Case Report on the Removal of a Central Venous Catheter with Subsequent Neurological Event
Case Report on the Removal of a Central Venous Catheter with Subsequent Neurological Event
Dr.Ibrahim Krenawi*1, Dr. Fadoua Abdeluahid2
1. Consultant Neurologist, Burjeel Hospital Al Ain, UAE.
2. Senior Physician Neurologist, St.Barbara Hospital, Gladbeck, Germany.
*Correspondence to: Dr. Ibrahim Krenawi, Consultant Neurologist, Burjeel Hospital Al Ain, UAE.
ORCID: 0009-0007-6850-4749.
Copyright
© 2025 Dr. Ibrahim Krenawi, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 June 2025
Published: 01 July 2025
DOI: https://doi.org/10.5281/zenodo.15798296
Abstract
This case report presents a 48-year-old female patient with a significant medical history, including arterial hypertension, a history of multi-level thrombosis, and nicotine dependence. The patient underwent an extensive interdisciplinary diagnostic evaluation involving both pulmonology and vascular surgery.
Case Report on the Removal of a Central Venous Catheter with Subsequent Neurological Event
Background
The diagnostic process encompassed various imaging modalities, including echocardiography, magnetic resonance imaging (MRI) of the skull, computed tomography (CT) scans of the abdomen and thorax, bronchoscopy, bone scintigraphy, and histopathological analysis.
Findings
The diagnosis of non-small cell lung carcinoma was confirmed, classified as Stage IB adenocarcinoma, comprising 60% acinar and 40% lepidic components. Postoperative staging indicated pT2a (with visceral pleura involvement), pN0, cM0, L1, V0, Pn0, G2, and R0 status. A minimally invasive upper lobe resection was performed during the vascular surgical intervention, where intraoperative frozen section analysis validated the diagnosis of primary pulmonary adenocarcinoma. This was followed by an extensive radical lymph node dissection, encompassing interlobar, hilar, and mediastinal lymph nodes.
Clinical Course
Post-surgery, the patient was closely monitored in the intensive care unit (ICU). After demonstrating marked improvement, the central venous catheter was removed. Subsequently, the patient exhibited neurological symptoms indicative of left-sided hemiplegia, prompting her immediate transfer to the neurology department.
Neurovascular Assessment: An angiographic CT of the skull conducted during the neurological evaluation revealed the presence of air emboli in the cavernous sinus. Notably, echocardiographic assessment ruled out the presence of a patent foramen ovale (PFO), leaving the etiology of the air embolism due to several mechanisms unclear.
Primarily, they include a patent foramen ovale, the presence of right or left intrapulmonary shunts, and the forcing of air through the pulmonary filter. According to the literature on venous embolism, our case suggests that air likely migrated from the arm, passing through the right subclavian vein and entering the internal jugular vein on a cranial path. Once in the internal jugular vein, the air travels through the inferior petrosal sinus, ultimately reaching the cavernous sinus. Patients experiencing gas embolism may not exhibit symptoms; however, they can present with headache, nausea, vomiting, dizziness, or seizures. As the literature indicates, the etiology of these symptoms remains poorly understood.
Figure 1
Figure 2
Figure 3
Conclusion
This case underscores the complex interplay between the removal of a central venous catheter and neurological complications in patients with a history of vascular concerns. Further investigation is essential to elucidate the underlying mechanisms leading to such occurrences.
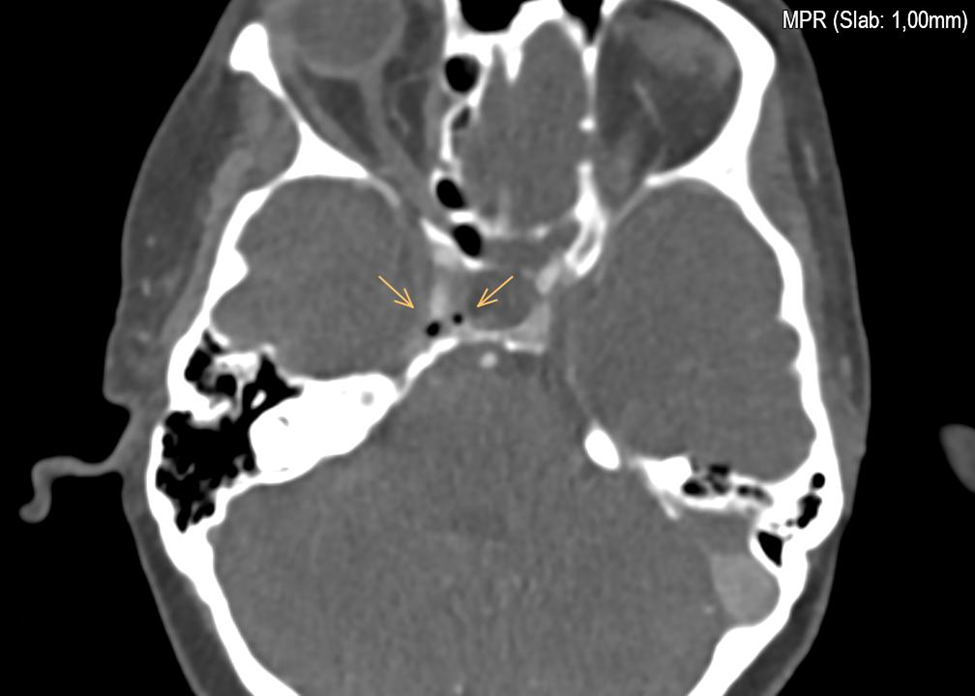
Figure 1
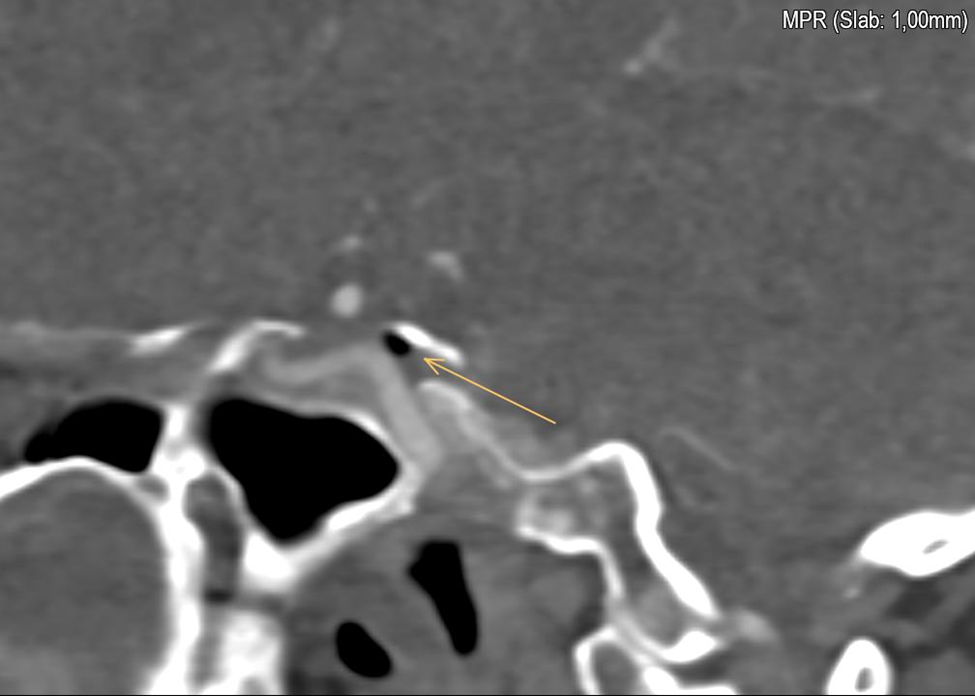
Figure 2
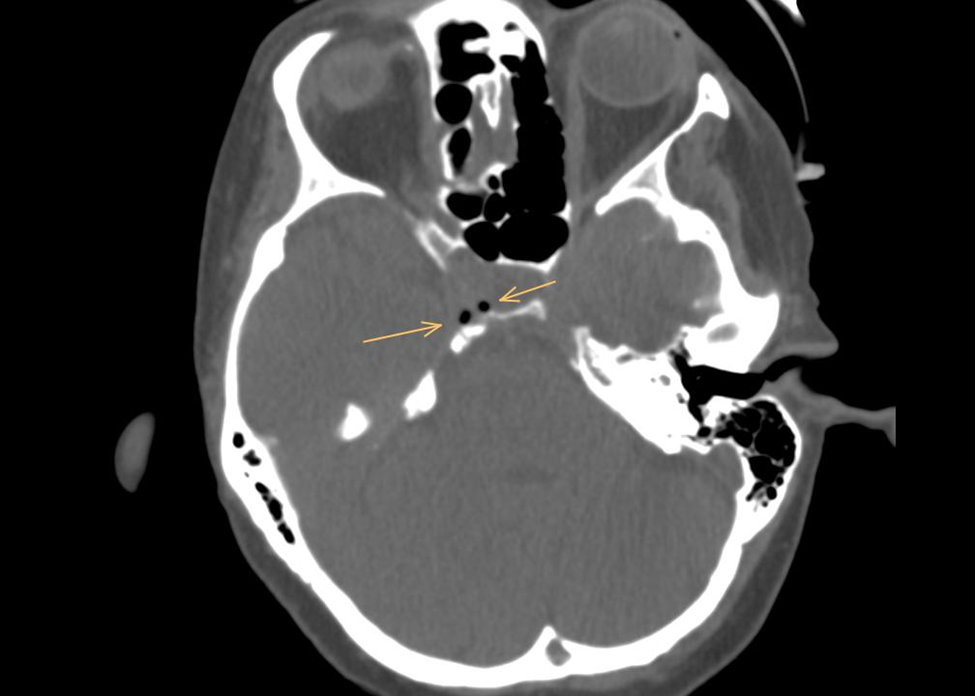
Figure 3