From Ether to Innovation: The Evolving Role of General Anesthesia in Dentistry.
From Ether to Innovation: The Evolving Role of General Anesthesia in Dentistry.
Dr. Hussein Moussawi*, Fatima Merza2
*Correspondence to: Dr. Hussein Moussawi, DMD, oral pathologist, impantologist. American board certified. Michigan, USA.
Copyright.
© 2025 Dr. Hussein Moussawi This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 Apr 2025
Published: 30 June 2025
DOI: https://doi.org/10.5281/zenodo.15837975
ABSTRACT
General anesthesia (GA) has become an essential modality in dental care, especially for patients with cognitive, behavioral, or physical limitations that preclude safe and effective treatment under local anesthesia or conscious sedation. This article explores the historical evolution of GA in dentistry, reviews contemporary literature on its indications, protocols, and outcomes, and presents a case involving a 33-year-old woman with Down syndrome who successfully underwent dental treatment under GA. This case exemplifies the ongoing relevance of GA in providing comprehensive, compassionate dental care to special needs populations, and underscores the importance of interprofessional collaboration and individualized care planning.
Keywords: General anesthesia, dentistry, Down syndrome, special care dentistry, intellectual disability, oral surgery, case report.
From Ether to Innovation: The Evolving Role of General Anesthesia in Dentistry.
Introduction
The use of general anesthesia in dentistry dates back to the mid-19th century, when ether was first administered to facilitate tooth extraction. Since then, anesthetic techniques have advanced dramatically, evolving from rudimentary inhalation agents to highly controlled, safe intravenous and inhalational protocols used in outpatient and hospital settings. General anesthesia has significantly broadened the scope of care for patients who cannot tolerate conventional dental treatment due to behavioral, psychological, or medical conditions.
FIRST AMERICAN PROCEDURE USING ANESTHESIA: Illustration of dentist William T.G. Morton & surgeon John Warren giving anesthesia to patient Glenn Abbott at Boston’s Massachusetts General Hospital on October 16, 1846. Illustration: Wikimedia Common
Case Report
2.1 Patient Background
A 33-year-old woman with a diagnosis of trisomy 21 (Down syndrome) was referred to the dental clinic for evaluation and management of persistent dental pain and visible decay. The patient exhibited limited verbal communication, heightened anxiety, and non-compliance with intraoral examination, making routine clinical and radiographic assessments in the outpatient setting unfeasible. A medical history review revealed no significant cardiac or respiratory comorbidities, although airway features typical of Down syndrome (macroglossia, narrow oropharynx) raised concerns for potential anesthetic complications.
2.2 Clinical Findings and Treatment Plan
Initial clinical observation and reports from the caregiver suggested carious lesions on the anterior maxillary teeth and signs of impaction of third molars. Given the behavioral challenges and anticipated need for extensive treatment, a comprehensive dental procedure under general anesthesia was scheduled in a hospital setting.
Under general anesthesia, full-mouth examination, radiographs, and treatment were completed. Findings included:
- Impacted mandibular and maxillary third molars with chronic pericoronitis.
- Extensive decay in teeth #7–10 requiring restoration.
- Generalized plaque accumulation and gingival inflammation.
Treatment included:
- Surgical extraction of all four third molars.
- Composite restorations of anterior teeth #7 through #10.
- Prophylaxis and oral hygiene instructions for caregivers.
Outcome and Follow-Up
The procedure was completed without intraoperative complications. Post-operative recovery was uneventful, and the patient demonstrated improved comfort, oral intake, and behavior within days. At the two-week and three-month follow-ups, healing was complete, restorations were intact, and oral hygiene had improved with caregiver reinforcement. The case was considered highly successful from both medical and quality-of-life perspectives.
Figure 1
Discussion
Historical Perspective
The first documented use of general anesthesia in dentistry occurred in 1846 when William Morton used ether for a tooth extraction. Since then, anesthetic techniques have evolved alongside advancements in pharmacology, anesthesiology, and surgical dentistry. In the past, GA was reserved for major oral surgeries, but its use has expanded into routine dental care for select patient populations.
Indications and Risk Assessment
Modern indications for GA in dentistry include:
- Inability to tolerate local anesthesia or sedation.
- Severe dental phobia or anxiety.
- Extensive or invasive dental needs.
- Special healthcare needs, including developmental disabilities.
Risk assessment tools such as the ASA Physical Status Classification System and pre-anesthesia medical evaluations help mitigate complications. When performed by qualified teams, the morbidity and mortality associated with GA in dental settings is extremely low.
Down Syndrome and Anesthesia Considerations
Individuals with Down syndrome present unique anesthetic challenges due to potential atlantoaxial instability, macroglossia, upper airway obstruction, congenital heart defects, and heightened sensitivity to sedatives. These factors necessitate careful airway assessment, collaboration with anesthesiologists, and hospital-based settings for GA.
In this case, multidisciplinary coordination between dental, anesthetic, and nursing teams ensured a safe and successful outcome.
Ethical and Access-to-Care Implications
Providing access to GA-supported dental care is both an ethical imperative and a public health concern. Untreated oral disease disproportionately affects individuals with disabilities, impacting their nutrition, communication, and quality of life. This case highlights how GA can remove a significant barrier to oral health equity.
Conclusion
General anesthesia remains a cornerstone of modern dentistry, particularly for underserved populations such as individuals with intellectual and developmental disabilities. The case presented here demonstrates the critical role GA plays in delivering safe, comprehensive, and compassionate care. As anesthesia practices continue to evolve, emphasis must be placed on training, infrastructure, and interprofessional collaboration to ensure this vital service remains accessible and safe for those who need it most.
References
1. Boynes SG, Moore PA, Lewis CL, Zovko J. Complications associated with anesthesia administration for dental treatment. Gen Dent. 2010;58(2):E20-E25.
2. Wilson KE, Welbury RR, Hosey MT. General anesthesia in pediatric dentistry. In: Pediatric Dentistry. Oxford University Press; 2016.
3. Nelson LP, Getzin A, Graham D, et al. Unmet dental needs and barriers to care for children with significant special health care needs. Pediatr Dent. 2011;33(1):29-36.
4. Glassman P, Miller CE. Dental treatment of fearful and uncooperative patients with developmental disabilities under general anesthesia. Spec Care Dentist. 2009;29(6):254-260.
5. Cote CJ, Wilson S. Guidelines for monitoring and management of pediatric patients during and after sedation for diagnostic and therapeutic procedures. Pediatr Dent. 2019;41(4):E26-E52.
6. Santoro JD, Steigman SA. Anesthetic considerations in individuals with Down syndrome. Anesth Prog. 2018;65(3):145–151.
7. Jastak JT, Donaldson D. Anesthesia and Sedation in the Dental Office. Philadelphia: W.B. Saunders; 1995.
8. Morgan JP, Minihan PM, Stark PC, et al. The oral health status of 4,732 adults with intellectual and developmental disabilities. J Am Dent Assoc. 2012;143(8):838-846.
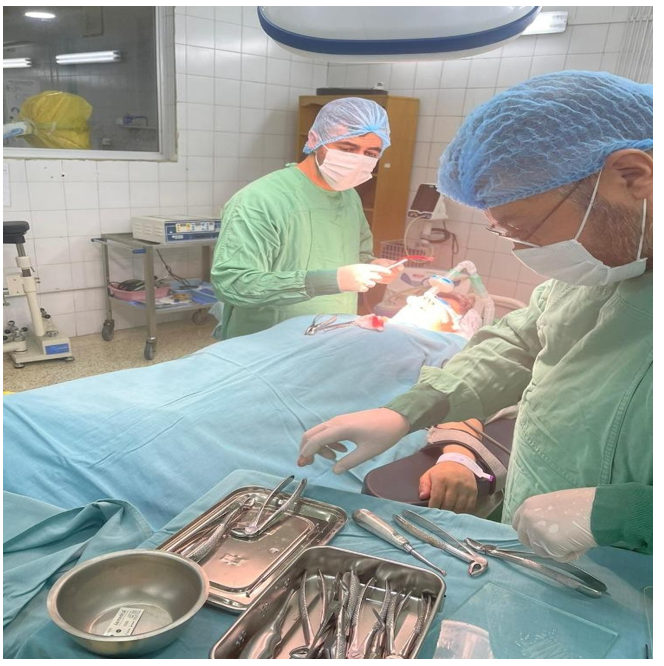
Figure 1