Horseshoe Appendix, A rare congenital anomaly: Case Report and Literature Review
Horseshoe Appendix, A rare congenital anomaly: Case Report and Literature Review
Khadidja Amedjoudj *
*Correspondence to: Khadidja Amedjoudj, Department of pediatric surgery, specialized hospital of mother and child Bachir Bennacer, Eloued, Algeria.
Copyright.
© 2025 Khadidja Amedjoudj This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 July 2025
Published: 19 July 2025
DOI:https://doi.org/10.5281/zenodo.16302970
Abstract
The horseshoe appendix is the rarest subtype of appendix duplication, with only 19 cases reported worldwide to date. We describe a case of 5-year-old boy who was diagnosed with acute appendicitis by clinical examination and ultrasound. Intraoperatively, we discovered a horseshoe appendix with two bases, communicating both with the cecum, appendectomy was safely performed. In this report we provide a literature review, with discussion of the clinical features, diagnosis, and surgical approach of this rare congenital anomaly.
Keywords: Horseshoe appendix, Appendix duplication, Acute appendicitis, Congenital malformation.
Horseshoe Appendix, A rare congenital anomaly: Case Report and Literature Review
Introduction
Appendix duplication is a rare congenital anomaly with an estimated incidence of 0.004 to 0.009% in separate studies 1. Various types of this malformation have been described and classified according to Cave-Wallbridge classification system. Among these variants, the horseshoe shaped appendix represents the rarest and the most recently described form.
In this paper we report a case of horseshoe appendix encountered during surgery for acute appendicitis and we also provide a focused review of the existing literature on this exceptionally rare entity.
Case Presentation
A 5-year-old boy presented to the emergency department (ED) with a 4 days history of abdominal pain, vomiting and fever, he was initially evaluated by a general Practitioner, misdiagnosed as gastroenteritis and treated with antibiotics. Over the 48hours preceding his arrival to the ED his abdominal pain has increased with persistent fever. On physical examination, the patient exhibited significant tenderness in the right iliac fossa (RIF), local guarding and rebound tenderness were elicited at McBurney's point Blood tests revealed a marked leukocytosis with a white blood cell count of 22,000/μL, predominantly neutrophils. The C-reactive protein (CRP) level was also elevated.
Abdominal US revealed a thickened appendix to 14mm with reactive free fluid in the abdomen.
Based on the clinical presentation, physical examination findings, laboratory results, and imaging, the diagnosis of acute appendicitis was made. We decided to proceed with an open appendectomy intraoperatively; the appendix was found to be tightly adherent to the cecum. After careful dissection, an anatomical anomaly was discovered: two distinct appendiceal stumps were identified, positioned frontally on the cecum (Fig-1). These stumps were noted to be communicating with each other and shared a central mesoappendix (Fig-2). A small quantity of reactive free fluid was also present in the peritoneal cavity. An appendectomy was performed, involving the ligation of both identified appendiceal bases. The patient had an uncomplicated postoperative recovery. He was discharged home on the fourth postoperative day. Subsequent follow-up was uneventful.
Histopathological examination of the resected specimen confirmed the structure as a true appendiceal tissue originating from and inserting into the cecum at two points, and revealed features of suppurative appendicitis, confirming inflammation within the horseshoe appendix (Fig-3).
Fig-1, 2,3
Discussion
Appendix duplication is an extremely rare congenital anomaly, less than 100 cases have been documented in the medical literature, with fewer than 15 cases complicated by acute appendicitis 2.
The classification of appendiceal duplication was first proposed by Cave in 1936 3 and later modified by Wallbridge in 1962 4, creating what is now known as the Cave-Wallbridge classification system. This system was further expanded by Bierman in 1993 to include additional variants 5.
In 2010, Calota et al added the horseshoe shape to the old classification 6
The classification includes:
Type A: A single cecum with various degrees of incomplete appendiceal duplication.
This represents partial duplication of the appendix.
Type B: A normal appendix arising from the cecum with a second appendix. This type is further subdivided into:
- Type B1 (avian-type): The second appendix arises symmetrically from the opposite side of the ileocecal valve, resembling the arrangement seen in birds.
- Type B2 (taenia coli type): The second appendix arises anywhere along the lines of the taenia coli, and this is the most commonly reported type.
Type B3: The second appendix arises from the hepatic flexure.
Type B4: The second appendix arises from the splenic flexure.
Type C: Duplication of the cecum, each containing an appendix.
Type D: A horseshoe appendix with two openings into a single cecum.
With Frontal disposal (Fig-4)
With Sagittal disposal (Fig-5)
Fig-4: Frontal disposal
Fig-5: Sagittal disposal
Our case represents a Type D duplication, the limited number of horseshoe appendix cases reported since its first description by Mesko et al in 1989 7, makes it extremely rare with an estimated incidence far lower than the overall 0.004% reported for all duplications
Reviewing the literature; only nineteen cases of horseshoe appendix have been reported to date 8–11, across various age groups and geographic locations. Our case represents the twentieth case and it hasn’t been reported before in Algeria to our knowledge. While often associated with appendicitis 8,9,11, as in the presented case, they have also been found incidentally or in association with other conditions like bowel obstruction, appendicular mass, lymphoma, or colonic adenoma12,13 The anatomical configuration typically involves both bases inserting into the cecum (cecum-cecum), although variations like cecum-hepatic flexure or cecum-ascending colon have been described 14
The embryological origin of the horseshoe appendix remains speculative. Proposed theories include the fusion of two initially separate appendicular buds, the development of fistula between the tip of appendix and the cecum connecting them together, or an anomaly in the division of the mesoappendix, possibly linked to a single supplying blood vessel 15. None of these theories have been definitively proven.
The presence of associated congenital anomalies varies with the type of appendiceal duplication. Type B1 and Type C duplications are frequently associated with other anomalies, including duplications or anomalies of the gastrointestinal tract, genitourinary tract, vertebral anomalies, and hindgut duplications 2,12. Type D duplication, is not typically associated with other congenital anomalies9. This is consistent with our patient, who had no evidence of additional anomalies on clinical examination or imaging studies.
The significant challenge associated with horseshoe appendix is its preoperative diagnosis. As demonstrated in the presented case and corroborated by literature, standard imaging modalities like ultrasound and CT scans often fail to identify the duplication, typically showing only signs of appendicitis if present8–11,15–19 . Liu et al reported successful preoperative diagnosis using ultrasound with 3D reconstruction in two cases, suggesting advanced imaging might play a role, but this is not the norm20 . Consequently, the diagnosis is most commonly made intraoperatively.
Surgeons encountering suspected appendicitis should maintain a degree of suspicion for anatomical variations, especially if the initial findings are atypical. Thorough exploration of the ileocecal region is paramount on identifying any appendiceal anomaly. For horseshoe appendix, the key management principle is the complete removal of the entire appendiceal structure along with secure closure of both cecal openings. Failure to identify and manage the second base can lead to persistent inflammation, stump appendicitis, or future diagnostic confusion. Techniques involve careful dissection, ligation of the mesoappendix often containing a single vessel, and separate ligation or stapling of both appendiceal bases. Some reports mention additional dissection of the cecum to eliminate retrocecal duplication 6
Conclusion
The rarity of Horseshoe appendix makes each case report valuable for expanding our understanding of the embryological origins, its clinical significance, management, and potential complications.
This report contributes in enriching knowledge base, and potentially aiding surgeons in recognizing and appropriately managing this rare entity.
Conflict of Interests:
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Collins, D. C. A study of 50,000 specimens of the human vermiform appendix. Surg. Gynecol. Obstet. 101, 437–445 (1955).
2. Vieira, E. de P. L., Bonato, L. M., Silva, G. G. P. da & Gurgel, J. L. Congenital abnormalities and anatomical variations of the vermiform appendix and mesoappendix. J. Coloproctology 39, 279–287 (2019).
3. Cave, A. J. Appendix Vermiformis Duplex. J. Anat. 70, 283–292 (1936).
4. Wallbridge, P. H. Double appendix. J. Br. Surg. 50, 346–347 (1962).
5. Biermann, R., Borský, D. & Gogora, M. [Double appendicitis--a rare pathologic entity]. Chir. Z. Alle Geb. Oper. Medizen 64, 1059–1061 (1993).
6. Calot?, F. et al. Horseshoe appendix: a extremely rare anomaly. Chir. Buchar. Rom. 1990 105, 271–274 (2010).
7. Mesko, T. W., Lugo, R. & Breitholtz, T. Horseshoe anomaly of the appendix: a previously undescribed entity. Surgery 106, 563–566 (1989).
8. Jabi, R., Elmir, S. & Bouziane, M. First case report of horseshoe appendix in Morocco according according to SCARE guidelines. Ann. Med. Surg. 70, 102870 (2021).
9. Roy, S., Chakraborty, P., Shaw, M. & Halder, P. Horseshoe appendix with double insertion of base: A previously unreported anomaly. J. Anat. Soc. India 72, 70 (2023).
10. Deflaoui, T. et al. Appendiceal duplication: a case report of horseshoe-shaped appendix and implications for patient safety. J. Surg. Case Rep. 2024, rjae075 (2024).
11. Pflieger, H. & Tchikladzé-mérand, C. Horseshoe appendix: A case report and literature review. Medicine (Baltimore) 104, e41425 (2025).
12. Nageswaran, H., Khan, U., Hill, F. & Maw, A. Appendiceal Duplication: A Comprehensive Review of Published Cases and Clinical Recommendations. World J. Surg. 42, 574–581 (2018).
13. Takabatake, K. et al. A case of a horseshoe appendix. Surg. Case Rep. 2, 140 (2016).
14. Dube, B., Manoharan, G. R., Daya, M. & Pillay, S. S. Anomalous origin of the vermiform appendix. S. Afr. J. Surg. 49, 100–101 (2011).
15. Singh, C. G. Horseshoe Appendix: An Extremely Rare Appendiceal Anomaly. J. Clin. Diagn. Res. (2016) doi:10.7860/JCDR/2016/16569.7494.
16. Oruc, C., Isik, O., Ureyen, O., Kahyaoglu, O. S. & Koseoglu, A. An extremely rare appendiceal anomaly: horseshoe appendicitis. Turk. J. Trauma Emerg. Surg. 19, 385–386 (2013).
17. Choi, S.-J. et al. Horseshoe appendix identified during laparoscopic appendectomy: A case report and literature review. Medicine (Baltimore) 98, e14104 (2019).
18. Serter, ?., Ero?lu, E., Akbal, E., Kesici, U. & Alt?nl?, E. Horseshoe Appendix Is an Extremely Rare Cause of Acute Appendicitis. Am. Surg. 84, e490–e491 (2018).
19. Pamak Bulut, S., Cabioglu, N. & Akinci, M. Perforated double appendicitis: Horseshoe type. Turk. J. Surg. 32, 134–136 (2016).
20. Liu J, Li D. Man xing huan zhuang lan wei yan ji xing fa zuo bing qian dun xing hui chang nei zuo yi li. Chin J Gastrointest Surg. 2012:786–7.
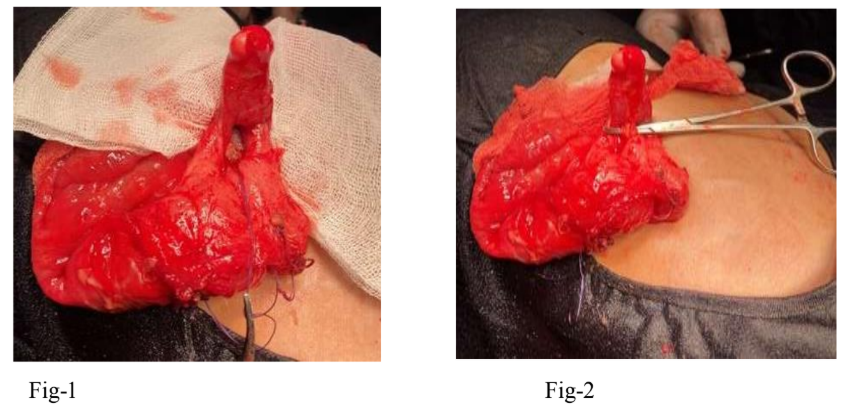
Figure 1
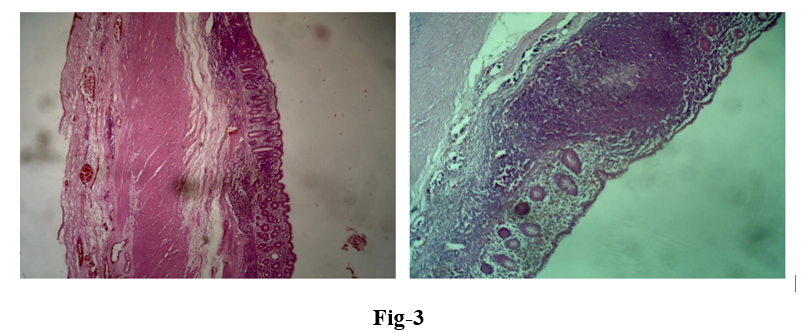
Figure 2
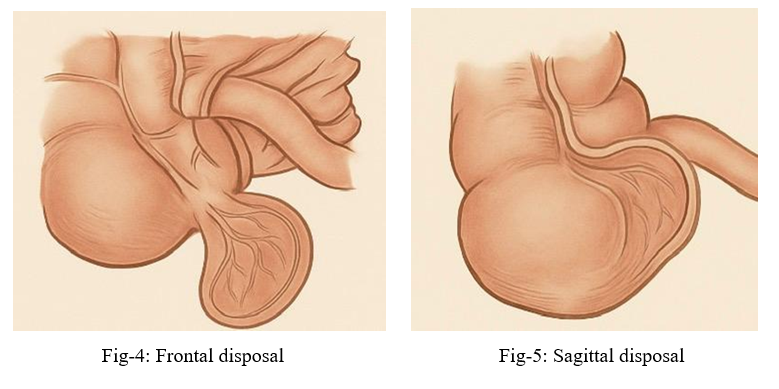
Figure 3