Left-Sided Gallbladder Encountered During Elective Laparoscopic Cholecystectomy: A Case Report and its Surgical Implications
Left-Sided Gallbladder Encountered During Elective Laparoscopic Cholecystectomy: A Case Report and its Surgical Implications
Zahoor Ahmad *1; Sali Mobarak Suliman Elsayed. 2
1: Zahoor Ahmad, General Surgeon, Mediclinic Alnoor Hospital –Abu Dhabi UAE
2: Sali Mobarak Suliman Elsayed, Resident General surgery, Mediclinic Alnoor Hospital –Abu Dhabi UAE.
*Correspondence to: Zahoor Ahmad, General Surgeon, Mediclinic Alnoor Hospital –Abu Dhabi UAE.
Copyright.
© 2025 Zahoor Ahmad This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 June 2025
Published: 30 June 2025
DOI:https://doi.org/10.5281/zenodo.15797830
Abstract
Left-sided gallbladder (LSGB) is a rare congenital anatomical anomaly, with an incidence reported between 0.1–1.2%. It is characterized by the gallbladder being located to the left of the falciform ligament, often beneath segment III of the liver. LSGB without associated situs inversus is the most common variation. This congenital anomaly can pose significant intraoperative technical challenges and increased risk of inadvertent biliary ducts injury particularly during laparoscopic procedures. We report a case of LSGB encountered intraoperatively during elective laparoscopic cholecystectomy, discuss the importance of, prompt intraoperative recognition of variation, knowledge about the anatomical variation and key intraoperative modifications that ensured a favourable surgical outcome.
Key Words: Left side gall bladder, intraoperative Cholangiogram ,gall bladder anomalies.
Left-Sided Gallbladder Encountered During Elective Laparoscopic Cholecystectomy: A Case Report and its Surgical Implications
Introduction
Left-sided gallbladder (LSGB) is a rare congenital anatomical variation, first described by Hochstetter in 1886 with its reported incidence of about 0.1-1.2% 1,2. Normally, the gallbladder is located in the gallbladder fossa under the right lobe of the liver, to the right of the falciform ligament. In LSGB, the organ is located to the left of the falciform ligament, typically under segment III of the liver. Three types of LSGB have been identified, with sinistroposition without situs inversus being the most common1,3,4.
LSGB is typically diagnosed incidentally, either through imaging or intraoperatively during procedures such as laparoscopic cholecystectomy. Its unusual location complicates surgical approaches due to altered anatomical landmarks, increasing the risk of biliary injury. so increased intraoperative vigilance is required on surgeons part. This report highlights a case of LSGB encountered unexpectedly during elective cholecystectomy and the importance of prompt recognition and technical adaptability to ensure a successful outcome.
Case Presentation
A 47-year-old man with no significant past medical and surgical history presented with Epigastric pain radiating to the back to urgent care. Clinical examination revealed mild clinical jaundice and mild right upper abdominal tenderness. Laboratory work up showed elevated liver function tests, normal lipase and slightly elevated inflammatory makers. Ultrasound revealed stones and sludge in the gallbladder. Subsequently patient was admitted to inpatient for further workup with Magnetic resonance cholangiopancreatography (MRCP) which ruled common bile duct obstruction or choledocholithiasis. Repeated Liver functions tests as outpatient normalized within few days, suggesting transient biliary obstruction cleared spontaneously .
The patient was scheduled for elective laparoscopic cholecystectomy. Intraoperatively, the gallbladder was found to be located to the left of the falciform ligament, attached to segment III of the liver, consistent with sinistroposition. The standard epigastric port was positioned slightly lower and more to the left to improve access and ergonomics. Due to altered anatomy A retrograde fundus-first dissection technique was employed. The gallbladder was mobilized from the left lobe and repositioned toward the right to approximate standard anatomical orientation. Dissection of Calot’s area was then performed with identification of the cystic duct and artery. A trans-cholecystic intraoperative cholangiogram was performed to clearly delineate biliary anatomy .So cystic was clearly identified and confirmed. Followed by clipping of cystic duct and artery and divided. the patient was discharged the next day and Postoperative recovery was uneventful.
Fig 1: Left sided gall bladder images before and after removal
Fig 2: Intra-operative Cholangiogram
Discussion
LSGB is a rare anatomical anomaly, with fewer than 150 cases reported since its first documentation[^1,^3]. It is categorized into two main types:
1. With situs inversus
2. Without situs inversus, which includes:
- Sinistroposition (true LSGB)
- Medioposition (falciform ligament displaced to the right)[^1,^4,^5]
The clinical presentation of LSGB generally mimics that of normally positioned gallbladders, often causing right upper quadrant or epigastric pain. This is because there is no corresponding neural transposition even if the gallbladder is left-sided[^4,^5].
Preoperative diagnosis of LSGB is challenging due to its usual clinical presentation and may be missed with usual imaging modalities like ultrasound and CT scan. Even sophisticated modalities such as MRCP(Magnetic resonance cholangiopancreatography) may fail to detect LSGB, as in our case (1,2,5). Therefore, prompt intraoperative recognition remains a crucial aspect in appropriate and safe intraoperative management.
Intraoperative technical modifications are essential for safe laparoscopic cholecystectomy in LSGB. These include:
• Adjusted port placement, especially relocating the epigastric port for better ergonomics
• Use of fundus-first dissection to align the gallbladder and cystic duct toward their usual orientation
• A low threshold for intraoperative cholangiography to delineate biliary anatomy and avoid inadvertent injury[^2,^4,^5,^6]
LSGB may be associated with biliary ductal and vascular anomalies which increase the risk of inadvertent biliary duct injuries 2,3,5. Therefore it is crucial to Adhere strictly to the basic principles of safe cholecystectomy and perform intra-operative cholangiogram 2,4,5,6 .intra-operative Cholangiogram is of immense help to confidently identify cystic before clipping and thereby helps in avoiding inadvertent injury to biliary ducts 2,4,5,6.
Conclusion
LSGB, though rare, must be kept in mind during laparoscopic cholecystectomy. Surgeons should be prepared to modify their technique and employ intraoperative Cholangiography to avoid complications. Early recognition and tailored surgical strategies are key to achieving safe and successful outcomes.
References
1 Ozsoy, M. S, Buyuker, F., Gapbarov, A., Colapkulu, N., Erol, C. I., Ek?nc?, O., Eren, T., & Alimoglu, O. (2018). Left-sided gallbladder without situs inversus?: report of a case. International Journal of Human and Health Sciences (IJHHS), 2(3), 158. https://doi.org/10.31344/ijhhs.v2i3.46
2. Doo-Ho Lee 1, Doojin Kim 1, Yeon Ho Park 1, Joo Seop Kim . Clinical significance and characteristics of left-sided gallbladder: case series study of 10 patients.Ann Surg Treat Res 2019 Dec 2;97(6):302–308. doi: 10.4174/astr.2019.97.6.302
3. Tali S, Çelik A. An Unusual Case: Atypical Localization of the Gallbladder. Am J Surg Case Rep. 2024;5(7):1143.
4. Talal Almas etal, Look, but to the left: A rare case of gallbladder sinistroposition and comprehensive literature review. nn Med Surg (Lond). 2021 Nov 1;71:103016. doi: 10.1016/j.amsu.2021.103016
5. Moses Amarjothi Joacquim 1, Kannan Devvygounder 2, Anbalagan P.
Left-Sided Gall Bladder: An Anatomic Rarity and Its Implications. Cureus. 2023 May 30;15(5):e39754.DOI: 10.7759/cureus.39754
6: Ding GQ, Cai W, Qin MF. Is intraoperative cholangiography necessary during laparoscopic cholecystectomy for cholelithiasis? World J Gastroenterol. 2015;21:2147–2151. doi: 10.3748/wjg.v21.i7.2147.
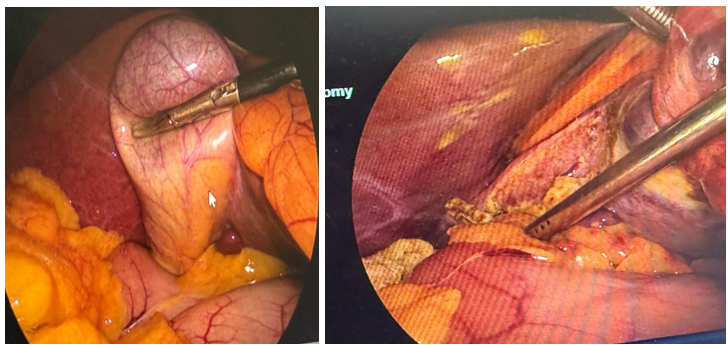
Figure 1
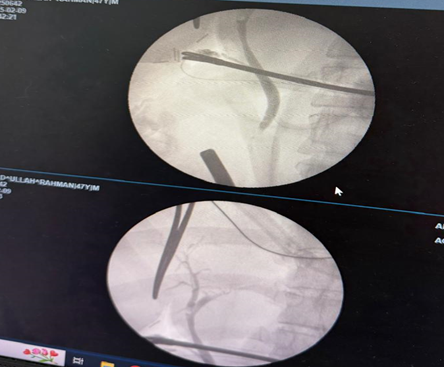
Figure 2