Minimally invasive versus full sternotomy aortic valve replacement and the integration of computed tomography imaging into clinical decision making: A Retrospective Observational Single-Centre study in the UK
Minimally invasive versus full sternotomy aortic valve replacement and the integration of computed tomography imaging into clinical decision making: A Retrospective Observational Single-Centre study in the UK
Pretesh Patel *1, Joon Lee2, Ishtiaq Ahmed3
1. Pretesh Patel. Brighton and Sussex Medical School, Brighton, England. 01273 523320
2. Joon Lee. Department of Radiology, Royal Sussex County Hospital, Brighton, England. 01273 696955
3. Ishtiaq Ahmed. Department of Cardiac Surgery, Royal Sussex County Hospital, Brighton, England. 01273 696955.
*Correspondence to: Ishtiaq Ahmed. Department of Cardiac Surgery, Royal Sussex County Hospital, Brighton, England
Copyright.
© 2025 Ishtiaq Ahmed This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 June 2025
Published: 04 July 2025
DOI: https://doi.org/10.5281/zenodo.15838132
Abstract:
OBJECTIVES: To compare clinical outcomes between full sternotomy (FS) and minimally invasive aortic valve replacement (MiAVR) and assess what proportion of MiAVR patients qualify for a right anterior mini-thoracotomy.
METHOD: A retrospective analysis was performed on 646 patients who underwent isolated AVR between 2014 and 2022 at our centre. Main outcome measures were aortic cross-clamping and cardiopulmonary bypass times, post-operative outcomes, hospital length of stay and mortality rates. Pre-operative CT scans of MiAVR patients assessed aortic valve annulus diameter, distance to the second intercostal space and ascending aorta location.
RESULTS: Aortic cross-clamping times (61.80 ± 27.48 vs 84.27 ± 24.24, P < 0.001) and cardiopulmonary bypass times (81.65 ± 34.12 vs 109.15 ± 28.55, P < 0.001) were significantly prolonged in the MiAVR group. No significant differences were observed in mortality, stroke risk, hospital length-of-stay, sternal infection and re-operative rates. Of the 77 CT scans analysed, 70.1% of MiAVR patients satisfied our criteria for a right anterior mini-thoracotomy procedure.
CONCLUSION: MiAVR is a safe technique with outcomes that are at least comparable with those demonstrated in FS cohorts. Despite prolonged aortic cross-clamp and cardiopulmonary bypass times following MiAVR, no adverse outcome was detected in this study. A substantial proportion of patients satisfying the criteria for a right anterior mini-thoracotomy though its practice must be viewed in the context of surgeon’s experience and institutional practice.
Key words: Minimally invasive aortic valve replacement, full sternotomy, propensity score analysis, computed tomography.
Minimally invasive versus full sternotomy aortic valve replacement and the integration of computed tomography imaging into clinical decision making: A Retrospective Observational Single-Centre study in the UK
Introduction
Aortic valve replacement (AVR) remains the only panacea for severe or symptomatic aortic stenosis. The traditional approach describes a full median sternotomy (FS) whereby the entire sternum is divided via a longitudinal incision which extends from the sternal notch to the xiphisternum (1). The safety and feasibility of FS has been extensively proven such that multiple high-volume centres worldwide employ this technique as the standard approach (2, 3).
Despite the prevalence of the FS approach, the sizeable extent to which the incision is made led to surgeons exploring the possibility of a less invasive approach (Figure 1). In 1993 Rao and Kumar describe the use of a right anterior mini-thoracotomy performed via a transverse incision in either the second or third intercostal space (4). This resulted in Cosgrove and Sabik coining the now widely accepted term ‘minimally invasive’ aortic valve replacement (MiAVR) (5). An important adaptation made by Liu et al. in 1999 denotes an upper J-shaped mini-sternotomy consisting of a partial median sternotomy to the third intercostal space (6, 7). This mini-sternotomy approach is the technique of choice for MiAVR in centres worldwide (8).
Whilst these minimally invasive incisions may result in a smaller and more aesthetically pleasing scar, there is an area of concern regarding operative time lengths. These pertain to the added complexity of MiAVR procedures given the limited cardiac exposure. Crucially, this may result in increased CPB and aortic cross-clamp times. The subsequent effects that these increases can potentiate on patient outcomes has been documented, with impacts seen on patient late survival and post-operative complications such as surgical site infections and acute kidney injury (9).
Figure 1. Full sternotomy incision compared to minimal access approaches. Adapted from (7).
A = Full sternotomy; B = Upper mini-sternotomy with ‘T’ incision; C = Upper mini-sternotomy with ‘J’ incision; D = Right anterior mini-thoracotomy
FS is generally well tolerated with excellent long-term outcomes (10). However the sternal interference has been shown to induce pain; reduce mobility; increase infection risk and impact on the patient’s ability to weight bear (11). Ultimately this can result in a prolonged recovery and hospital stay (12). Given the less-invasive nature of MiAVR it would be rational to think that these procedures would offer some benefit over FS, however, some uncertainty remains.
Additionally, the stringent anatomical criteria that right anterior mini-thoracotomy. patients must meet to be considered for a MiAVR warrants consideration. In these patients, an evaluation of the anatomical relationship between ascending aorta, aortic valve, sternum and intercostal space is performed by a pre-operative CT scan (13, 14). Currently, it is unknown the proportion of patients who may qualify for a mini-thoracotomy. If only a small proportion of patients meet these criteria, mini-thoracotomy practice may be deemed redundant particularly in comparison to the mini-sternotomy technique which possesses more relaxed anatomical criteria.
Aims
As such, this study will compare outcomes between FS and MiAVR undertaken at our centre and assess the advantages and limitations of each technique. This study will consider what proportion of patients who underwent MiAVR would qualify for a right anterior mini-thoracotomy via analysis of pre-operative CT scans.
Methods
Study design and population
A retrospective analysis was performed to compare post-operative outcomes in 646 patients who underwent isolated AVR between January 2014 and November 2022 at our centre. The operations were performed using either the standard FS approach (n=508) or MiAVR (n=138) by mini-sternotomy (n=135) or right anterior mini-thoracotomy (n=3).
The primary inclusion criteria for this study were patients requiring isolated AVR. Patients requiring concomitant procedures such as coronary artery bypass grafting or other valve surgeries; multiple valve replacements; re-operation on a previous AVR; other thoracic or vascular procedures; previous cardiac surgery and atrial fibrillation ablation were excluded from this study.
All pre-operative data and in-hospital outcomes were collected from medical records. The operative variables that were analysed include aortic cross-clamping times and CPB time, mortality rates, re-operative rates, post-operative complications and post-operative hospital stay.
Definition of outcomes
Mortality was defined as a death for any reason occurring during the same hospitalization regardless of the length. Post-operative arrhythmia is defined as a new onset of one of the following: atrial fibrillation / flutter, ventricular tachycardia, ventricular fibrillation or other arrhythmias which required temporary or permanent pacing.
Statistical analyses
Statistical analysis was performed using SPSS (version 28.0). Continuous data is expressed as a mean with standard deviations and the categorical data as numbers and percentages. A propensity score analysis was performed to reduce the effect of selection bias and potential confounding variables. A match tolerance of 0.01 was applied. The covariates which were matched include age, gender, weight, height, BMI, previous myocardial infarctions, smoking status, history of diabetes, hypertension, renal dysfunction, history of pulmonary disease, pre-operative arrhythmia and left ventricular ejection fraction. The final sample consists of 128 equally-matched propensity pairs of FS and MiAVR patients. Comparative analysis between the two cohorts was performed using the Student’s paired t-test. Significant differences were assessed using Pearson’s chi-squared test. All P-values reported are two-sided and a result was considered statistically significant when the P-value was ≤0.05.
Pre-operative CT imaging analysis for a right anterior mini-thoracotomy
Pre-operative CT images of the patients who underwent a MiAVR procedure were analysed using the Phillips Sectra PACS software. Recommendations for the optimal criteria used to consider patients for a right anterior mini-thoracotomy are described in previous papers (13, 14).
1. Aortic valve annulus sizing. The minimum and maximum annulus diameter are both greater than 20mm (Figure 2a).
2. More than one half of the ascending aorta is located rightward of the right sternal border at the level of the main pulmonary artery (Figure 2b).
3. Distance from the mid-clavicular line of the second intercostal space to the aortic valve is less than 120mm (Figure 2c).
Figure 2. Pre-operative CT imaging measurements. A: Aortic annulus sizing; B: Rightward ascending aorta; C: Distance from second intercostal space to aortic valve.
RV = Right ventricle; LA = Left atrium; dAo = Descending aorta
Results
Patient characteristics
Standard FS was performed in 508 patients (299 male and 209 female) and MiAVR was performed in 138 patients (91 male and 47 female). Comparisons of pre-operative data between unmatched FS and MiAVR groups are listed in Table 1.
|
Table 1. Baseline characteristics of between FS and MiAVR group prior to propensity score matching. |
|||
|
FS (n = 508) |
MiAVR (n = 138) |
P-value |
|
|
Age |
68.3 ± 11.7 |
67.4 ± 11.8 |
0.415 |
|
Gender (Male) |
299 (58.9%) |
91 (65.9%) |
0.132 |
|
Height (cm) |
168.4 ± 9.7 |
169.7 ± 13.3 |
0.215 |
|
Weight (kg) |
82.3 ± 17.0 |
82.3 ± 20.2 |
0.987 |
|
BMI |
29.0 ± 5.3 |
30.2 ± 5.9 |
0.340 |
|
Non-smoker |
245 (48.2%) |
56 (40.6%) |
0.110 |
|
Diabetes mellitus |
85 (16.7%) |
25 (18.1%) |
0.701 |
|
Hypertension |
320 (63.0%) |
68 (49.3%) |
0.003 |
|
COPD |
70 (13.8%) |
19 (13.8%) |
0.997 |
|
Neurological disease |
25 (5%) |
14 (10.1%) |
0.020 |
|
13 |
10 |
|
|
12 |
4 |
|
|
Dialysis |
5 (0.98%) |
1 (0.72%) |
0.778 |
|
Previous myocardial infarction |
19 (3.7%) |
5 (3.6%) |
0.949 |
|
Atrial fibrillation |
18 |
5 |
0.964 |
|
LVEF <30% (n, %) |
23 (4.5%) |
3 (2.2%) |
0.097 |
|
LVEF: Left Ventricular Ejection Fractio |
|||
There were a significantly greater proportion of hypertensive patients in the FS group (P = 0.003). There were a significantly greater proportion of patients with neurological disease in the MiAVR group (P = 0.020). A propensity matching analysis resulted in 128 well-matched pairs with no significant differences in baseline characteristics (Table 2).
|
Table 2. Baseline characteristics of FS and MiAVR groups after propensity score matching. |
|||
|
Variables |
FS (n = 128) |
MiAVR (n = 128) |
P-value |
|
Age |
67.9 ± 11.2 |
67.9 ± 11.3 |
0.996 |
|
Gender (Male) |
76 (59.4%) |
81 (63.3%) |
0.521 |
|
Height (cm) |
169.1 ± 9.0 |
169.8 ± 10.6 |
0.585 |
|
Weight (kg) |
80.8 ± 17.0 |
80.6 ± 18.4 |
0.926 |
|
BMI |
28.8 ± 5.2 |
27.8 ± 5.4 |
0.599 |
|
Non-smoker |
55 (43.0%) |
55 (43.0%) |
1.000 |
|
Diabetes mellitus |
24 (18.8%) |
22 (17.2%) |
0.745 |
|
Hypertension |
63 (49.2%) |
64 (50.0%) |
0.901 |
|
COPD |
18 (14.1%) |
18 (14.1%) |
1.000 |
|
Neurological disease |
7 (5.5%) |
10 (7.8%) |
0.451 |
|
Dialysis |
0 (0%) |
0 (0%) |
|
|
Previous myocardial infarction |
5 (3.9%) |
4 (3.1%) |
0.734 |
|
Atrial fibrillation |
4 (3.1%) |
5 (3.9%) |
0.734 |
|
LVEF <30% (n, %) |
2 (1.6%) |
3 (2.3%) |
0.652 |
MiAVR versus FS study outcomes
The unmatched comparison of outcomes (Table 3) demonstrates a significantly prolonged CPB time (80.3 ± 31.2 vs 107.3 ± 25.7, P < 0.001) and aortic cross-clamp time (60.5 ± 24.9 vs 82.9 ± 22.3, P < 0.001) in the MiAVR group. There were no significant differences in any major post-operative complications. However, in the FS group there was an increased incidence in mortality rates (1.2% vs 0%, P = 0.199); post-operative arrhythmias (44.9% vs 42%, P = 0.566) and post-operative hospital stay (8.0 ± 6.3 vs 7.3 ± 5.1, P = 0.218). Indications for re-operation in the FS group include surgical debridement for deep sternal infections (n = 2) and bleeding/tamponade (n = 21). Indications for re-operation in the MiAVR group include surgical debridement (n = 1) and bleeding/tamponade (n = 4). All re-operations for the MiAVR cohort were for mini-sternotomy patients.
|
Table 3. Outcomes for FS and MiAVR groups prior to propensity score matching. |
|||
|
Outcomes |
FS (n = 508) |
MiAVR (n = 138) |
P-value |
|
Mortality |
6 (1.2%) |
0 |
0.199 |
|
Stroke |
29 (5.7%) |
7 (5.1%) |
0.540 |
|
Re-operation |
23 (4.5%) |
5 (3.6%) |
0.707 |
|
Post-operative arrhythmias |
228 (44.9%) |
58 (42%) |
0.566 |
|
Superficial Sternal infection |
12 (2.4%) |
4 (2.9%) |
0.879 |
|
Deep Sternal infection |
7 (1.4%) |
4 (2.9%) |
0.221 |
|
UTI |
11 (2.2%) |
6 (4.3%) |
0.156 |
|
Septicaemia |
4 (0.8%) |
0 |
0.296 |
|
Post-operative hospital stay (days) |
8.0 ± 6.3 |
7.3 ± 5.1 |
0.218 |
|
Cardiopulmonary bypass time (minutes) |
80.3 ± 31.2 |
107.3 ± 25.7 |
<0.001 |
|
Aortic cross-clamping time (minutes) |
60.5 ± 24.9 |
82.9 ± 22.3 |
<0.001 |
The propensity matched cohorts (Table 4) showed aortic cross-clamping time (61.80 ± 27.48 vs 84.27 ± 24.24, P < 0.001) and CPB time (81.65 ± 34.12 vs 109.15 ± 28.55, P < 0.001) was significantly prolonged in the MiAVR group. FS group tends to have a greater post-operative hospital stay, however, no significant difference was observed (8.32 ± 6.34 vs 7.21 ± 5.08, P = 0.125). Similar results between the two groups were seen in mortality rates, post-operative arrhythmias, post-operative stroke, superficial sternal infections, deep sternal infections, re-operative and septicaemia rates.
|
Table 4. Outcomes for FS and MiAVR groups after propensity score matching. |
|||
|
Outcomes |
FS (n = 128) |
MiAVR (n = 128) |
P-value |
|
Mortality |
1 (0.8%) |
0 |
0.316 |
|
Stroke |
6 (4.7%) |
6 (4.7%) |
1.000 |
|
Re-operation |
5 (3.9%) |
4 (3.1%) |
0.740 |
|
Post-operative arrhythmias |
52 (40.6%) |
56 (43.8%) |
0.613 |
|
Superficial Sternal infection |
4 (3.1%) |
3 (2.3%) |
0.702 |
|
Deep Sternal infection |
2 (1.6%) |
4 (3.1%) |
0.409 |
|
UTI |
2 (1.6%) |
5 (3.9%) |
0.250 |
|
Septicaemia |
0 |
0 |
|
|
Post-operative hospital stay (days) |
8.3 ± 6.3 |
7.2 ± 5.1 |
0.125 |
|
Cardiopulmonary bypass time (minutes) |
81.7 ± 34.1 |
109.2 ± 28.6 |
<0.001 |
|
Aortic cross-clamping time (minutes) |
61.8 ± 27.5 |
84.3 ± 24.2 |
<0.001 |
Pre-operative CT imaging
Of the 138 patients who underwent a MiAVR procedure, 77 pre-operative CT images were available (Table 5). The average distance between the second intercostal space and the aortic valve was 110.9mm. 85.7% of patients (n = 66) met the criteria for intercoastal space to aortic valve distance. 76.7% of patients (n = 59) met the criteria for the rightward position of the aorta. 90.9% of patients (n = 70) met the minimum aortic valve annulus diameter. Overall, 70.1% of patients (n = 54) satisfied the three requirements for a right anterior mini-thoracotomy.
|
Table 5. Pre-operative CT imaging results for right anterior mini-thoracotomy |
|
|
Criteria |
Number of patients (n = 77) |
|
Distance from second intercostal space to aortic valve < 120mm |
66 (85.7%) |
|
Rightward ascending aorta with respect to the right sternal border |
59 (76.7%) |
|
Minimum aortic valve annulus diameter > 20mm |
70 (90.9%) |
|
Total number of patients eligible for right anterior mini-thoracotomy |
54 (70.1%) |
Discussion
Since Harkens first description of a successful AVR, significant advancements in surgical technique have been made. A meta-analysis of randomized trials demonstrated the safety and feasibility of MiAVR when compared to FS but failed to register any significant advantages particularly in operative data, post-operative outcomes and early mortality (8). Currently, MiAVR is recognized as a suitable alternative to FS though current debate remains regarding the superior technique.
In the present study, comparison of outcomes between FS and MiAVR in propensity-matched and unmatched cohorts illustrates a significantly increased CPB and aortic cross-clamp times during a MiAVR procedure. The association between MiAVR and an increased CPB time is a comprehensive finding akin to several other papers who exhibit a similar pattern (15). Moreover, the 27.50-minute average difference in CPB time appears to be a greater increase in comparison to similar studies who report a more modest 13 (16) or 11.50-minute difference (10).
The correlation between prolonged CPB times and an increase in morbidity and mortality is well documented (17) and suggested to result in a systemic inflammatory response syndrome which in turn manifests into organ dysfunction (18). A prospective observational study raised appropriate concern regarding the direct relationship between increased CPB time and the incidence of surgical site infections (9). In our study the rates of infective complications, namely superficial and deep sternal infections, UTI and septicaemia showed insignificant differences.
Traversing the learning curve of novel MiAVR techniques is a factor apportioned to the increased CPB and aortic cross-clamp times. However, despite an increase in these intraoperative factors, several publications note that there was no increased incidence of adverse outcomes during this early period of the learning curve (19). This may reflect careful patient selection. In fact, a small increase in effect was observed towards the end as the surgeon accepted higher risk patients. Ultimately, despite an increase in CPB and aortic cross-clamp times apportioned to the reduced intraoperative field and initial learning curve, there were no significant adverse outcomes observed in MiAVR procedures.
Akin to CPB, prolonged aortic cross-clamp times have been highlighted as an independent risk factor for a spectrum of post-operative cardiovascular complications such as stroke, acute renal failure and low cardiac output (20). Whilst no difference in stroke incidences were seen in either cohort, the latter two outcomes were unfortunately not investigated in our study. The same paper observed a concomitant increase in mechanical ventilation times and hospital stay, neither of which were found in our study.
Nonetheless, a speculated increase in morbidity risk of 1.4% per 1 minute increase of aortic cross-clamp time warrants consideration (21). Reasons for this correlation are thought to reside in the intrinsic ischaemic injury reflected by aortic cross-clamping and that despite improved myocardial protection, it is still noted to affect morbidity and mortality (22). Given our study did not record incidences of acute renal failure or low cardiac output, it is difficult to conclusively determine that prolonged aortic cross-clamp times has no detrimental impact on cardiovascular complications. However, the lack of significant difference in stroke, mortality and arrhythmia rates between FS and MiAVR cohorts implies that perhaps the protracted aortic cross-clamp time may not be clinically relevant.
By avoiding unnecessary lower mediastinal dissection, MiAVR approach reduces blood loss. These results are synonymous with a meta-analysis who report markedly lower incidence of red blood cell transfusion (46.6% vs 63.5%, P < 0.001) and decreased post-operative blood loss in MiAVR patients (23). The improved preservation of the thoracic cage and sternal stability which implies an accelerated return to mobility has been proposed to reduce hospital stay (24), however, this did not materialise into a significant finding in our study. The lack of a significant finding when compared to other publications may reside in the heterogenicity in hospital stay reporting. Other analyses consider the total length of hospitalisation or intensive care unit (ICU) stay (23). We did not consider ICU stay in this study as this could be influenced by the availability of ICU beds at the time of operation.
No differences in re-operation rates were observed in our study. While it would be expected that re-operative rates would be reduced in MiAVR due the minimal dissection and sternal interference, other studies also report equal re-operative rates for FS and MiAVR (25).
Key anatomical factors deemed integral to determining the eligibility of a patient for a right anterior mini-thoracotomy include: aortic valve annulus size; distance from the second intercostal space to the aortic valve and the rightward position of the ascending aorta with respect to the right sternal border (13, 14). Patients with a small aortic valve annulus have been associated with an increased procedure complexity hence a larger annulus size is desirable for MiAVR (14). The distance from the second intercostal space to the aortic valve annulus is integral to determining the ease of the valve procedure itself (14). Additionally, the rightward position of the aorta provides information for the site of aortic cannulation (13, 14). Consequently, patient selection for a right anterior mini-thoracotomy is based off two key parameters: working distances to the aortic valve and central arterial cannulation sites.
Of the 138 MiAVR patients, only 77 pre-operative CT scans were available. Transfer of images from an alternative hospital and migration of images onto Sectra PACS are possible reasons for this. Nonetheless, 70.1% of these patients satisfied all three requirements for right anterior mini-thoracotomy. Given this large proportion of patients, the results from our study support the notion to offer right anterior mini-thoracotomies to patients. Whilst this study highlights potential anatomical challenges, these anatomical exclusion criteria should be interpreted flexibly with surgeons experience and institutional practice also taken into consideration.
Off the basis of the findings in our study, it is premature to consider MiAVR as a superior technique to FS considering the lack of long-term evaluation of MiAVR outcomes. Additionally, it is unknown which MiAVR technique is the optimal approach. Implementation of sutureless valves in MiAVR may be a promising solution to reducing aortic cross-clamp and CPB times though there is a lack of large cohort prospective studies to confirm this (13). The intra-operative and early post-operative findings of this study demonstrate promising results that are comparable to FS. Analysis of the long-term outcomes of MiAVR with supplementary evidence of the benefits of sutureless valves are required before considering the superiority of MiAVR.
Study Limitations
The generalizability of this study is limited as a retrospective analysis at a single-centre with patient data collected from a database thus a multi-centre study is required. There may be some potential confounding variables which could not be accounted for such as the learning curve of each surgeon. Additionally, covariate matching was limited to the available variables and was decided in accordance with similar studies. With respect to the CT imaging analysis, only a single rater performed the measurements. Introducing multiple raters to validate results would increase the robustness of these measurements.
Conclusion
MiAVR is a safe and effective approach for patients undergoing an isolated aortic valve replacement. MiAVR, which was predominantly performed by mini-sternotomy, boasts incidences of mortality and post-operative complications comparable to FS. Despite the prolonged CPB and aortic cross-clamp times in comparison to FS, there were no detrimental clinical outcomes observed. Evaluation of pre-operative CT images demonstrates that a substantial proportion of MiAVR patients satisfy the anatomical criteria required for a right anterior mini-thoracotomy procedure but a surgeon’s experience and institutional practice should also be considered during clinical decision making. A prospective randomized clinical trial is required to confirm our findings and evaluate the long-term outcomes following MiAVR procedures.
Acknowledgements
I would like to thank Mr Ahmed and Dr Lee for their continued support and overall lead in the project.
Data Availability
Anonymized data from this study maybe available to the scientific community subject to appropriate ethical approval. Requests for data should be directed to the senior author.
Conflict of interest: none declared.
References
1. Rodríguez-Caulo EA, Guijarro-Contreras A, Guzón A, Otero-Forero J, Mataró MJ, Sánchez-Espín G, et al. Quality of Life After Ministernotomy Versus Full Sternotomy Aortic Valve Replacement. Semin Thorac Cardiovasc Surg. 2021;33(2):328-34.
2. Lee BY, Gleason TG, Sonnad SS. Quality of life after aortic valve replacement. Expert Review of Pharmacoeconomics & Outcomes Research. 2004;4(3):265-75.
3. Tabata M, Umakanthan R, Cohn LH, Bolman III RM, Shekar PS, Chen FY, et al. Early and late outcomes of 1000 minimally invasive aortic valve operations. European journal of cardio-thoracic surgery. 2008;33(4):537-41.
4. Rao PN, Kumar AS. Aortic valve replacement through right thoracotomy. Texas Heart Institute Journal. 1993;20(4):307.
5. Cosgrove DM, Sabik JF. Minimally invasive approach for aortic valve operations. The Annals of thoracic surgery. 1996;62(2):596-7.
6. Liu J, Sidiropoulos A, Konertz W. Minimally invasive aortic valve replacement (AVR) compared to standard AVR. European Journal of Cardio-Thoracic Surgery. 1999;16(Supplement_2):S80-S3.
7. Boix-Garibo R, Uzzaman MM, Bapat V. Review of Minimally Invasive Aortic Valve Surgery. Interventional Cardiology Review 2015;10(3):144–8. 2015.
8. Brown ML, McKellar SH, Sundt TM, Schaff HV. Ministernotomy versus conventional sternotomy for aortic valve replacement: a systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2009;137(3):670-9.e5.
9. Jamil DD, Baram A, Saqat BH. Impact of prolonged cardiopulmonary bypass and operative exposure time on the incidence of surgical site infections in patients undergoing open heart surgery: Single center case series. International Journal of Surgery Open. 2020;22:52-6.
10. Brown JM, O'Brien SM, Wu C, Sikora JA, Griffith BP, Gammie JS. Isolated aortic valve replacement in North America comprising 108,687 patients in 10 years: changes in risks, valve types, and outcomes in the Society of Thoracic Surgeons National Database. J Thorac Cardiovasc Surg. 2009;137(1):82-90.
11. Sharony R, Grossi EA, Saunders PC, Schwartz CF, Ribakove GH, Baumann FG, et al. Propensity score analysis of a six-year experience with minimally invasive isolated aortic valve replacement. The Journal of heart valve disease. 2004;13(6):887-93.
12. Bakir I, Casselman FP, Wellens F, Jeanmart H, De Geest R, Degrieck I, et al. Minimally invasive versus standard approach aortic valve replacement: a study in 506 patients. The Annals of thoracic surgery. 2006;81(5):1599-604.
13. Glauber M, Ferrarini M, Miceli A. Minimally invasive aortic valve surgery: state of the art and future directions. Ann Cardiothorac Surg. 2015;4(1):26-32.
14. Tavakoli R, Leprince P, Gassmann M, Jamshidi P, Yamani N, Amour J, et al. Technique and Patient Selection Criteria of Right Anterior Mini-Thoracotomy for Minimal Access Aortic Valve Replacement. J Vis Exp. 2018(133).
15. Johnston DR, Atik FA, Rajeswaran J, Blackstone EH, Nowicki ER, Sabik III JF, et al. Outcomes of less invasive J-incision approach to aortic valve surgery. The Journal of thoracic and cardiovascular surgery. 2012;144(4):852-8. e3.
16. Gilmanov D, Bevilacqua S, Murzi M, Cerillo AG, Gasbarri T, Kallushi E, et al. Minimally invasive and conventional aortic valve replacement: a propensity score analysis. Ann Thorac Surg. 2013;96(3):837-43.
17. Calderon J, Richebe P, Guibaud JP, Coiffic A, Branchard O, Asselineau J, et al. Prospective randomized study of early pulmonary evaluation of patients scheduled for aortic valve surgery performed by ministernotomy or total median sternotomy. Journal of cardiothoracic and vascular anesthesia. 2009;23(6):795-801.
18. Wan S, LeClerc J-L, Vincent J-L. Inflammatory response to cardiopulmonary bypass: mechanisms involved and possible therapeutic strategies. Chest. 1997;112(3):676-92.
19. Taylor M, Low J, Apparau D, Mehta V, Venkateswaran R. Traversing the Learning Curve Associated with a New Minimal Access Aortic Valve Replacement Service. Braz J Cardiovasc Surg. 2021;36(5):648-55.
20. Al-Sarraf N, Thalib L, Hughes A, Houlihan M, Tolan M, Young V, et al. Cross-clamp time is an independent predictor of mortality and morbidity in low- and high-risk cardiac patients. Int J Surg. 2011;9(1):104-9.
21. Ranucci M, Frigiola A, Menicanti L, Castelvecchio S, de Vincentiis C, Pistuddi V. Aortic cross-clamp time, new prostheses, and outcome in aortic valve replacement. J Heart Valve Dis. 2012;21(6):732-9.
22. Doenst T, Borger MA, Weisel RD, Yau TM, Maganti M, Rao V. Relation between aortic cross-clamp time and mortality—not as straightforward as expected. European journal of cardio-thoracic surgery. 2008;33(4):660-5.
23. Murtuza B, Pepper JR, DeL Stanbridge R, Jones C, Rao C, Darzi A, et al. Minimal access aortic valve replacement: is it worth it? The Annals of thoracic surgery. 2008;85(3):1121-31.
24. Phan K, Xie A, Tsai Y-C, Black D, Di Eusanio M, Yan TD. Ministernotomy or minithoracotomy for minimally invasive aortic valve replacement: a Bayesian network meta-analysis. Annals of Cardiothoracic Surgery. 2014;4(1):3-14.
25. Phan K, Xie A, Di Eusanio M, Yan TD. A Meta-Analysis of Minimally Invasive Versus Conventional Sternotomy for Aortic Valve Replacement. The Annals of Thoracic Surgery. 2014;98(4):1499-511.
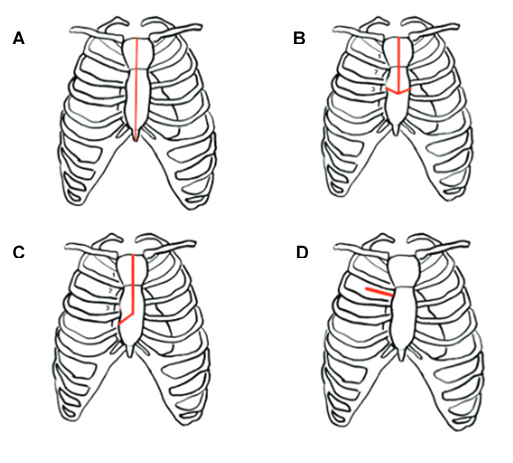
Figure 1
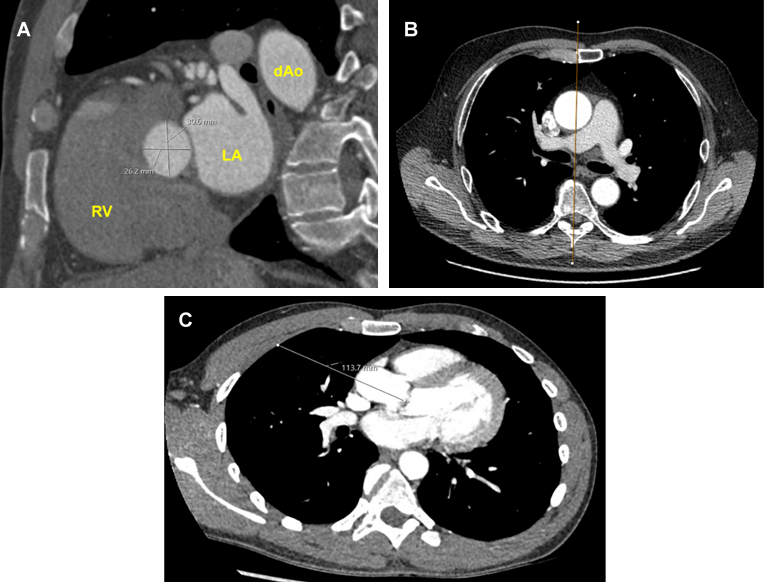
Figure 2