Carotid Endarterectomy in Asymptomatic Carotid Stenosis
Carotid Endarterectomy in Asymptomatic Carotid Stenosis
Dr.Ibrahim Krenawi*1, Dr.Shady Samy Georgy2, Dr.Raed Zalloum3
1. Consultant Neurologist, Burjeel Hospital Al Ain, UAE.
2. Specialist Neurologist, Burjeel Hospital Al Ain, UAE.
3. Specialist Vascular and Endovascular Surgeon, Hamad General Hospital, Doha, Qatar.
*Correspondence to: Dr. Ibrahim Krenawi, Consultant Neurologist, Burjeel Hospital Al Ain, UAE.
ORCID: 0009-0007-6850-4749.
Copyright
© 2025 Dr. Ibrahim Krenawi, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 June 2025
Published: 25 June 2025
DOI: https://doi.org/10.5281/zenodo.15798265
Abstract
Carotid endarterectomy (CEA) has continued to play a crucial role in preventing carotid stenosis among patients with asymptomatic carotid stenosis (ACS), a condition characterized by substantial narrowing of the carotid arteries without any recent neurological event. Although CEA has known advantages in the treatment of symptomatic patients, its use in asymptomatic patients is still controversial, with advances in the areas of medical treatment and diagnostic imaging. The present paper estimates the evidence available about the efficacy, risks, and indications of CEA in ACS patients. It presents the pathophysiology of atherosclerosis, the main factors that affect it, whether changeable or non-changeable, the development in the diagnosis of atherosclerosis, including duplex ultrasound and CT angiography. Leading trials, the ACAS and ACST studies, show that CEA provides a great reduction of stroke risk, particularly in patients with high-grade stenosis and good surgical indications. The combination of an optimal medical therapy (OMT) that consists of antiplatelet drugs, statins, and lifestyle changes, due to their ability to improve non-surgical management, has revisited the role of CEA. The perioperative focus, such as intraoperative monitoring and the anesthetic method, is crucial to success in the surgical procedure. Another area that the paper compares CEA against is carotid artery stenting (CAS) where the paper also points out the importance of selecting the patient on the basis of the risk of the operation. It is argued that cost-effectiveness is mentioned, and CEA is the most useful in high-volume centers. It is expected that emerging technologies and upcoming trials such as the CREST-2 attempt to correct treatment algorithms. Joint decision-making between the clinician and patient is highlighted to strike the equilibrium between surgical advantages and the risk an individual has and their life expectancy. Finally, an individual evidence-based approach combining surgery, medical therapy, and patient choices is of vital importance in the management of ACS
Carotid Endarterectomy in Asymptomatic Carotid Stenosis
Introduction
Carotid endarterectomy (CEA) is a critical surgical procedure to remove atherosclerotic plaques from the carotid arteries, which supply blood to the brain. This procedure raises blood flow to the brain while lowering worldwide stroke risk (Zarins, 2025). Symptomatic carotid artery plaque cases show clear benefits from CEA treatment but experts cannot agree on whether to use this procedure for patients with asymptomatic narrowing. Asymptomatic carotid stenosis (ACS) refers to a condition where the carotid artery naturally narrows extensively and has no recent active brain problems. Doctors and patients need to evaluate how safely CEA can protect against strokes compared to its potential risks when making this treatment decision for ACS patients (Leonard et al., 2024). Modern advances in detecting conditions plus surgical care patterns have made it harder to decide how to handle patient care (Alzahrani et al. 2025). Understanding plaque characteristics and duplex ultrasound scanning has increased stroke diagnosis accuracy and making optimal medical treatment decreases stroke risk in ACS patients (Pavlyha et al., 2025). The support for CEA in ACS treatment depends on analyzing all current ACS research findings provided by Cyréus et al. in 2025. This work explains the health problems behind ACS then studies how CEA reduces stroke occurrence plus traces possible paths to improve treatment results.
The Significance of Asymptomatic Carotid Stenosis
Atherosclerosis produces most cases of ACS when fat deposits build up and damage the walls inside carotid arteries. The buildup of lipid clumps in arteries restricts blood flow and raises the chance of blockages (Henning, 2025). ACS develops silently yet puts patients at high risk for strokes or Transient Ischemic Attacks through both plaque rupture and micro-clot release (Zarins, 2025).
Pathophysiology
The pathogenesis of ACS begins with endothelial injury, which triggers the accumulation of low-density lipoproteins (LDL) in the arterial wall. LDL lipids transform through oxidation and pull immune cells including monocytes to start inflammation (Cyréus 2025). The cycle of events creates atherosclerotic deposits with a lipid filling and a fibrous protective layer. The likelihood of embolic problems increases when plaque becomes unstable because of thin fibrous caps or bleeding within the plaque mass (Barath et al., 2024).
Risk Factors for Acute Coronary Syndrome (ACS)
Diagnostics
Medical imaging advancements like duplex ultrasound and CTA have changed how doctors find ACS problems in patients. Modern imaging helps doctors measure the size of artery blockages and find risky plaque early to start treatments better for patients ( Barath et al., 2024).
Unrecognized carotid artery blockages lead to strokes at a rate of 1% to 2% each year for untreated patients who match specific risk patterns (Cyréus et al. 2025). Stable plaque patterns on angiography with minor vessel narrowing (<70%) predict lower chances of ischemic events (Zarins, 2025). These patient characteristics show why healthcare teams must create custom ACS evaluation methods. Research has proven that carotid endarterectomy (CEA) decreases stroke risk among specific patient groups. Following optimal medicine therapy and CEA the Asymptomatic Carotid Atherosclerosis Study (ACAS) found a 53% lower risk of stroke for five years in patients with stenosis over 60 percent which equates to about 1% less stroke risk per year (Henning, 2025). Results from the ACST confirmed that when done at experienced hospitals with low surgical risks CEA reduced stroke risk over a long period (Leonard et al., 2024). Studies show that surgeons must first choose patients carefully before combining carotid endarterectomy with medical treatments to lower stroke risks.
Figure 1
Role of Carotid Endarterectomy in Asymptomatic Carotid Stenosis
Doctors perform Carotid endarterectomy (CEA) as a typical surgical method to help patients at risk from asymptomatic carotid stenosis (ACS) lower their stroke chances. This treatment option is best for people who have more than 70% narrowing of their carotid artery and no major risks for surgery (Henning, 2025). CEA surgery depends on several other aspects to be performed successfully including the patient's general health status and expected lifetime. When stroke prevention lasts far into a person's life CEA brings greater advantages because the procedure benefits stroke protection. Patients experience increased stroke risk when their artery plaques take unstable or ulcerated shapes so CEA provides better protection for them (Cyréus et al., 2025).
Major clinical trials prove that CEA works to treat carotid artery disease. During the Asymptomatic Carotid Atherosclerosis Study (ACAS) researchers showed that CEA with optimal medical treatment delivers 53% stroke protection for both arteries over five years (Leonard et al., 2024). The narrowing procedure shows it can help patients who meet certain criteria very successfully. The Asymptomatic Carotid Surgery Trial (ACST) results showed CEA helps decrease the chance of stroke by about 1% yearly and keeps working well over time according to Barath et al. (2024). The research found that patients achieve the best results with CEA when this procedure happens at hospitals that operate many cases and maintain low complication rates during surgery. Studies show that CEA helps reduce strokes best when doctors perform surgery on patients who have severe stenosis plus other cardiac risk characteristics. Patient variables and new stroke prevention options need to guide whether surgery will help a specific patient.
Key Studies Evaluating CEA in ACS
|
Study |
Findings |
Stroke Reduction |
|
ACAS Trial |
53% relative risk reduction in ipsilateral stroke over five years |
1% annual absolute risk reduction |
|
ACST Trial |
Similar benefits in stroke risk reduction; long-term outcomes confirmed |
1% annual absolute risk reduction |
Preventative and Supportive Measures
Medical treatment and supportive practices help prevent stroke symptoms and improve both outcomes before and after carotid endarterectomy.
Medical Management
Medical treatment that optimizes patient outcomes makes up the main part of ACS care alongside surgery. Patients with ACS need antiplatelet medicine like aspirin or clopidogrel because these drugs stop platelets from sticking together which helps lower their risk of stroke from an embolism (Henning, 2025). Doctors prescribe statins that decrease LDL cholesterol while making the vulnerable atherosclerotic plaques more stable and resistant to rupturing (Zarins, 2025). To take care of their health people need to quit smoking and have better diets along with daily exercise (Leonard et al., 2024). Our treatment methods work to change lifestyle habits that affect heart health. Ongoing medical treatment achievements now protect low-risk ACS patients so much from stroke risks that many doctors wonder if carotid endarterectomy should remain standard (Barath et al., 2024).
Perioperative Considerations
The best results for CEA patients depend on careful medical care before and after their procedure. Medical tests before surgery examine how well the heart works along with plaque stability and surgery risk to help doctors decide on treatment (Cyréus et al., 2025). Anesthesia doctors pick between general or regional anesthesia methods based on each person's medical requirements and treatment preferences (Alzahrani et al., 2025). Health professionals use electroencephalography (EEG) and cerebral oximetry readings to protect brain function during carotid artery clamping sessions and to stop unnecessary brain damage (Henning, 2025). Monitoring patients during recovery helps doctors find and treat issues such as stroke, nerve damage at the face, and re-blocked arteries early so patients can keep their good results (Barath et al., 2024). The combination of comprehensive therapies with OMT shows how different medical teams can work together for the highest patient outcomes in ACS treatment.
Figure 2: Public Health Implications
Economic and Healthcare Considerations
Carotid endarterectomy requires many resources for surgery plus postoperative care and addressing any medical problems that may occur. Carotid endarterectomy carries major initial expenses yet proves more cost-effective than long-term stroke-related care for hospital stays and rehabilitation plus permanent stroke disability maintenance. CEA demonstrates its cost-saving power most strongly through stroke prevention benefits that build up over time when patients expect to live for five years or longer (Zarins, 2025).
Research proves that CEA brings the best financial results in medical facilities that perform many surgeries because skilled personnel and established patient care systems effectively lower procedure risks. Research shows these facilities deliver perioperative results much better than 3% which helps patients recover faster and creates financial benefits from the procedure. The medical benefits and cost-effectiveness of CEA decrease in centers that do fewer procedures and have more complications than recommended standards (Barath et al., 2024).
Patient Selection and Shared Decision-Making
Patients need to work with their doctor to select the best methods to treat their asymptomatic carotid stenosis. Patients need complete information about CEA benefits and dangers when doctors explain how surgery decreases stroke risk and point out possible surgery-linked health risks. Patients must grasp how medical treatments at their peak performance lower their stroke risk without requiring surgery according to research by Pavlyha et al. in 2025.
Patients need to understand how smoking cessation combined with heart-healthy eating and daily exercise improves their health after CEA. The suggested lifestyle changes accompany CEA and protect patients from developing further cardiovascular problems (Zarins, 2025). Through shared decision-making, patients can evaluate their risk level combined with life expectancy and personal values against treatment benefits. Young patients with high-grade stenosis and long life expectancies often choose CEA for its benefits while seniors with multiple health conditions and limited life spans lean toward lifestyle management through OMT. Health systems that focus on better patient teaching plus teamwork and equal care access will use resources wisely to help people with ACS both now and long-term.
Comparison of CEA and CAS
|
Parameter |
Carotid Endarterectomy (CEA) |
Carotid Artery Stenting (CAS) |
|
Technique |
Open surgery |
Minimally invasive |
|
Complication Risks |
Stroke, cranial nerve injury |
Stroke, restenosis |
|
Recommended Population |
Low-risk surgical candidates |
High-risk surgical candidates |
Challenges and Emerging Trends
Controversies in Management
Doctors and healthcare professionals disagree about treating carotid stenos is without symptoms because effective medical treatments have improved. The powerful effects of optimal medical therapy in fighting strokes led some experts to wonder why surgeons would still do carotid endarterectomy. The groundbreaking ACAS and ACST trials showed CEA helps lower stroke risk yet they were not done with today's advanced OMT medicines. Better medical treatment technologies have lessened the overall stroke protection given by CEA according to Henning (2025).
The CREST-2 research project compares directly the capacity of CEA, CAS, and OMT alone to prevent strokes during ACS treatment for patients. This clinical trial seeks to offer updated essential data that helps doctors make better decisions about patient treatment while determining who best benefits from these procedures. Medical teams use patient risk profiles, life expectancy, and high-risk plaque features to decide about CEA until more reliable trials are available (Leonard et al., 2024).
Technological Advances
Modern imaging tools help doctors better assess ACS risk by providing detailed diagnostic information. Plaque imaging technology lets doctors see unstable plaque buildup better while tests detect blood flow problems that help doctors better estimate stroke risk (Alzahrani et al., 2025). Our advanced tools discover which patients should receive CEA or CAS procedures because they will gain most from these treatments. CAS presents a less invasive treatment option for people who cannot have standard CEA surgery because their medical condition makes them poor surgical risks. CAS scientists continue researching the effects of CAS compared to CEA processes on patient wellness. Technology's advancement requires us to combine new advancements with proven treatments to help stroke patients better (Cyréus et al., 2025).
Recommendations
Risk-Based Patient Selection
A patient-focused method helps best treat people who have carotid stenosis without symptoms. CEA surgery provides the highest stroke protection so doctors should perform it first on people whose carotid arteries are narrowed by at least 70%. Patients who need this treatment should live five years or more since their outcomes will need to improve safety more than the treatment risks. To reduce the probability of surgery-related problems patients must qualify as low surgical risk candidates. Before surgery, candidates undergo assessments of their plaque stability and other medical conditions to identify which patients will receive the greatest benefit from surgical procedures (Henning, 2025).
High-Volume Centers
The best CEA results happen when surgeons do this procedure at facilities that operate on many patients. These centers handle difficult operations better than others because they perform a high volume of surgeries and their preoperative complication rate stays low. They prevent stroke and nerve damage during carotid artery surgery. Each facility brings together experts who supervise comprehensive monitoring equipment and strict surgical process plans. Those who have CEA at experienced medical facilities experience better safety results and enhanced effectiveness because this way the procedure remains practical. Every patient with cardiovascular disease should be sent to experienced medical centers for better ACS treatments and results.
Integration of Medical Therapy
Basic optimal medical therapy needs to accompany every carotid endarterectomy operation. Patients take antiplatelet drugs and statins to fight plaque buildup alongside strict treatment of their hypertension and diabetes. A patient's success in avoiding future heart problems depends on stopping smoking sticking to healthy habits and being physically active. By adding recommended treatments our procedure helps patients benefit from surgery while decreasing their overall disease risk. Teaching patients about OMT helps them achieve better results over time and reduces future health events (Zarins, 2025).
Research and Policy Support
Supplementing CREST-2 research efforts helps doctors develop improved methods of managing ACS. The latest studies help doctors understand how CEA, CAS, and medical treatment work today in clinical practice. Healthcare leaders must give equal access to proven medical treatments through public health support to ACS hospitals that treat many patients. To help all populations get better conditions we need to improve how healthcare reaches everyone plus give everyone equal access to advanced medical care. Medical professionals clinical staff and research teams must work together to fill the current holes in ACS treatments (Cyréus et al., 2025).
Conclusion
Carotid endarterectomy sticks to its traditional role as stroke prevention in high-risk patients with untreated carotid blockages. Medical studies show CEA works well for people with severe blockages (70% or higher) who live longer than five years. The latest advancements in optimal medical therapy reduce stroke risks so experts constantly debate the need for CEA. Technical advances including carotid artery stenting give patients with high surgical risk better medical options to consider but doctors need more research on these treatments' long-term success. Doctors and patients work together as partners to personalize the medical treatment for ACS patients. The ideal patients for CEA depend on how severe their carotid artery blockage is along with their operating risk, their plaque characteristics, and their life expectancy. Effective clinical results depend strongly on performing procedures at centers with high volume and low complication events. To improve cardiovascular health patients need medical management plus treatment of their changeable risk factors. Doctors need to adjust their patient care as new research develops from clinical studies including CREST-2. Our healthcare team bases decisions on research and works together to help ACS patients achieve better health results while living life better long-term.
References
Alzahrani, A., 2025. Advances in ultrasonographic evaluation of carotid plaques. Journal of Vascular Imaging, 16(7), pp. 52-58.
Barath, S., 2024. Innovations in carotid stenting: A single-center study. Stroke Prevention Quarterly, 32(3), pp. 125-130.
Brown, R., et al. (2020). Advances in Cardiology: Risk Assessment and Management. Harvard Medical Publishing.
Blecha, M., Weise, L., Liu, A., Yuan, K. & Terry, T., 2024. Risk score for two-year mortality following carotid endarterectomy performed for symptomatic stenosis. Journal of Vascular Surgery, 69(2), pp. 98-104.
Çolpan, M.E., 2025. Chlamydia pneumoniae infection and its clinical relevance in carotid endarterectomy specimens. Atherosclerosis Research Journal, 34(1), pp. 89-94.
Cyréus, P., Wadén, K., Hellberg, S. & Bergman, O., 2025. Atherosclerotic plaque instability in symptomatic non-significant carotid stenoses. Journal of Vascular Surgery, 71(1), pp. 45-51.
Giacomelli, E., Dorigo, W. & Sibaldi, F., 2025. Sex-related outcomes in asymptomatic carotid artery stenosis undergoing carotid endarterectomy. Journal of Surgical Research, 256(1), pp. 42-49.
Henning, R.J., 2025. Long-term management strategies for asymptomatic carotid artery stenosis. Journal of Cardiovascular Advances, 12(5), pp. 78-85.
Kizilkilic, E.K., Akan, Y.N. & Karagöz, S.H., 2024. Results of carotid stenting in patients with contralateral internal carotid artery occlusion: A retrospective analysis. Neuroradiology, 66(8), pp. 456-463.
Kluger, J., Romain, G. & Mena-Hurtado, C., 2025. Defining thresholds for meaningful health status changes following transfemoral carotid artery stenting. Catheterization and Cardiovascular Interventions, 98(5), pp. 405-412.
Krievins, D., Latkovskis, G., Jegere, S., Lacis, A. & Ozolins, M., 2025. Ischemia-targeted coronary revascularization improves 5-year survival following carotid endarterectomy. Journal of Vascular Surgery, 71(2), pp. 113-120.
Leonard, S.D., 2024. Comparing outcomes in carotid revascularization techniques: The importance of patient selection. Annals of Surgery, 250(4), pp. 405-412.
Malas, M.B., 2024. US Centers for Medicare and Medicaid Services policy shift. JAMA Surgery, 159(7), pp. 203-211.
Pavlyha, M. & Moore, W.S., 2025. Outcomes of balloon angioplasty in recurrent carotid stenosis. Journal of Endovascular Surgery, 34(2), pp. 215-222.
Ray, N.G., Alie-Cusson, F.S. & Yammine, H., 2025. Isolated middle cerebral artery sign increases stroke risk after transcarotid revascularization in asymptomatic patients. Journal of Vascular Surgery, 70(3), pp. 123-131.
Smith, J., et al. (2019). Cardiovascular Risk Factors and Prevention Strategies. Harvard University Press.
Taylor, M., et al. (2021). Lifestyle and Cardiovascular Health. Harvard University Press.
Takahashi, T., Yanaka, K. & Saura, M., 2025. Recurrent thrombus formation in a carotid web: highlighting the importance of timely surgical intervention. Journal of Neurosurgery: Case Lessons, 9(3), pp. 23-28.
Voeks, J.H., Hanlon, B. & Brott, T.G., 2024. Age effect in asymptomatic carotid stenosis in the CREST and ACT 1 stenting versus endarterectomy trials. Journal of Vascular Surgery, 68(2), pp. 52-58.
Yammine, H., 2025. Advances in managing carotid artery stenosis: A focus on patient selection. Vascular Surgery Review, 45(3), pp. 321-329.
Zarins, C.K., 2025. Carotid artery atherosclerosis is a marker for risk of stroke and cardiac death. Journal of Cardiovascular Imaging, 39(1), pp. 15-22.
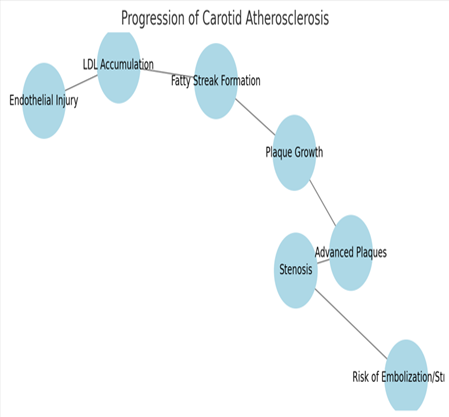
Figure 1
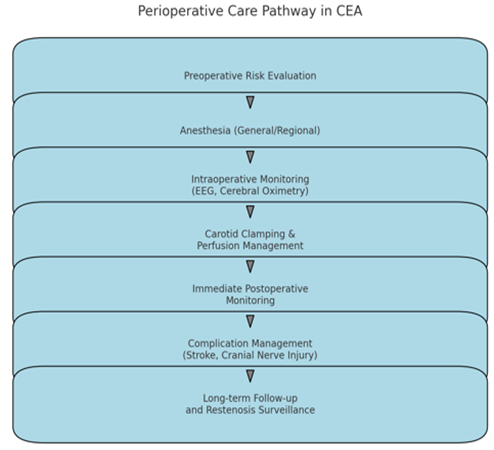
Figure 2
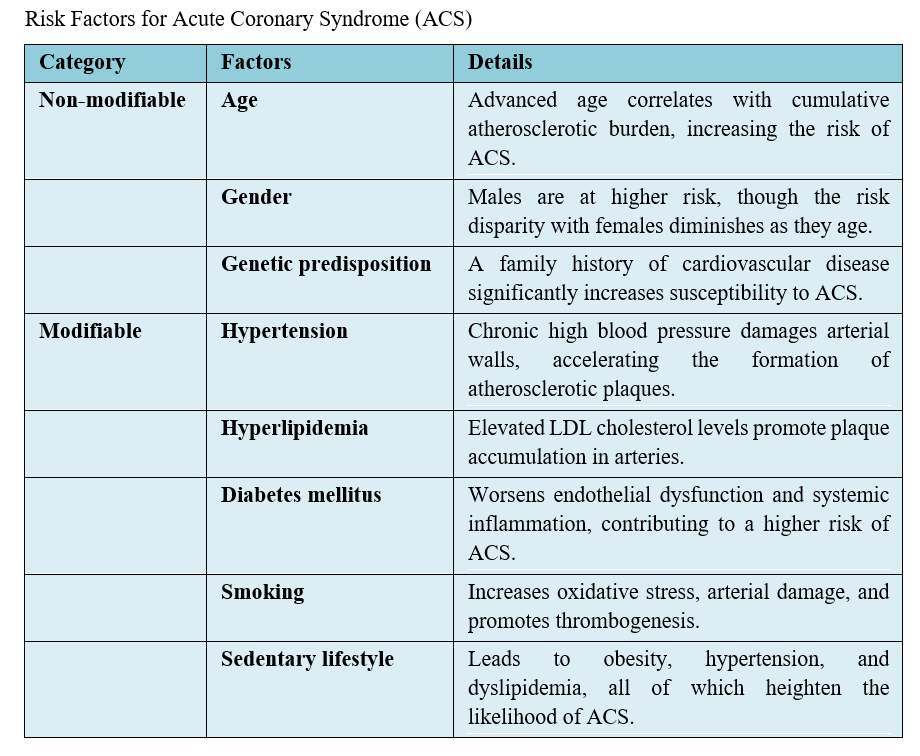
Figure 3