The Role of Defocus Lenses in Controlling Axial Elongation in Myopia: A Review
The Role of Defocus Lenses in Controlling Axial Elongation in Myopia: A Review
Dr. Rupali *
*Correspondence to: Dr Rupali Consultant Optom Pediatric and Binocular Vision at Save Sight Centre, M.optom F.optom B.optom Certified FDP In CVI And Seizure Care Perkins U.S.A
Copyright
© 2025 Dr. Rupali. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 June 2025
Published: 17 July 2025
Abstract:
The global prevalence of myopia, particularly among children and adolescents, has risen sharply over recent decades, posing a significant public health concern. The condition is primarily driven by excessive axial elongation, which increases the risk of vision-threatening ocular pathologies later in life. Among emerging interventions, optical treatments utilizing defocus principles—especially those that impose peripheral myopic defocus—have demonstrated considerable potential in slowing axial elongation and myopia progression. This review provides an overview of the biological basis of myopia, the mechanism by which defocus lenses operate, and current evidence from clinical trials involving Defocus Incorporated Multiple Segments (DIMS) spectacle lenses and multifocal soft contact lenses. The paper also evaluates their efficacy, safety, and long-term potential as a non-invasive treatment strategy for myopia control.
The Role of Defocus Lenses in Controlling Axial Elongation in Myopia: A Review
1. Introduction
Myopia is a growing global epidemic. By 2050, it is estimated that nearly 50% of the world population will be myopic, with up to 10% having high myopia [1]. High myopia (≤ -6.00 D) is associated with increased risks of irreversible visual impairment due to complications such as retinal detachment, myopic macular degeneration, and glaucoma [2,3]. Excessive axial elongation of the eyeball is a primary structural feature of progressive myopia and serves as a predictor of long-term visual prognosis [4]. Therefore, controlling axial elongation has become central to modern myopia management strategies.
Among various interventions, optical strategies such as defocus lenses that manipulate retinal image quality to alter ocular growth have received considerable attention. This review discusses the theoretical foundation, types, and clinical effectiveness of defocus lenses, with emphasis on Defocus Incorporated Multiple Segments (DIMS) and center-distance multifocal soft contact lenses.
2. Background: Mechanisms of Myopia and Axial Elongation
The process of emmetropization enables the eye to adjust its axial length in response to defocus signals during early development [5]. Inappropriate retinal image defocus, especially peripheral hyperopic defocus, may drive axial elongation and myopia progression [6]. Experimental studies in animal models have consistently shown that the eye grows in response to hyperopic defocus and that myopic defocus suppresses ocular elongation [7,8].
These principles have translated into clinical strategies aimed at manipulating peripheral retinal defocus to inhibit abnormal ocular growth. Specifically, defocus lens technologies aim to provide clear central vision while simultaneously imposing myopic defocus peripherally, thus signaling the retina to decelerate axial elongation [9].
Figure 1
3. Optical Defocus Lenses for Myopia Control
3.1 Defocus Incorporated Multiple Segments (DIMS) Lenses
The DIMS spectacle lens, developed by Hong Kong Polytechnic University, has a central 9 mm optical zone for distance correction and an annular zone embedded with multiple myopic defocus segments of +3.50 D [10]. This configuration provides constant peripheral myopic defocus irrespective of gaze direction.
A pivotal 2-year randomized clinical trial by Lam et al. found that DIMS lenses reduced myopia progression by 59% and axial elongation by 60% compared to single-vision lenses [10]. A 3-year follow-up confirmed sustained efficacy without adverse effects [11]. DIMS lenses have since been validated in multiple populations, including Chinese, Japanese, and European children [12,13].
Figure 2
3.2 Stellest™ lenses
Stellest™ lenses by Essilor company are innovative spectacle lenses developed by Essilor for myopia control in children. They incorporate H.A.L.T. (Highly Aspherical Lenslet Target) technology, which features a central clear zone for sharp vision surrounded by concentric rings of aspherical lenslets that create a myopic defocus signal. This optical design aims to slow the elongation of the eyeball (axial length), a key factor in myopia progression.
Clinical studies have demonstrated that over a two-year period, children wearing Stellest™ lenses experienced approximately a 67% reduction in myopia progression compared to those wearing conventional single-vision lenses. Additionally, axial elongation, which is closely associated with the worsening of myopia, was reduced by about 60%, indicating that these lenses can significantly slow the structural changes in the eye that drive myopia progression. Importantly, this was achieved without compromising visual clarity or comfort, making Stellest™ lenses a promising option for myopia control in pediatric patients [14].
3.3 Multifocal Soft Contact Lenses
Center-distance multifocal soft contact lenses (e.g., MiSight 1 Day, Biofinity Multifocal) contain concentric treatment zones that create peripheral myopic defocus while preserving central vision [15]. The MiSight lens, in particular, is FDA-approved for myopia control in children aged 8–12 years [16].
The BLINK study compared single-vision lenses to multifocal lenses with +1.50 D and +2.50 D additions. After 3 years, the +2.50 D group had 43% less myopia progression and 38% less axial elongation than the control group [17]. Other studies, such as the DISC study in Hong Kong, reported a 25% reduction in axial elongation over 2 years with bifocal contact lenses [18].
4. Comparative Effectiveness and Outcomes
A comparison of key studies is shown below:
|
Lens Type |
Myopia Progression Reduction |
Axial Elongation Reduction |
|---|---|---|
|
DIMS Spectacle Lenses [10] |
~59% |
~60% |
|
Stellest Spectacle Lenses [14] |
~67% |
~60% |
|
MiSight Soft Lenses [16] |
~50–60% |
~50% |
|
BLINK Trial (+2.50 D) [18] |
~43% |
~38% |
These outcomes suggest that defocus lenses significantly reduce both refractive progression and axial elongation in children. Compliance, early initiation, and consistent wear are critical to maximizing these benefits [19].
5. Limitations and Challenges
While defocus lenses are effective, inter-individual variability exists. Some children may not respond adequately, and predictive biomarkers are lacking [20]. Treatment efficacy is also influenced by compliance, baseline refractive error, ethnicity, and time spent outdoors [21].
Furthermore, long-term rebound effects after cessation of lens wear are not fully understood. Although DIMS lenses have shown sustained effects over 3 years [11], longer follow-up is required. Additionally, multifocal contact lenses carry risks of infection and require strict hygiene practices, which can be challenging in pediatric populations [22].
Cost and accessibility may also hinder widespread adoption, particularly in low-resource settings. Future research should focus on combining optical therapies with pharmacological agents like low-dose atropine to enhance outcomes [23].
6. Future Directions
Emerging technologies include extended-depth-of-focus (EDOF) lenses, spectacle lenses with gradient power profiles, and AI-powered smart lenses that adjust focus dynamically [24]. Personalized treatment algorithms based on biometric data and environmental exposure may soon allow clinicians to tailor interventions with greater precision.
Combining multiple treatment modalities, including behavioral strategies such as increased outdoor time, may further amplify treatment success [25]. Digital tools for monitoring lens wear compliance and axial growth in real time are also under development [26].
7. Conclusion
Defocus lenses represent a well-established, non-pharmacological approach for controlling myopia progression, primarily by targeting and slowing axial elongation. Clinical trials consistently demonstrate significant reductions in both refractive error progression and axial length increase when using optical interventions such as DIMS spectacle lenses, Stellest™ lenses, and center-distance multifocal soft contact lenses. Notably, DIMS lenses have shown up to 60% reduction in axial elongation over three years, while Stellest™ lenses have achieved up to 67% reduction in myopia progression. MiSight and other multifocal contact lenses also yield substantial benefits, albeit with varying efficacy based on lens design and patient compliance.
Despite the promising results, individual variability in response, dependency on adherence, and potential barriers related to cost and access remain challenges. There is a need for long-term data to assess sustained benefits and any rebound effects post-treatment cessation. Future directions, including the integration of digital compliance monitoring, AI-driven personalization, and combination therapies (e.g., with low-dose atropine), may enhance the overall effectiveness of myopia control programs.
In summary, defocus lenses are a clinically validated, safe, and increasingly accessible modality in pediatric myopia management. Their use, when combined with early intervention and supportive lifestyle strategies like increased outdoor activity, holds significant promise for reducing the global burden of myopia-related visual impairment.
References
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036-42.
2. Wong TY, Ferreira A, Hughes R, et al. Epidemiology and burden of pathologic myopia and myopic choroidal neovascularization: An evidence-based systematic review. Am J Ophthalmol. 2014;157(1):9-25.
3. Jonas JB, Ohno-Matsui K, Panda-Jonas S. Myopia: anatomic changes and consequences for its etiology. Asia Pac J Ophthalmol. 2019;8(5):355-359.
4. Tideman JW, Snabel MC, Tedja MS, et al. Association of axial length with risk of uncorrectable visual impairment for Europeans with myopia. JAMA Ophthalmol. 2016;134(12):1355-63.
5. Mutti DO, Mitchell GL, Sinnott LT, et al. Corneal and crystalline lens dimensions before and after myopia onset. Optom Vis Sci. 2012;89(3):251-62.
6. Smith EL, Hung LF, Huang J. Relative peripheral hyperopic defocus alters central refractive development in infant monkeys. Vision Res. 2009;49(19):2386–2392.
7. Wallman J, Winawer J. Homeostasis of eye growth and the question of myopia. Neuron. 2004;43(4):447–68.
8. Wildsoet CF. Active emmetropization—evidence for its existence and ramifications for clinical practice. Ophthalmic Physiol Opt. 1997;17(4):279-90.
9. Sankaridurg P, Holden B, Smith E, et al. Decreasing the global burden of myopia by delaying the onset of myopia and reducing progression: a review. Investig Ophthalmol Vis Sci. 2012;53(11):6449-53.
10. Lam CSY, Tang WC, Tse DY, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomized clinical trial. Br J Ophthalmol. 2019;104(3):363-368.
11. Tang WC, Lam CSY, et al. Three-year clinical trial of DIMS spectacle lenses for myopia control. Ophthalmic Physiol Opt. 2021;41(5):1203-1210.
12. Bao J, Yang A, Huang Y, et al. One-year myopia control efficacy of spectacle lenses with aspherical lenslets. Br J Ophthalmol. 2022;106(8):1110-4.
13. Mori K, Hasebe S, et al. Effectiveness of DIMS lenses in Japanese children: a 1-year study. Clin Ophthalmol. 2021;15:1701–1709.
14. Bao, J., Huang, Y., Li, X., Yang, A., Zhou, F., Wu, J., Wang, C., Li, Y., Lim, E.W., Spiegel, D.P. and Drobe, B., 2022. Spectacle lenses with aspherical lenslets for myopia control vs single-vision spectacle lenses: a randomized clinical trial. JAMA ophthalmology, 140(5), pp.472-478.
15. Anstice NS, Phillips JR. Effect of dual-focus soft contact lens wear on axial myopia progression in children. Ophthalmology. 2011;118(6):1152-1161.
16. CooperVision. MiSight 1 Day: Clinical Trial Report. [Internet]. Available: https://coopervision.com
17. Walline JJ, Walker MK, Mutti DO, et al. Effect of high add power, medium add power, or single-vision contact lenses on myopia progression in children: the BLINK randomized clinical trial. JAMA. 2020;324(6):571-580.
18. Lam CSY, Tang WC, Tse DY, et al. Randomized clinical trial of contact lens with peripheral defocus to control myopia progression. Ophthalmology. 2014;121(11):2248-2255.
19. Chamberlain P, Peixoto-de-Matos SC, Logan NS, et al. Myopia control with MiSight 1 day lenses: 4-year results. Optom Vis Sci. 2019;96(8):556-567.
20. Brennan NA, Touboul J, Cheng X, et al. Efficacy in myopia control: meta-analysis and guidance for interpreting differences between devices. Ophthalmic Physiol Opt. 2022;42(3):403–416.
21. French AN, Ashby RS, Morgan IG, et al. Time outdoors and the prevention of myopia. Exp Eye Res. 2013;114:58-68.
22. Matsumura H, Hirai H. Prevalence of myopia and refractive changes in students from 3 to 17 years of age. Surv Ophthalmol. 1999;44:S109–S115.
23. Chia A, Lu QS, Tan D. Five-year clinical trial on atropine for the treatment of myopia 2: Myopia control with atropine 0.01% eyedrops. Ophthalmology. 2016;123(2):391-399.
24. Ruiz-Pomeda A, Villa-Collar C, et al. Myopia control with corneal reshaping contact lenses in Spanish children: a 2-year clinical trial. Eye Contact Lens. 2018;44(1):58-63.
25. Wu PC, Chen CT, Lin KK, et al. Myopia prevention and outdoor light intensity in a school-based cluster randomized trial. Ophthalmology. 2020;127(8):1029-1037.
26. Yang Z, Lan W, et al. The impact of digital screen time on myopia: a meta-analysis. Int J Ophthalmol. 2020;13(8):1337-1345..
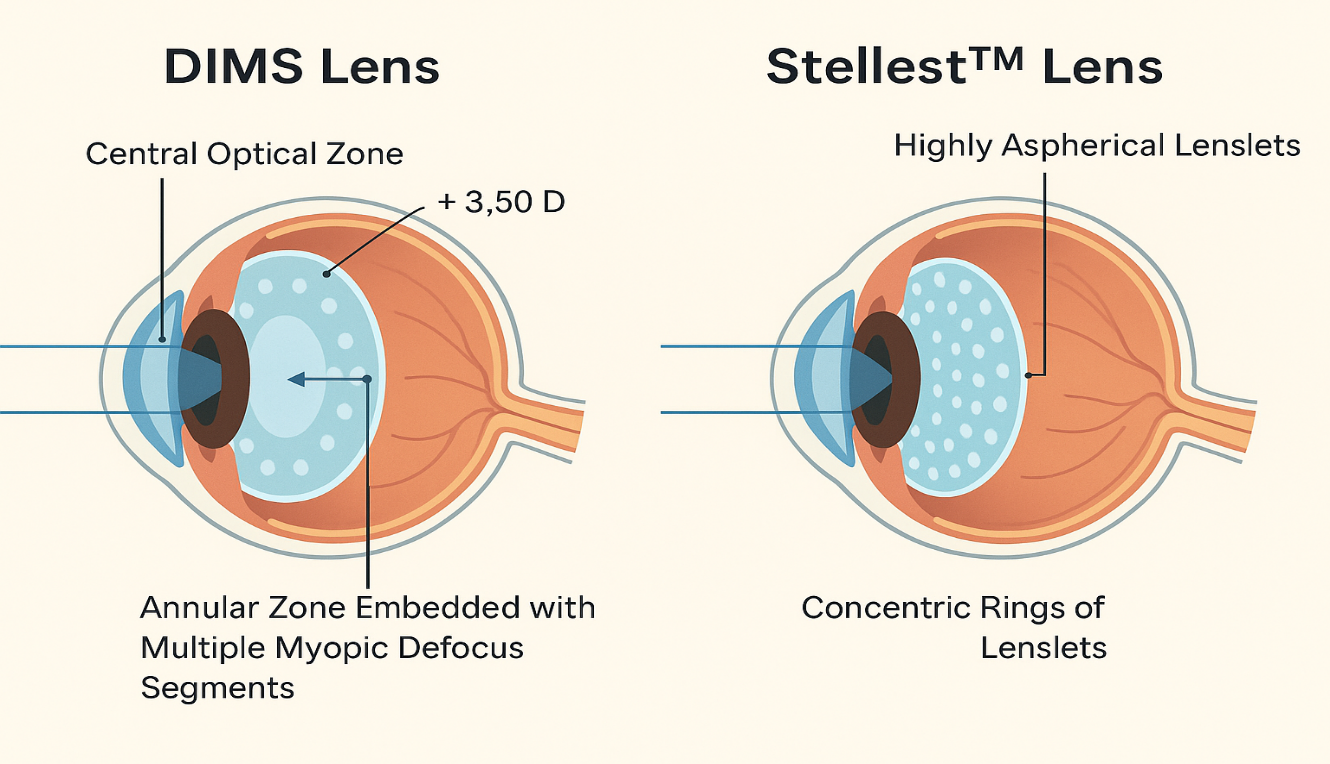
Figure 1
Figure 2