A Transmural Journey
A Transmural Journey
María Machín Delgado*1, Valentin Roales Gómez2, Esteban Martin Antona3, Alicia López García4, José Miguel Esteban López-Jamar5
2. Department of Gastroenterology, Hospital Clínico San Carlos, Madrid, Spain.
Orc ID: 0000-0003-4322-8956
3. Department of General and Digestive Surgery, Hospital Clínico San Carlos, Madrid, Spain.
Orc ID: 0000-0002-1568-2337
4. Department of Gastroenterology, Hospital Infanta Sofía, Madrid, Spain.
Orc ID: 0000-0001-9268-4259
5. Department of Gastroenterology, Hospital Clínico San Carlos, Madrid, Spain.
*Correspondence to: María Machín Delgado, Spain.
Copyright
© 2025 María Machín Delgado, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 May 2025
Published: 27 June 2025
A Transmural Journey
Introduction
The Nissen fundoplication is a commonly used surgical technique for the treatment of gastroesophageal reflux disease (GERD). In recent years, the concurrent use of surgical meshes has become widespread to prevent recurrences, although it can be associated with complications.
Clinical Case
61-year-old woman with gastroesophageal reflux disease and a type III hiatal hernia, who underwent laparoscopic Nissen fundoplication and hiatoplasty with a 360º microvalve mesh 9 years ago. She reports self-limited impactions over the past 5 years. She presents to the Emergency Department with aphagia after 15 days of epigastric pain, heartburn, and regurgitation.
An urgent gastroscopy is performed, revealing a food bolus which is fragmented and removed, exposing friable mucosa with oozing bleeding, decubitus ulcers, and a suture thread over a whitish area compatible with surgical mesh (Figure 1). Due to suspicion of pressure-induced perforation and risk of iatrogenic injury, the exploration is suspended without advancing into the gastric cavity.
The patient is admitted on a nil per os (NPO) diet with high-dose proton pump inhibitors. An elective gastroscopy shows the mesh incorporated into the wall of the esophagogastric junction (Figure 2). With the surgeon present, who provides key information about the surgical technique and materials used, the sutures closing the prosthesis in a complete ring are cut, followed by those anchoring it to the diaphragmatic crura using argon plasma coagulation, sphincterotome, and needle knife (Figure 3).
With extreme caution and under strict endoscopic control, traction is applied (Figure 4) to the material, achieving en bloc extraction (Figure 5). A CT scan was performed, ruling out complications (Figure 6). The patient was discharged after 4 days asymptomatic, with normal outpatient endoscopic follow-up.
Figure 1. Whitish, firm material with exposed suture thread following food bolus disimpaction, compatible with surgical mesh.
Figure 2. Surgical mesh partially embedded in the esophagogastric junction
Figure 3: Surgical sutures cut using endoscopic instruments
Figure 4: Release of surgical mesh into the gastric cavity after traction with a crocodile forceps.
Figure 5. Surgical mesh extracted en bloc..
Figure 6: hanges consistent with Nissen fundoplication, showing thickening and inflammatory alterations. No contrast extravasation or extraluminal gas bubbles observed.
Discussion
Laparoscopic Nissen fundoplication is currently the treatment of choice for surgical management of GERD (1), while other types of fundoplication are reserved for cases with compromised esophageal body motility. Due to high rates of hernia recurrence in the medium and long term—especially in type III and IV hiatal hernias—reinforcement of the gastroesophageal junction with hiatal surgical mesh has become popular. This aims to strengthen the closure of the diaphragmatic hiatus at the gastroesophageal junction and can reduce recurrence rates to 2–7% (2).
However, mesh placement is technically challenging due to the oblique orientation of the diaphragmatic crura and esophageal peristalsis, and the procedure carries risk of short-, medium-, and long-term complications. These have been reported in 2.3% of patients with an average latency of 23.4 months (3).
Complications include fibrosis, esophageal erosions, strictures, fistula formation, gastric and/or esophageal perforation, and mesh migration (2). Hiatal mesh migration may occur into the thoracic cavity—representing 0.5% of complications in large series—or into the gastrointestinal tract, which is exceptionally rare (4).
To date, no direct link has been established between the type of mesh material used and complication rates (5,6). However, some recent authors advocate for the use of biological meshes, which seem to result in fewer complications compared to synthetic meshes due to reduced perimaterial fibrosis (5).
Only exceptional cases of complete mesh migration into the digestive tract have been reported in the literature, typically treated with a combined laparoscopic-endoscopic approach (3).
This is the first documented case of en bloc surgical mesh removal using endoscopy in a single procedure. The collaborative approach between surgeon and endoscopist was key in guiding therapy and resolving intra-procedural uncertainties, clearly benefiting the patient through complete and immediate clinical resolution with no recurrence of GERD during follow-up.
References
1. Fernando Alcaide-Matas, Hernán Giordano, Ildefonso Campano-Cruz, Alejandro Fernández Alonso, Maurizio Meus, Alberto Gil-Iriondo, Claudia Bagur-Bagur. Migration of gastric fundoplication with intrathoracic perforation. Annals of Mediterranean Surgery. 2020;3(2):8–11.
2. Mehmet Emin Gönüllü, ?smet Özayd?n Nurgül, Alt?nsoy Hasan Can Demirkaya. Endoscopic Removal of Migrated Nissen Fundoplication Mesh. Duzce Med J. 2022;24(3):337–9.
3. Iago Rodríguez-Lago, Miguel Muñoz-Navas, Juan Carrascosa, Maite Betés, Víctor Valentí, Fernando Rotellar. Endoscopic removal of migrated mesh after laparoscopic Nissen fundoplication. Rev Esp Enferm Dig. 2012;104(11):605–6.
4. Hernández González JM, Pérez Lara FJ, Sanchiz Cárdenas EM, Galeote Quecedo T, Oehling de los Reyes H, del Rey Moreno A, et al. Mesh migration as a complication after hiatal hernia surgery. Cir Esp 2015;93(Special Congress):372.
5. Martín Rodrigo P, Rial Justo X, Gil Cidoncha L, Remírez Arriaga X, Equisoain Azcona A, Polaino Moreno V, et al. Esophageal inclusion of mesh after hiatoplasty for giant hiatal hernia. Cir Esp 2021;99(Special Congress 2):223.
6. Targarona EM, Bendahan G, Balague C. Mesh in the Hiatus. A Controversial Issue. Arch Surg. 2004;139(12):1286–1296.

Figure 1

Figure 2
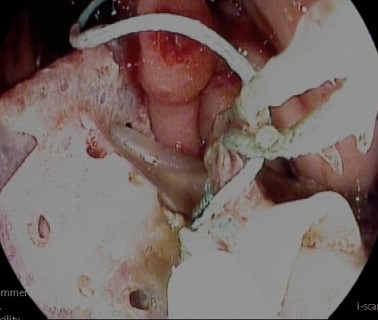
Figure 3

Figure 4

Figure 5
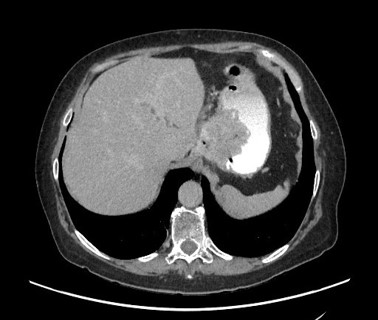
Figure 6