Redo Triple-Valve Surgery with Bypass Graft and Pacemaker Implantation Thirty-Five Years after Tetralogy of Fallot Repair
Redo Triple-Valve Surgery with Bypass Graft and Pacemaker Implantation Thirty-Five Years after Tetralogy of Fallot Repair
Anitha Chandrasekhar1*, Firdooz Ahmad Mir2, Sudipto Bannerjee3, Anil Bhan 4
1,2,3,4. Medanta-The Medicity, Gurugram, Haryana, India.
Correspondence to: Anitha Chandrasekhar, Medanta, Gurugram, Haryana, India.
Copyright
© 2025 Anitha Chandrasekhar. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 Mar 2025
Published: 14 July 2025
Abstract:
Surgery for Tetralogy of Fallot (TOF) is among the most common pediatric cardiac surgical procedures with excellent long-term survival rates. The combination of multiple pathologies in this condition makes it more susceptible to a spectrum of sequelae as increasing numbers of patients reach adulthood. Significant focus remains on issues related to the right ventricular outflow tract (RVOT) during follow-up after TOF repair. However, compelling evidence suggests that many patients also present with aortic dilatation, which may or may not necessitate re-intervention. We present the case of a sixty-two-year-old gentleman with TOF who developed triple valve regurgitation three and a half decades after a complete correction procedure, requiring intervention for all three valves along with bypass grafting and pacemaker implantation. A thorough understanding of the pathophysiology of aortic dilation following TOF repair would assist in developing appropriate management strategies. Follow-up care for these patients should concentrate not only on the RVOT but also on careful measurements of the aortic root and ascending aortic sizes to prevent catastrophic complications.
KEYWORDS: Tetralogy of Fallot, Aortic dilatation, Aortopathy, Pulmonary regurgitation, Tricuspid regurgitation.
Redo Triple-Valve Surgery with Bypass Graft and Pacemaker Implantation Thirty-Five Years after Tetralogy of Fallot Repair
Introduction
Tetralogy of Fallot (TOF) is the most common cyanotic congenital heart disease, with survival into adulthood being common.1 Long-term complications following TOF correction include right ventricular outflow tract issues, pulmonary valve problems, and aortic pathologies such as valve regurgitation and aortic dilatation.2 While the follow-up care for patients with TOF typically emphasizes the right ventricular outflow tract and pulmonary valve, recent evidence highlights a growing concern regarding aortic issues. Many patients are presenting with aortopathy, which is linked to the disease's inherent characteristic of right-to-left blood shunting. Contrary to the popular belief that aortic root dilatation in patients with TOF is primarily the result of chronic volume overload, evidence suggests that the aortic size does not stabilize even after the repair of the defect. Thus, a deeper understanding of the physiology of aortic dilatation in this patient subset is warranted to help plan appropriate treatment strategies.
Case Report
We report the case of a 62-year-old gentleman who presented with triple valve regurgitation and single-vessel coronary artery disease, requiring complex redo surgery three and a half decades after TOF repair.
History
The patient underwent a left-sided Blalock-Taussig (BT) shunt at the age of 8 and total correction of TOF with ventricular septal defect closure, take-down of BT shunt, infundibular resection, and transannular autologous pericardial patch augmentation of the RVOT at 27 years. He was regularly followed up and was doing well for the first two decades after surgery but was lost to follow-up thereafter.
Presentation
He presented recently with angina, breathlessness on exertion, palpitation, and three episodes of Syncope. Echocardiography revealed moderate to severe aortic regurgitation (AR), severe pulmonary regurgitation (Free PR), severe tricuspid regurgitation (TR), normal left ventricular function, borderline right ventricular function, intact ventricular septal defect (VSD) patch, and no residual VSD. He was in first-degree atrioventricular block with bifascicular block. Computed Tomography (CT) of the Chest exhibited a dilated aortic root and ascending aorta with a maximum transverse ascending aortic dimension of 5.36 cm and heavy calcium in the distal ascending aorta and base of the innominate artery (Figures 1,2,3). Marked cardiomegaly, biatrial, and left ventricular enlargement with a calcified aortic valve were also noted. Coronary Angiography demonstrated single-vessel coronary artery disease with a tight lesion in the right coronary artery (RCA), and normal left anterior descending (LAD) and left circumflex (LCX) arteries (Figure 4). The rest of his pre-operative investigations, including carotid Doppler and peripheral Doppler study, were unremarkable.
Figure 1: Sagittal view of CT thorax showing a layer of calcium lining the aortic wall in the ascending aorta and arch of the aorta, with dilated aortic root and dilated ascending aorta.
Figure 2: Axial cross-section view of CT Thorax revealing a maximum transverse diameter of the ascending aorta of 5.36 cm.
Figure 3: Coronal CT section showing cardiomegaly, biatrial and left ventricular enlargement with calcified aortic valve.
Figure 4: Coronary Angiogram stills showing normal left anterior descending artery (LAD), normal left circumflex artery (LCX), and long segment lesion in the distal right coronary artery. The stainless steel sternal wires used to approximate the sternum during the previous surgery are seen under fluoroscopy. (a) The picture shows that LAD is a Type III vessel with proximal irregularities and a normal, non-dominant LCX. (b) Dominant RCA, Distal RCA has tubular 90% stenosis, recanalized with bridging collaterals.
Surgery
After obtaining high-risk written informed consent and pre-operative anesthesia clearance, the patient was taken for surgery. He was initially scheduled for a complex major redo surgical procedure- Bentall’s procedure/ Aortic valve replacement, Pulmonary Valve implantation, and Tricuspid valve repair, along with Coronary artery bypass grafting. The axillary artery was exposed and cannulated to establish cardiopulmonary bypass. This approach was effective for the redo procedure, preventing cannulation of the calcified ascending aorta. Safe sternal re-entry was achieved. However, there were dense pericardial adhesions that needed to be dissected out. The aortic root, ascending aorta, and main pulmonary artery looked plastered with layers of tissue. The ascending aorta was calcified. To attempt a root replacement appeared to be a risky proposition. Given that the aortic dimension was less than 5.5 cm, the decision was made on-table to proceed with only the aortic valve replacement, rather than root replacement, to simplify the complex surgical procedure. Cardiopulmonary bypass was instituted using axillary artery-bicaval cannulation. The patient underwent aortic and pulmonary valve replacement using a 27mm aortic bioprosthesis (for both), modified De Vega’s Tricuspid annuloplasty, along with a reversed saphenous vein graft to the distal RCA. Valve implantations were done in the standard fashion according to the institutional protocol and surgeon’s preference, using multiple, interrupted, non-pledgetted, simple braided sutures. The procedure was uneventful. The patient was weaned off cardiopulmonary bypass uneventfully with good hemodynamics and sinus rhythm. Post-procedure transesophageal echocardiography was satisfactory, revealing normally functioning bioprosthetic valves, no valvular/paravalvular leak, adequately repaired tricuspid valve, and left ventricular dysfunction with ejection fraction of 35%.
Post-operative course
The patient had a relatively smooth course in the intensive care unit (ICU) post-operatively. He was extubated on the first postoperative day and had an uneventful stay in the ICU. However, he developed Tachycardia-Bradycardia Syndrome later, for which Holter monitoring was done, which indicated multiple long pauses. Given the previous history of syncope, dual-chamber permanent pacemaker implantation was done. The patient recovered well with slow and steady improvement in ventricular function and was discharged in stable condition with anti-coagulants, anti-platelets, diuretics, and pain relief medications. The patient was counseled about the need for close follow-up and meticulous CT evaluation of the ascending aortic diameter.
Discussion
Long-term outcomes of TOF repair have been excellent, with reported 30-year survival of 68.5% to 90.5%.3 However, re-operations may be indicated in a certain subset of patients with pulmonary valve issues, aortic pathologies, or any residual sequelae. The various problems that can occur late after TOF repair are listed in Table 1. Any of these factors, or a combination of them, could require a re-intervention, which may carry high risks associated with the redo surgical procedure and comorbidities. Our patient in the case study displayed many of the mentioned issues, including PR, TR, aortic dilatation, arrhythmias, and impaired cardiopulmonary performance.
Table 1: Late problems after TOF repair. The sequelae after surgery for TOF could potentially require re-interventions in the long term. Abbreviations: TOF- Tetralogy of Fallot, PR- Pulmonary Regurgitation, TR- Tricuspid Regurgitation, RVOTO- Right Ventricular Outflow Tract Obstruction, VSD- Ventricular Septal Defect
The aortic pathologies in this patient subset seem to be due to a combination of factors, including intrinsic aortic wall abnormalities, chronic right-to-left shunting of blood leading to aortic volume overloading, and histological alterations with advancing age as TOF repair patients reach adulthood.4 Many studies have identified risk factors for aortic root dilatation post-TOF repair. The longer the interval between shunt and repair, the greater the risk of developing a dilated aorta. Also, in patients with pulmonary atresia or severe pulmonary stenosis, the risk of developing an aortic aneurysm later in life is high. The various risk factors identified from a multitude of studies are listed in Table 2. However, the literature does not have a consensus on a cut-off aortic diameter at the time of corrective surgery that could predict a future aortic dilatation, considering that the aorta is usually bigger to start with, in these patients.
Table 2: Risk factors for aortic dilatation. Compiled from Cruz et al.5, Dimitrakakis et al.6, Egbe et al.7
Many studies have been conducted to elucidate whether TOF repair in infancy could prevent the problem of aortic dilatation. Bhat et al postulated that if TOF correction is staged within one year of age, the aortic dimensions could be stabilized and normalized within seven years.8 A combination of physiological, histopathological, and embryological factors could form the etiological component of aortic dilatation in TOF patients. The various variables that could be involved are summarized in Table 3. In addition to the logical volume overload, other histological factors like medial necrosis, medial degeneration, and extracellular matrix destruction play a major role.
Table 3: Variables causing aortic dilation. Adapted from Ramapabhu et al.9 and Vida et al.10
Seki et al postulated that aortic wall stiffness could be a prognostic indicator of aortic dilatation.11 They measured the wall stiffness using pulse wave velocity in 32 TOF correction procedure patients. Another parameter that was found to be more strongly associated with aortic dilatation is the aortic strain on magnetic resonance imaging.12
The risk of aortic dissection in this patient subset is lower than the conventional aortopathy syndrome patients, though isolated case reports have been published.13 Anecdotal case reports of aortic root dilatation of 8.8 cm at the Sinus of Valsalva have been published, but with no dissection.14 This patient was reported to be asymptomatic, and the aortic aneurysm was detected during a routine pre-employment health check. Historically, the cut-off for aortic replacement has been 4.5 cm in Marfan’s, Ehlers-Danlos, Loeys-Deitz, Turner, and bicuspid aortic valve syndromes. However, it has been recommended that in the absence of a family history of aortic dissection or aneurysm, a rapidly expanding aneurysm (1 cm/year) or progressive aortic insufficiency, aortic root replacement in adults with repaired TOF is not indicated until the aortic size exceeds 5.5 cm.4 The various co-morbidities, patient risk factors, expected longevity, and the risk of perioperative and long-term complications linked with surgical procedures need to be taken into consideration while deciding on aortic interventions. Hence, our on-table decision not to go for a Bentall’s procedure with an aortic dimension of 5.36 cm and to safely perform an aortic valve replacement along with the other valvular and coronary interventions is justified.
Conclusion
Lifelong follow-up is mandatory after TOF repair, not only for pulmonary valve issues but also to screen the ascending aorta, aortic root, and aortic valve. Aortic dilatation could be linked to factors that increase the exposure of the proximal aorta to volume overload, such as late corrective surgery, palliative shunt, and residual VSD, which need to be meticulously monitored. In case a re-operation is required, a well-planned redo surgery at an advanced cardiac surgical center, with careful attention to individual components combined with efficient and diligent post-operative care yields good results.
KEY POINTS
1. Aortic dilatation post-TOF repair is an established entity.
2. Follow-up care for patients with TOF should consider the RVOT and the size of the aorta.
3. The current guideline for aortic surgery following a TOF repair recommends surgical intervention when aortic dilatation exceeds 5.5 cm, although this recommendation is subject to individual patient co-morbidities and other relevant factors.
References
1. Van der Linde D, Konings EE, Slager MA, et al. Birth prevalence of congenital heart disease worldwide: A systematic review and meta-analysis. J Am Coll Cardiol. 2011; 58(21):2241–7. Doi:10.1016/j.jacc.2011.08.025
2. D?u?niewska N, Podolec P, Skubera M, et al. Long-term follow-up in adults after tetral- ogy of Fallot repair. Cardiovasc Ultrasound. 2018; 16(1):28. Doi:10.1186/ s12947-018-0146-7
3. Van der Ven JPG, Van den Bosch E, Bogers AJCC, Helbing WA. Current outcomes and treatment of tetralogy of Fallot. F1000Res. 2019; 8:F1000 Faculty Rev-1530. Doi:10.12688/f1000research.17174.1
4. Nagy CD, Alejo DE, Corretti MC, et al. Tetralogy of Fallot and Aortic Root Dilation: A Long-Term Outlook. Pediatric Cardiology 2012; 34(4):809–816. Doi:10.1007/ s00246-012-0537-8
5. Cruz C, Pinho T, Ribeiro V, Dias CC, Silva Cardoso J, Maciel MJ. Aortic dilatation after tetralogy of Fallot repair: A ghost from the past or a problem in the future? Rev Port Cardiol. 2018; 37(7):549-557. Doi:10.1016/j.repc.2017.10.014
6. Dimitrakakis G, Oppell UV, Bosanquet D, Wilson D, Luckraz H. Aortic aneurysm forma- tion five decades after tetralogy of Fallot repair. Ann Thorac Surg 2009, 88:1000-1001. Doi:10.1016/j.athoracsur.2009.02.029
7. Egbe AC, Miranda WR, Ammash NM, et al. Aortic disease and interventions in adults with tetralogy of Fallot. Heart. 2019; 105(12):926-931. Doi:10.1136/ heartjnl-2018-314115
8. Bhat AH, Smith CJ, Hawker RE. Late aortic root dilatation in tetralogy of Fallot may be prevented by early repair in infancy. Pediatr Cardiol. 2004; 25:654–9. Doi:10.1007/ s00246-003-0665-2
9. Ramaprabhu K, Idhrees M and Velayudhan B. Aortopathy in Tetralogy of Fallot—a col- lective review. Indian Journal of Thoracic and Cardiovascular Surgery 2019. Doi:10.1007/s12055-019-00791-5
10. Vida VL, Triglia LT, Zanotto L, et al. Late management of the aortic root after repair of tetralogy of Fallot: A European multicentre study. J Card Surg. 2020; 35(1):40-47. Doi: 10.1111/jocs.14316
11. Seki M, Kurishima C, Saiki H, et al. Progressive aortic dilation and aortic stiffness in children with repaired tetralogy of Fallot. Heart Vessel. 2014;29:83–7. Doi:10.1007/ s00380-013-0326-1
12. Grotenhuis HB, Dallaire F, Verpalen IM, van den Akker MJE, Mertens L, Friedberg MK. Aortic Root Dilatation and Aortic-Related Complications in Children After Tetralogy of Fallot Repair. Circ Cardiovasc Imaging. 2018; 11(12):e007611. Doi:10.1161/ CIRCIMAGING.118.007611
13. Rathi VK, Doyle M, Williams RB, Yamrozik J, Shannon RP, Biederman RWW. Massive aortic aneurysm and dissection in repaired Tetralogy of Fallot; diagnosis by cardiovas- cular magnetic resonance imaging. Int J Cardiol 2005, 101:169-170. Doi: 10.1016/j.ij- card.2004.05.037.
14. Nishimura Y, Yasutsune T, Shimajiri S, et al. Significant delayed aortic dilatation after tetralogy of Fallot repair: a case report. Surg Case Rep. 2020; 6(1):173. Doi:10.1186/ s40792-020-00935-5

Figure 1
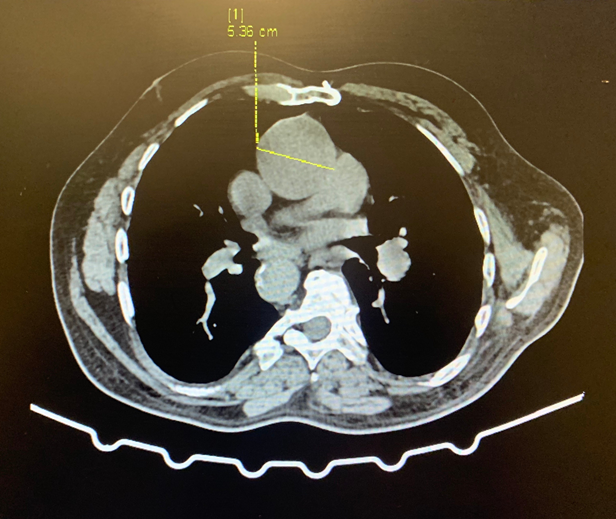
Figure 2
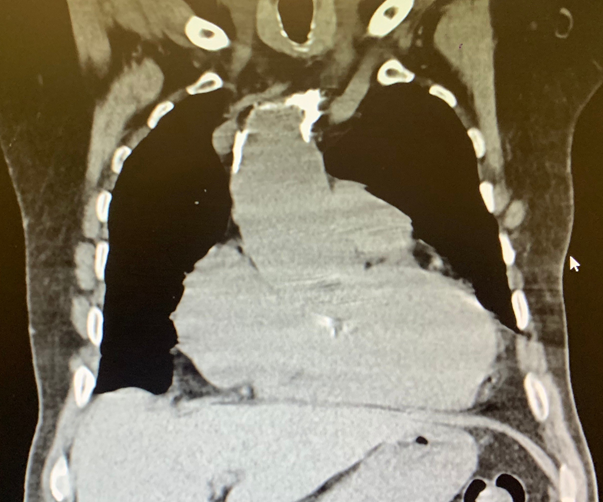
Figure 3
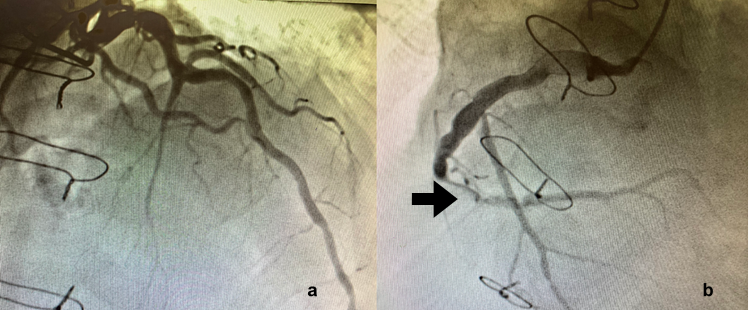
Figure 4
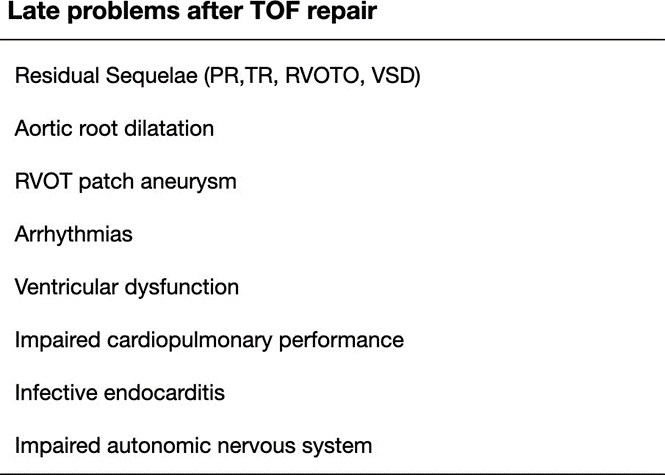
Figure 5
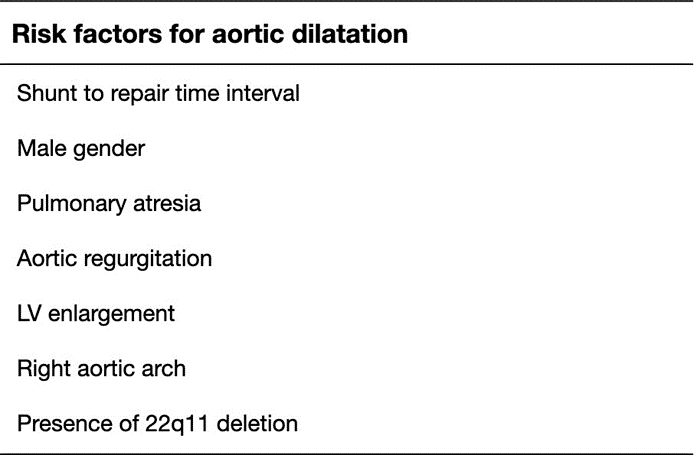
Figure 6
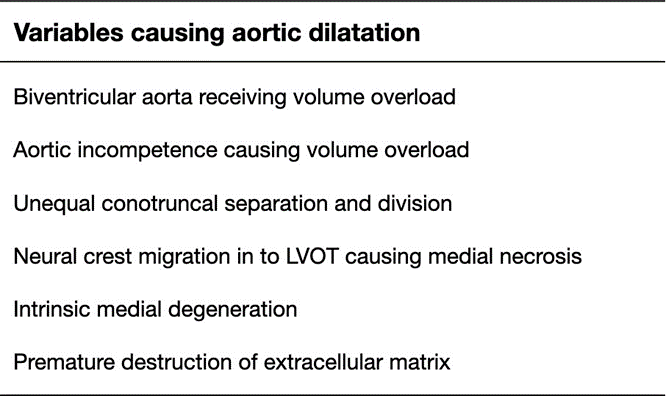
Figure 7