in which it remains open (partially or completely), and usually contains the right portal pedicle and identifies the sagittal plane of the main bile duct. During LC, it is best seen when the neck of the gallbladder retracts into the umbilical fissure. The dissection can safely begin in a triangle anterior and superior to the plane of the sulcus. It is essential that the surgeon knows the safe dissection zone to delineate the cystic duct and cystic artery. Looking at the fixed anatomical landmark (B-SAFE) will help the surgeon identify and remain in the safe dissection zone. These fixed anatomical landmarks include the bile duct and base of segment 4 (B), Rouviere's groove and segment 4 (S), hepatic artery (A), umbilical fissure (F), and enteric viscera (E), p. duodenum, pylorus. The Rouviere sulcus can now be defined in three simple terms: a deep sulcus, a cleft, or a scar. It is recommended by Basukala et al.(22), Singh et al.(23), Cheruiyot et al.(24) and Al-Naser et al.(25) as the first step in laparoscopic cholecystectomy, the surgeon must look for this point reference (whether in the form of a scar, a cleft or an actual groove) that will be the plane of the main bile duct, and therefore avoid any dissection below this point to eliminate any danger to the bile duct during the surgery.(26,27)
Although the groove of Rouviere is increasingly mentioned as the first landmark to begin dissection during laparoscopic cholecystectomy to prevent bile duct injuries, the anatomy of the groove has not been described in clear and simple terms. With an increasing emphasis on patient safety in recent years, it is recommended to identify and follow some landmarks that can guide surgeons from where to start the dissection by identifying the common bile duct (CBD) plane even earlier. before the dissection begins. A common landmark or landmark that is increasingly described in recent reports is the Rouviere groove. This sulcus, which was barely seen and described in the era of open surgery, is seen very clearly during LC. Today the SR is an element present in the guidelines proposed by Wakabayashi et al.(2), Gupta et al.(8) and Barauskas et al.(19) in favor of a safe cholecystectomy, this dissection plane should never be violated which promotes adequate visualization of the SVC, thus achieving a safe procedure.
Intraoperative cholangiography (IOC): since the Argentine Pablo Mirizzi introduced the first intraoperative cholangiography in 1932 until today, its benefit in preventing LIVB is debated.(3,10,11) IOC can help avoid LIVB at least for 3 causes: 1. Shows the diversity of the biliary tree and its abnormalities. 2. Helps the surgeon identify patients at risk for LIVB due to abnormal anatomy. 3. If LIVB has occurred, it allows for its identification and repair.
IOC has been shown to be cost-effective, especially when used by less experienced surgeons and when risk factors are present. Other studies do not recognize IOC as preventing LIVB and emphasize an increase in overall operative time. Many studies have been conducted on the use of IOC in the prevention and detection of biliary tract injuries. Regular use for LIVB prevention has been widely recommended, but remains controversial to this day. (28) COI has several disadvantages: longer surgical time, need for x-rays in the operating room, radiation exposure of the patient and specialist, and increased risk of biliary injury due to the placement of the transcystic cannula. Because it is related to type D injuries according to the Strasberg-Bismuth (CSB) classification.
In relation to cholangiography, although Flum et al.(29) have demonstrated a lower frequency of injuries in the patients in whom it was performed, the following circumstances must be kept in mind: a) Injuries may occur in attempts at cholangiography. b) The surgeon must be expert in interpreting the possible variations of the biliary tree. c) On some occasions, cholangiography does not prevent the lesion, but rather makes the lesion manifest. d) Even if the structures are identified in the radiological study and no injury is demonstrated, it may occur later. However, many other retrospective studies specific to laparoscopic cholecystectomy have not identified a benefit from the routine use of IOC. The largest work includes 111,815 patients with no differences in bile duct injury between routine use (0.25%) versus selective use (0.26%) and a slight increase in overall complications with routine use (7, 3% vs. 6.7%). In a survey of surgeons from the American College of Surgeons, only 27% routinely used IOC. In the survey carried out among Turkish surgeons, the routine use of IOC is not considered indicated, but they do consider that it should be used when the anatomy is uncertain, when a laparoscopic exploration of the bile duct is planned, or when we suspect intraoperative injury. It has proven useful in early intraoperative diagnosis once bile duct injury has occurred. In the Japanese study, only 20% of the surgeons questioned agreed with performing systematic IOC to prevent bile duct injury. In our country it is a routine procedure during open cholecystectomy, but this is not the case in laparoscopic cholecystectomy. And there are no significant reports of type D injuries according to CSB due to this procedure.
To date, there are no randomized clinical trials that justify the use of IOC. Its role has been focusing fundamentally on the intraoperative diagnosis of LIVB according to Manterola et al.(3).
Intraoperative laparoscopic ultrasound (IOC): in recent multicenter studies, its advantages for the prevention of LIVB are highlighted, although it is another very expensive method and sometimes not available in all hospitals, which does not completely replace IOC but opens up a future encouraging. Most authors(10,11,20,38) conclude that intraoperative ultrasound allows safe and clear visualization of the biliary anatomy and reduces the probability of BLI. Obviously this greatly increases the costs of surgery and cannot be used systematically. Its use is reported in 2.1% of surgeons dedicated to biliary surgery.
Figure 5 :The use of indocyanine green is observed during the dissection.
Use of indocyanine green (VI): Indocyanine green (VI) (Fig. 5) is a tricarbocyanine pigment that is administered intravenously and quickly and completely binds to albumin and is taken up by hepatocytes and eliminated for the bile. It has been approved by the FDA and among them for fluorescence-guided surgery (F). The first to use it to identify the bile duct was Ishizawa, as reported by Pérez et al.(32). There are experimental works that demonstrate that indocyanine green reaches a peak of F in the bile 8 minutes after its administration and this F is due to the fact that it binds to proteins present in the bile. It can be observed in the bile duct as early as 15 minutes after administration and F in the bile duct can persist more than 7 hours after administration. One of the problems is the penetration of light, which is not greater than 10 mm, so it can be difficult to identify structures with this technique in situations of inflammation. Identification of biliary anatomy is one of the most established applications for one simple reason: indocyanine green has an exclusively hepatic metabolism and excretion begins within 30 minutes after injection. We will comment on its use in LIVB, recently a series of possible advantages of the use of fluorescence cholangiography with indocyanine green (CFVI) have been postulated such as: a) It saves time. b) Prevents injuries associated with conventional IOC. c) The technique is more convenient as it requires only a preoperative intravenous injection of indocyanine green and fluorescent images obtained in real time at any time during surgery without the need for radiation. d) Allows surgeons to evaluate the extrahepatic bile duct easily and in a short period of time. e) It is a safe procedure.
Pujol et al.(33) compare fluorescence cholangiography with intraoperative cholangiography in a group of 82 patients undergoing laparoscopic cholecystectomy and found that the identification of biliary anatomy was greater and faster with CFVI. In 20 patients where IOC could not be completed, in 80% identification was achieved with indocyanine green. Indocyanine green cholangiography failed to identify any biliary structure in less than 5% of cases. Catalin et al.(34) analyzed the usefulness of CFVI in 65 patients undergoing laparoscopic cholecystectomy. They perform fluorescence before and after the dissection of Calot's triangle and determine in which patients the cystic duct and bile duct are identified and also correlate it with cholangioresonance images. In the randomized multicenter study by Van Den Vos et al. (35) to determine the effectiveness of indocyanine green in determining the drawing of the safety window during laparoscopic cholecystectomy, which should offer answers regarding the effectiveness of the technique and the doses used. In this sense, an interesting work by Ambe et al.(36), in which they compare different moments and different doses of administration, concludes that a dose of 0.25 mg/Kg administered 45 minutes before facilitates the safe intraoperative identification of the biliary tree. and considers that fluorescence cholangiography is a safe and effective practical method of identifying the bile duct. Kontantinos et al. (37) determined that it is much cheaper than IOC ($778 vs. $14), much faster (consuming 10 times less time), easy to perform by surgeons, and at least as effective as IOC.
In our country there is no report of its use, nor experience considering it as another work tool to achieve a safe procedure, although there is still no uniform use of the VI. Furthermore, its use is limited during acute episodes of the extrahepatic bile duct or when a stone is lodged in the cystic duct. Furthermore, it has no use for the diagnosis of choledocholithiasis, although its introduction in bile duct surgery is not this. Where IOC continues to be of choice in the aforementioned for Pucher el al.(1) in SAGES expert Delphi consensus: critical factors for safe surgical practice in laparoscopic cholecystectomy.
Figure 6: The use of rescue techniques during a difficult cholecystectomy is shown.
Changes in strategies during cholecystectomy: in this group we will see a series of steps or techniques to avoid a BLI proposed by Brunt et al.(39) in a consensus on safe cholecystectomy (fig. 6), a) Use of the intraoperative pause and request a second opinion. b) consider conversion or use of another technique during surgery.
Surgical or intraoperative pause and request a second opinion: the intraoperative pause, before clipping or cutting any structure, if the anatomy is not clear and safe, it is recommended to perform a “pause”. This pause or time-out has the function of encouraging a calm look at the surgical situation and acting accordingly. This intraoperative pause is already part of the recommendations of the SAGES (Society of American Gastrointestinal Endoscopic Surgeons) guideline for the prevention of LIVB, and a critical vision pause is recommended in prospective studies. If SVC has not been achieved despite the measures described, the guidelines advise calling another surgeon for his opinion or requesting assistance. The surgeon must be careful and ask for help before taking any irreversible step.(38,39,40)
Consider conversion to laparotomy and other techniques: Conversion to laparotomy is one of the most frequent options to avoid LIVB in complex situations, by providing better exposure, being able to directly palpate and feel the anatomical structures. This option in difficult scenarios is increasingly less practiced by new generations of surgeons, making them inexperienced in difficult cases. An acute or exacerbated chronic inflammatory process, with retraction and inflammatory fusion of the bile/cystic duct is where manual identification of the structures is capable of reducing the risk of LIVB. Another circumstance where conversión is appropriate is uncontrollable bleeding.
Partial or subtotal cholecystectomy: it is an alternative in the course of a difficult LC, and can be performed laparoscopically or openly as proposed by Hajabandeh et al. (41) and Loh et al. (42) . According to Borie et al. (16) the indications for subtotal cholecystectomy are the same as for a conversion, particularly when SVC is not achieved. In these cases, a “direct” cholecystectomy must be performed (from fundus to basin) and if it is not possible to identify the structures, proceed to section of the gallbladder over the basin. There are two ways to perform partial cholecystectomy, fenestrant or restorative subtotal cholecystectomy. Both techniques share the resective phase and consists of partial direct neck dissection. In this dissection, caution must be taken when approaching the hepatic hilum to avoid traction of the bile confluent. Upon reaching the gallbladder neck, the gallbladder must be transversely sectioned and the intraluminal contents extracted. The fenestrant technique refers to leaving the BV mucosa connected to the peritoneal cavity, closing the cystic duct with a purse string intraluminally. We recommend the use of a drain in the sutured stump, due to the risk of bile leak. There is a technical variant of the subtotal fenestrant cholecystectomy or Pribram cholecystectomy. In this technique, the gallbladder is sectioned longitudinally, resecting its anterior side and leaving the side attached to the liver, avoiding. Electrocoagulation of the abandoned posterior wall mucosa is recommended to avoid mucin secretion in the postoperative period, a situation that has been described in the fenestrant technique.(1,3,4,11,16,40)
Cholecystostomy: it is an option in cases where the patient's anatomy or life may be seriously compromised. Fundal cholecystostomy can be performed with a Pezzer tube and drains left. This solution, although not definitive, allows cholecystectomy to be scheduled in a second time with better technical and local conditions.
Final Considerations
In conclusion, we can say that there are a series of methods, tools and strategies to globally reduce bile duct injuries, however these are not used systematically or uniformly worldwide. We consider the visualization of the Rouviere sulcus to begin the dissection as a constant element in this procedure, identification of the Budde-Calot triangle and sign of Lord Ganesha as a reference point towards an adequate visualization of Strasberg's critical vision, if this is not achieved it is ,the acting surgeon must use Fisher's method to complete the surgery or perform a rescue technique to avoid injury to the bile duct.
References
1.Pucher, P.H., Brunt, L.M., Fanelli, R.D. et al. SAGES expert Delphi consensus: critical factors for safe surgical practice in laparoscopic cholecystectomy. SurgEndosc 29, 3074–3085 (2015). Disponible en: https://doi.org/10.1007/s00464-015-4079-z
2.Wakabayashi G, Iwashita Y, Hibi T, Takada T, Strasberg SM, Asbun HJ et al. Tokyo Guidelines 2018: surgical management of acute cholecystitis: safe steps in laparoscopic cholecystectomy for acute cholecystitis (with videos). Journal of Hepato-Biliary-Pancreatic Sciences. 2018 Jan;25(1):73-86. Disponible en: https://doi.org/10.1002/jhbp.517
3. Manterola Carlos, Claros Nataniel. Morphology of Iatrogenic Lesions of the Bile Duct: Diagnostic and Therapeutic Aspects. Int. J. Morphol. [Internet]. 2022 Feb [cited 2022 Mar 21] ; 40( 1 ): 210-219. Available from: http://www.scielo.cl/scielo.php?script=sci_arttext&pid=S0717-95022022000100210&lng=es. http://dx.doi.org/10.4067/S0717-95022022000100210 .
4. Iwashita Y, Hibi T, Ohyama T, Umezawa A, Takada T, Strasberg SM,
et al. Delphi consensus on bile duct injuries during laparoscopic cholecystectomy: an evolutionary cul-de-sac or the birth pangs of a new technical framework? J HepatobiliaryPancreatSci. 2017;24:591-602. Available at: https://doi.org/10.1002/jhbp.503
5. Algieri, Rubén Daniel, et al. "Trigonocystohepatic: A Critical Anatomical Area for Surgical Safety." International Journal of Morphology 32.3 (2014): 860–865. Available at: https://scielo.conicyt.cl/pdf/ijmorphol/v32n3/art19.pdf .
6. Gómez, Francisco Ruiz, et al. "Iatrogenic Injuries of the Bile Duct." Cirugía Española 88.4 (2010): 211–221. Available at: https://doi.org/10.1016/j.ciresp.2010.03.045
Current knowledge on iatrogenic biliary tract injuries. Rev Cubana Cir [Internet]. 2017 Sep [cited 2022 Mar 21] ; 56( 3 ): 1-18. Available from: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0034-74932017000300005&lng=es .
8.Gupta, Vishal, and Gaurav Jain. "Safe laparoscopic cholecystectomy: Adoption of universal culture of safety in cholecystectomy." World journal of gastrointestinal surgery 11.2 (2019): 62. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6397793/
9. Álvarez Luis Fernando, Rivera Diego, Esmeral Miguel Evaristo, García Marta Cecilia, Toro Diego Fernando, Rojas Olga Lucía. Difficult laparoscopic cholecystectomy, management strategies. rev. colomb. cir. [Internet]. 2013 July [cited 2022 Mar 20] ; 28( 3 ): 186-195. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S2011-75822013000300002&lng=en .
10. Claros Nataniel, Laguna Roger, Pinilla Ramiro. INTRAOPERATIVE STRATEGIES TO PREVENT BILIARY TRACT INJURY DURING LAPAROSCOPIC CHOLECYSTECTOMY. Rev. Méd. La Paz [Internet]. 2011 [cited 2022 Mar 15] ; 17( 1 ): 5-15. Available from: http://www.scielo.org.bo/scielo.php?script=sci_arttext&pid=S1726-89582011000100002&lng=es .
11. Manatakis, D.K., Papageorgiou, D., Antonopoulou, MI. et al. Ten-year Audit of Safe Bail-Out Alternatives to the Critical View of Safety in Laparoscopic Cholecystectomy. World J Surg 43, 2728–2733 (2019). Available at: https://doi.org/10.1007/s00268-019-05082-z
12. Jimenez Vera, Jose Marco. "Clinical and epidemiological characteristics and causes of conversion from laparoscopic cholecystectomy to open cholecystectomy in the surgery department of the Carlos Alberto Seguin Escobedo National Hospital during 2019." (2020).
13. Guevara-Morales, Guillermo R. "Relevance of critical safety vision as a standardized step in laparoscopic cholecystectomy." Surgery and Surgeons 87.4 (2019): 477-478. Available at: https://www.medigraphic.com/pdfs/circir/cc-2019/cc194q.pdf .
14. Strasberg, Steven M. “A three-step conceptual roadmap for avoiding bile duct injury in laparoscopic cholecystectomy: an invited perspective review.” Journal of hepato-biliary-pancreatic sciences vol. 26.4 (2019): 123-127. Available at: https://doi:10.1002/jhbp.616
15. Sanford DE, Strasberg SM. A simple effective method for generation of a permanent record of the critical view of safety during laparoscopic cholecystectomy by intraoperative “doublet” photography. J Am Coll Surg. 2014;218:170-8. Disponible en: https://doi.org/10.1016/j.jamcollsurg.2013.11.003
16. Borie, Frederic et al. “SAGES SAFE CHOLE program changes surgeons practice in France-results of the FCVD implementation of SAFE CHOLE in France.” Surgical endoscopy vol. 37,8 (2023): 6483-6490. Disponible en: https://doi:10.1007/s00464-023-10128-4
17. Yadav, Ashok K., and Jeevan Kankaria. "Ten-point Strategy for Safe Laparoscopic Cholecystectomy: A Prospective Study." World 13.2 (2020): 56. Disponible en: https://www.iosrjournals.org/iosr-jdms/papers/Vol19-issue3/Series-16/G1903163036.pdf
18. Tantia, O., Jain, M., Khanna, S. et al. Iatrogenic biliary injury: 13,305 cholecystectomies experienced by a single surgical team over more than 13 years. SurgEndosc22, 1077–1086 (2008). Disponible en: https://doi.org/10.1007/s00464-007-9740-8
19. Barauskas, Giedrius, et al. "Referral pattern, management, and long-term results of laparoscopic bile duct injuries: a case series of 44 patients." Medicina 48.3 (2012): 19. Disponible en: https://doi.org/10.3390/medicina48030019
20. Marcos Yto, Eder. "Critical view of safety and biliary tract injury after laparoscopic cholecystectomy in patients aged 18 to 60 years treated in the General Surgery Department of Cayetano Heredia Hospital, 2017-2019." (2020). Available at: https://hdl.handle.net/20.500.12866/8476
21. Muñoz C. César, Inzunza Martín, Marino Carlo, Martínez Jorge. How to avoid bile duct injury in laparoscopic cholecystectomy: Beyond the critical safety view. Rev. cir. [Internet]. 2021 Jun [cited 2022 Mar 15] ; 73( 3 ): 362-369. Available from: http://www.scielo.cl/scielo.php?script=sci_arttext&pid=S2452-45492021000300362&lng=es. http://dx.doi.org/10.35687/s2452-45492021003927
22. Basukala, Sunil et al. “Rouviere's sulcus - An anatomical landmark for safe laparoscopic cholecystectomy: A cross-sectional study.” Annals of medicine and surgery (2012) vol. 75 103404. 1 Mar. 2022, Disponible en: https://doi:10.1016/j.amsu.2022.103404
23. Singh, Mohinder, and Neeraj Prasad. "The anatomy of Rouviere's sulcus as seen during laparoscopic cholecystectomy: A proposed classification." Journal of minimal access surgery 13.2 (2017): 89.
24. Cheruiyot, Isaac, et al. "The prevalence of the Rouviere's sulcus: A meta?analysis with implications for laparoscopic cholecystectomy." ClinicalAnatomy 34.4 (2021): 556-564. Disponible en: https://doi.org/10.1002/ca.23605.
25. Al-Naser, Mumtaz KH. "Rouviere's sulcus: a useful anatomical landmark for safe laparoscopic cholecystectomy." International Journal of Medical Research & Health Sciences 7.1 (2018): 158-161. Disponible en: https://www.ijmrhs.com/medical-research/rouvieres-sulcus-a-useful-anatomical-landmark-for-safe-laparoscopic-cholecystectomy.pdf.
26. Elwan, Ayman M. "Critical view of safety and Rouviere’s sulcus: extrahepatic biliary landmarks as a guide to safe laparoscopic cholecystectomy." The Scientific Journal of Al-Azhar Medical Faculty, Girls 3.2 (2019): 297. Disponible en: https://doi.org/10.4103/sjamf.sjamf_7_19
27. Lockhart, Stuart, and Gurpreet Singh-Ranger. "Rouviere's sulcus—Aspects of incorporating this valuable sign for laparoscopic cholecystectomy." Asian journal of surgery 41.1 (2018): 1-3. Available at: https://doi.org/10.1016/j.asjsur.2016.07.012
28. Oliva, Marcelo, et al. "Selective Intraoperative Cholangiography and Bile Duct Injury During Laparoscopic Cholecystectomy." Acta Gastroenterológica Latinoamericana 48.1 (2018): 13–22. Available from: https://www.redalyc.org/articulo.oa?id=199355697020 .
29. Flum DR, Dellinger EP, Cheadle A et al. Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA 2003; 289: 1639-1644. Disponible en: https://doi.org/10.1001/jama.289.13.1639
30. Awan, Bakhtawar et al. “A Systematic Review of Laparoscopic Ultrasonography During Laparoscopic Cholecystectomy.” Cureus vol. 15,12 e51192. 27 Dec. 2023, Disponible en: https://doi:10.7759/cureus.51192
31. Pesce, Antonio, et al. "Near-infrared fluorescent cholangiography–real-time visualization of the biliary tree during elective laparoscopic cholecystectomy." Hpb 20.6 (2018): 538-545. https://doi.org/10.1016/j.hpb.2017.11.013
32. Pérez-Saborido, B., M. Toledano-Trincado, and D. Pacheco-Sánchez. "Use of indocyanine green to prevent iatrogenic biliary tract injuries during laparoscopic cholecystectomy." Cirugía Andaluza 30.2 (2019): 228–234.
33. Pujol-Cano, Natalia et al. “Near-infrared fluorescence cholangiography at a very low dose of indocyanine green: quantification of fluorescence intensity using a color analysis software based on the RGB color model.” Langenbeck's archives of surgery vol. 407.8 (2022): 3513-3524. Available at: https://doi:10.1007/s00423-022-02614-5
34. Alius, Catalin et al. “When Critical View of Safety Fails: A Practical Perspective on Difficult Laparoscopic Cholecystectomy.” Medicina (Kaunas, Lithuania) vol. 59,8 1491.19 Aug. 2023, Disponible en: https://doi:10.3390/medicina59081491
35. Van Den Bos J, Schols RM, Luyer MD, Van Dam RM, Vahrmeijer AL, Meijerink
WJ, et al. Near-infrared fluorescence cholangiography assisted laparoscopic
cholecystectomy versus conventional laparoscopic cholecystectomy (FALCONtrial): Study protocol for a multicenter randomised controlled trial. BMJ Open 2016;6:1-9. Disponible en: https://doi.org/10.1136/bmjopen-2016-011668
36. Ambe, Peter C., et al. "The role of indocyanine green fluoroscopy for intraoperative bile duct visualization during laparoscopic cholecystectomy: an observational cohort study in 70 patients." Patient Safety in Surgery 13.1 (2019): 1-7. Disponible en: https://doi.org/10.1186/s13037-019-0182-8.
37. Georgiou, Konstantinos et al. “Intraoperative cholangiography 2020: Quo vadis? A systematic review of the literature.”Hepatobiliary& pancreatic diseases international : HBPD INT vol. 21,2 (2022): 145-153. Disponible en: https://doi:10.1016/j.hbpd.2022.01.002
38. Micó Obama Benjamín, León Goire Walter Lizardo, Romaguera Barroso Danilo, Lozada Prado Guido Alfonso, Rodríguez Fernández Zenén. Characterization of patients with iatrogenic surgical injuries of the biliary tract. MEDISAN [Internet]. 2015 Dec [cited 2022 Mar 15] ; 19( 12 ): 1507-1518. Available from: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1029-30192015001200010&lng=es .
39. Brunt, Michael L, et al. Safe cholecystectomy multi-society practice guideline and state-of-the-art consensus conference on prevention of bile duct injury during cholecystectomy. Ann Surg. 2020; 272:3-23. Available at: https://doi.org/10.1097/SLA.0000000000003791
40. Jara G, Rosciano J, Barrios W, Vegas L, Rodriguez O, Sánchez R, et al. Subtotal laparoscopic cholecystectomy as a safe surgical alternative in complex cases. Cir Esp. 2017;95:465-70. Available at: https://doi.org/ 10.1016/j.ciresp.2017.07.013
41. Hajibandeh, Shahin et al. “Meta-analysis of fenestrating versus reconstituting subtotal cholecystectomy in the management of difficult gallbladder.” HPB : the official journal of the International Hepato Pancreato Biliary Association vol. 26,1 (2024): 8-20. Available at: https://doi:10.1016/j.hpb.2023.09.005
42. Loh, Alex Y H et al. “Short and long term outcomes of laparoscopic fenestrating or reconstituting subtotal cholecystectomy versus laparoscopic total cholecystectomy in the management of acute cholecystitis.” HPB : the official journal of the International Hepato Pancreato Biliary Association vol. 24,5 (2022): 691-699. Disponible en: https://doi.org/10.1016/j.hpb.2021.09.018.
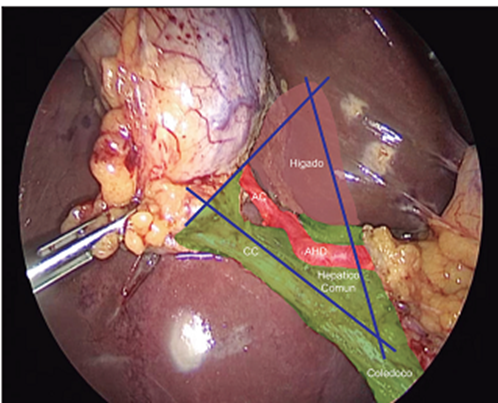
Figure 1
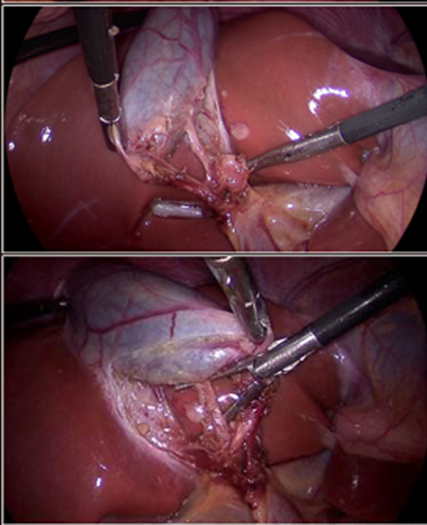
Figure 2
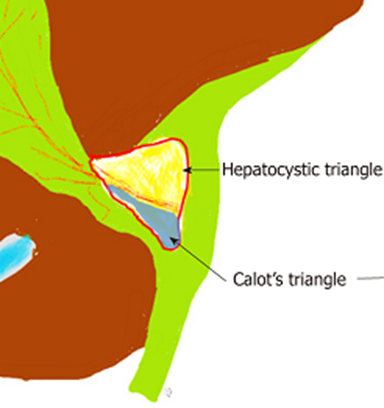
Figure 3
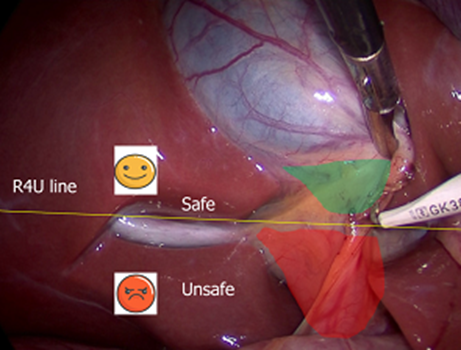
Figure 4
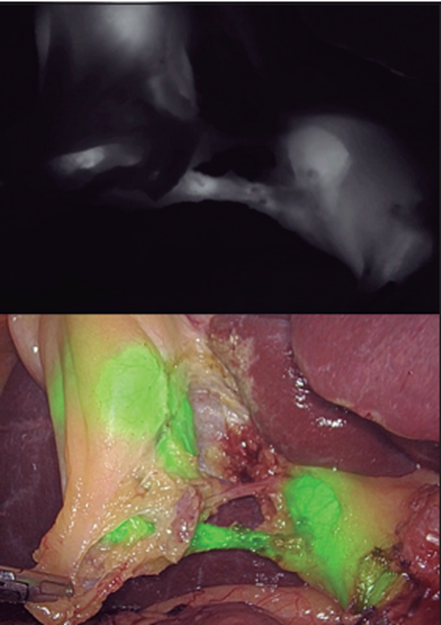
Figure 5
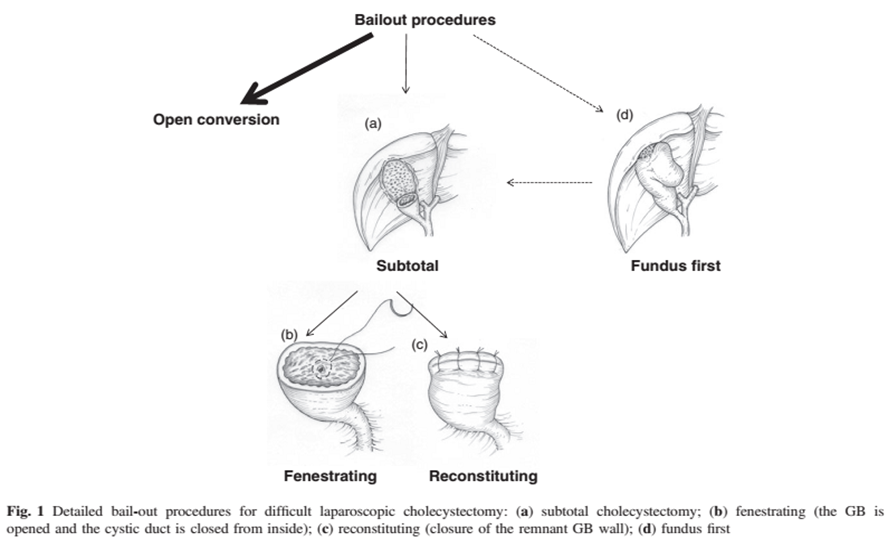
Figure 6