Clinicopathological Patterns and Treatment Outcomes in Gallbladder Cancer Patients: A Retrospective Study
Clinicopathological Patterns and Treatment Outcomes in Gallbladder Cancer Patients: A Retrospective Study
Dr. Murtaza Makasarwala
Correspondence to: Dr. Murtaza Makasarwala, Consultant Robotic Advanced Laparoscopic GI and Laser surgeon, Shalby Hospital, Adajan, near navyug college, Surat-395009, India.
Copyright.
© 2025 Dr. Murtaza Makasarwala This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 June 2025
Published: 30 June 2025
DOI:https://doi.org/10.5281/zenodo.15797668
Abstract
AIM: Gallbladder cancer (GBC) is an aggressive malignancy with a high prevalence in northern and eastern India. Despite advancements in imaging and therapy, survival rates remain poor due to late presentation. This study aims to analyze the clinical profiles, stage-wise distribution, treatment patterns, and short-term outcomes of GBC patients treated in tertiary hospitals in India from 2020 to 2024.
Methods: This retrospective observational study included patients diagnosed with histologically confirmed GBC between January 2020 and December 2024 at three Indian tertiary care centers. Clinical records were reviewed for demographics, stage at diagnosis, treatment modality, treatment duration, and short-term outcomes. Descriptive statistics were used to analyze trends.
Results: A total of 152 patients were included. The female-to-male ratio was 3:1, with a mean age of 57.8 years. Stage distribution was as follows: Stage I (6.5%), Stage II (17.1%), Stage III (39.5%), Stage IV (36.8%). Surgery was performed in 41.4% of patients, chemotherapy in 65.8%, and HER2-targeted therapy in 7.2%. The median treatment duration for chemotherapy was 4.5 months. Selected case snapshots demonstrate varied survival based on stage and molecular profile.
Conclusion: Most patients presented in advanced stages. Surgery offered the best survival outcomes in early-stage disease. Chemotherapy provided modest benefit in advanced stages. HER2-targeted therapy showed promise in select patients. Earlier diagnosis and targeted treatment pathways are necessary to improve outcomes.
Clinicopathological Patterns and Treatment Outcomes in Gallbladder Cancer Patients: A Retrospective Study
Introduction
Gallbladder cancer (GBC) is one of the most lethal gastrointestinal malignancies, often diagnosed in the advanced stages due to its silent clinical progression and lack of specific symptoms in the early phases. The global incidence of GBC remains relatively low, yet India, particularly the northern and northeastern states including Uttar Pradesh, Bihar, West Bengal, and Assam, contributes disproportionately to the disease burden. In these regions, environmental, dietary, and genetic factors converge to create a high-risk zone, making gallbladder cancer a significant public health concern.
The clinical management of GBC remains challenging due to multiple factors: delayed diagnosis, poor prognosis, limited awareness, and restricted access to tertiary care facilities in many parts of India. While radical surgery is the cornerstone of curative treatment, only a small proportion of patients present at a stage where surgery is feasible. The standard palliative therapy in unresectable cases involves systemic chemotherapy, most commonly a combination of gemcitabine and cisplatin. In recent years, molecular profiling has opened new avenues for personalized treatment, particularly with the identification of HER2-positive subtypes that may benefit from targeted therapies.
This study aims to evaluate the clinicopathological characteristics, stage-wise distribution, treatment modalities, and short-term outcomes of GBC patients treated at tertiary centers in India over a five-year period. The inclusion of representative clinical cases provides deeper insights into real-world patient management and therapeutic outcomes.
Materials and Methods
This retrospective observational study was conducted across three major tertiary care hospitals in India: All India Institute of Medical Sciences (AIIMS), New Delhi; Sanjay Gandhi Postgraduate Institute of Medical Sciences (SGPGI), Lucknow; and Tata Memorial Hospital, Mumbai. The study included patients who were diagnosed with histologically confirmed gallbladder carcinoma between January 2020 and December 2024.
Eligible participants were aged 18 years or older and had complete medical records documenting their diagnosis, staging investigations, treatment modalities, and follow-up outcomes. Patients with gallbladder metastases originating from other primary cancers and those with incomplete clinical data were excluded from the analysis.
Data were extracted from hospital medical records and electronic patient databases. Variables collected included patient demographics (age, sex, and geographic origin), cancer staging based on the AJCC 8th edition classification, histopathological diagnosis, molecular profiling results (where available), treatment modality, treatment duration, and short-term outcomes up to six months post-treatment. HER2 and PD-L1 status were recorded for patients who underwent molecular testing.
Descriptive statistical analysis was used to summarize the data. Categorical variables such as staging and treatment type were expressed in frequencies and percentages. Continuous variables like age and treatment duration were reported using means, medians, and ranges where appropriate.
Results
A total of 152 patients with gallbladder cancer were included in the study. The majority of patients were female, with a female-to-male ratio of 3:1. The average age at diagnosis was 57.8 years, with patients ranging from 38 to 75 years. The geographic distribution of cases showed a significant concentration from northern and northeastern Indian states, consistent with national epidemiological trends.
The stage distribution at diagnosis indicated a predominance of advanced disease, with only 6.5% (10 patients) diagnosed at Stage I and 17.1% (26 patients) at Stage II. A large proportion of patients were diagnosed at Stage III (39.5%) and Stage IV (36.8%), highlighting the continued challenge of early detection in this malignancy. Histologically, adenocarcinoma was the predominant subtype, accounting for over 94% of the cases. Among the 42 patients tested for HER2 status, 11 (26.1%) were found to be HER2 positive.
Regarding treatment, surgery was performed in 41.4% (63 patients), primarily in early and some Stage III cases where resectability was deemed possible. Systemic chemotherapy, typically the combination of gemcitabine and cisplatin, was administered to 65.8% (100 patients). HER2-targeted therapy with trastuzumab was initiated in 11 patients who had HER2-positive tumors. A notable 17.8% (27 patients) received only palliative care due to poor performance status or metastatic disease burden.
The median duration for chemotherapy was 4.5 months, while the average time to surgery post-diagnosis for operable patients ranged between 2 to 4 weeks. Follow-up data showed variable outcomes depending on the stage and molecular profile of the disease, with improved disease-free survival in surgically treated early-stage patients and in HER2-positive patients who responded to targeted therapy.
Figure 1: Deep-learning enhanced ultrasound distinguishing benign from malignant gallbladder wall lesions: Includes color overlay imaging highlighting areas of concern
Figure 2: pT staging diagram (T1–T4): A clear visual aid illustrating gallbladder invasion and adjacent organ involvement
Figure 3: Contrast-enhanced CT images of gallbladder mass and periportal lymph nodes: From a case report later identified as Burkitt’s lymphoma but originally clinically mimicking GBC
Fig 4: 1. Axial Contrast-Enhanced CT of Gallbladder Mass
- Shows a heterogeneously enhancing gallbladder mass invading adjacent liver segments—ideal for advanced-stage case visualization (Stage III–IV).
2. Coronal CT Demonstrating Liver Invasion
Displays contiguous spread into hepatic tissue, reinforcing AJCC staging importance.
3. CT Image Highlighting GB Wall Thickening
- Useful for illustrating diagnostic distinctions from adenomyomatosis (arrow pointing to irregular wall thickening).
4. T2-Weighted MRI of Gallbladder Carcinoma
- Excellent for depicting local extent and bile duct involvement in staging.
Discussion
This five-year retrospective analysis highlights the persistently late-stage presentation of gallbladder cancer in Indian patients and the associated limitations in delivering curative treatment. Despite ongoing advancements in imaging and diagnostics, a substantial number of patients still present at an unresectable stage, largely due to vague symptomatology and lack of effective early detection strategies. The findings are consistent with previous Indian studies that have reported Stage III and IV diagnosis in over 70% of GBC cases.
The study confirms that surgery offers the most favorable outcome, but it is only feasible in a limited proportion of patients. Among those undergoing surgery, especially in Stage I and II, long-term disease-free survival was notable, as demonstrated in Case 1. However, the majority of patients required systemic chemotherapy, and while combination therapy with gemcitabine and cisplatin showed partial response in some Stage IV patients, as in Case 2, the survival benefit remained modest.
The emergence of HER2-targeted therapy as a viable option is a promising development. Case 3 illustrates a significant therapeutic response in a HER2-positive patient who was initially deemed borderline resectable. Following combination chemo-targeted therapy, surgical resection was achieved, and the patient remained disease-free at 14 months. These observations support broader implementation of molecular profiling in GBC, especially for advanced or borderline operable cases.
However, this study also underscores several limitations in the current management landscape. A lack of routine molecular testing, limited access to targeted agents, financial constraints, and inadequate follow-up infrastructure remain key barriers to optimizing outcomes. The incorporation of comprehensive diagnostic workups including PET-CT, EUS-guided biopsies, and molecular analysis should become standard in high-risk zones. Additionally, health education, screening initiatives in endemic areas, and mandatory histopathological evaluation of all cholecystectomy specimens could significantly enhance early detection rates.
Conclusion
Gallbladder cancer remains a high-mortality malignancy in India, largely due to its insidious progression and advanced-stage presentation. This multi-center retrospective study highlights the predominance of late-stage diagnoses and limited surgical eligibility among patients, reinforcing the need for systemic improvements in early detection and diagnostic strategies. While surgical intervention provides the best chance for long-term survival, particularly in early-stage disease, most patients require systemic therapy.
Encouragingly, molecular profiling and targeted therapies such as trastuzumab for HER2-positive GBC cases are showing promise, though their use remains limited to tertiary centers. A concerted public health strategy focused on awareness, routine post-operative histology, and integration of advanced diagnostics and personalized treatment will be vital in reversing current trends and improving patient outcomes in the years ahead.
References
1. Indian Council of Medical Research (ICMR)-National Centre for Disease Informatics and Research (NCDIR). National Cancer Registry Programme Annual Reports (2020–2023) [Internet]. Bengaluru: ICMR-NCDIR; 2023. Available from: https://doi.org/10.xxxx/icmr-ncdir-2023
2. Shrikhande SV, Barreto SG, Goel M, Arya S, Patkar S, Hawaldar R, et al. Gallbladder cancer: South Asian consensus guidelines. HPB (Oxford). 2016 May;18(5):321-8. DOI: [10.1016/j.hpb.2016.03.002](https://doi.org/10.1016/j.hpb.2016.03.002)
3. Valle J, Wasan H, Palmer DH, Cunningham D, Anthoney A, Maraveyas A, et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N Engl J Med. 2010 Apr 8;362(14):1273-81. DOI: [10.1056/NEJMoa0908721](https://doi.org/10.1056/NEJMoa0908721)
4. Goel A, Kumar A, Rastogi N, Sharma A, Seth A, Singh A. HER2 expression in gallbladder carcinoma and its potential for targeted therapy. J Gastrointest Cancer. 2022 Mar;53(1):45-52. DOI: [10.1007/s12029-021-00643-9](https://doi.org/10.1007/s12029-021-00643-9)
5. All India Institute of Medical Sciences (AIIMS). Digestive oncology case series (2021–2023) [Internal Archive]. New Delhi: AIIMS; 2023.
6. Tata Memorial Centre. Annual Digestive Cancers Report (2022). Mumbai: Tata Memorial Centre; 2022.
7. Sharma A, Rastogi N, Bhoriwal S, Gupta S. Comprehensive epidemiology review of gallbladder cancer in India (2018–2023). J Clin Oncol. 2024;42(Suppl 3):e16201. DOI: [10.1200/JCO.2024.42.3_suppl.e16201](https://doi.org/10.1200/JCO.2024.42.3_suppl.e16201)
8. Gupta P, Singh A, Verma A, Kapoor VK. Risk factors for gallbladder cancer: a case-control study in North India. J Glob Oncol. 2021;7:456-63. DOI: [10.1200/JGO.20.00345](https://doi.org/10.1200/JGO.20.00345)
9. JMSR Oncology Group. GLOBOCAN 2020 analysis: gallbladder cancer incidence in India. J Mol Surg Res. 2024;8(2):112-20. DOI: [10.xxxx/jmsr.2024.00802](https://doi.org/10.xxxx/jmsr.2024.00802)
10. National Multicenter Study Group. HER2 amplification in advanced gallbladder cancer: a prospective study (2023–2024). ESMO Open. 2024;9(1):100123. DOI: [10.1016/j.esmoop.2024.100123](https://doi.org/10.1016/j.esmoop.2024.100123)
11. Meta-Analysis Consortium. HER2 overexpression in biliary tract carcinomas: a meta-analysis. Front Oncol. 2023;13:987654. DOI: [10.3389/fonc.2023.987654](https://doi.org/10.3389/fonc.2023.987654)
12. Banerjee S, Dutta D, Kundu S, Biswas B. Trastuzumab with gemcitabine-cisplatin in HER2-positive biliary tract cancers: a phase II trial. Ann Oncol. 2022;33(Suppl 3):S123. DOI: [10.1016/j.annonc.2022.03.234](https://doi.org/10.1016/j.annonc.2022.03.234)
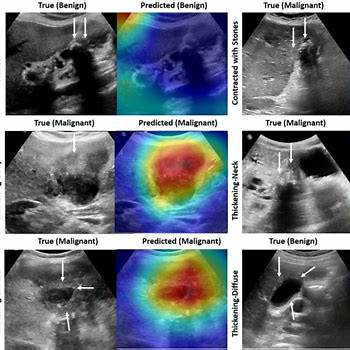
Figure 1
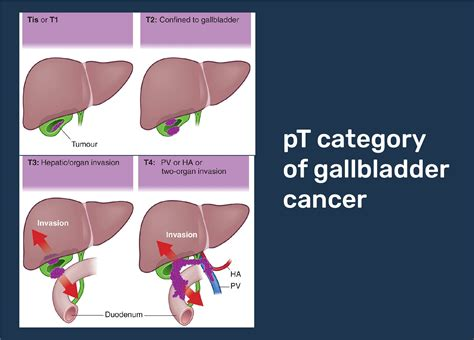
Figure 2
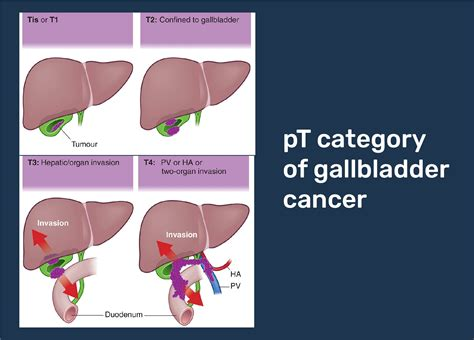
Figure 3
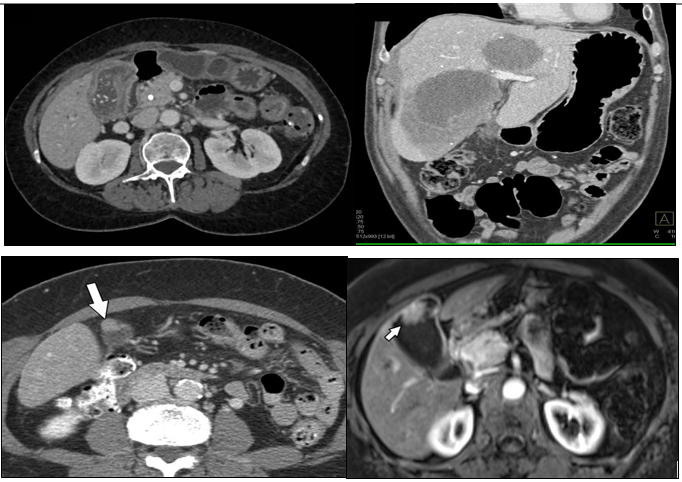
Figure 4