Colonic Stent Placement in Malignant Bowel Obstruction
Colonic Stent Placement in Malignant Bowel Obstruction
Ethan Mitchell, BS1*, Corey Mealer, BS1, Manjakkollai P. Veerabagu, MD2
1. Medical Student, College of Medicine; Medical University of South Carolina
2.Affiliate Associate Professor; Medical University of South Carolina
*Correspondence to: Ethan Mitchel, BS., Medical Student, College of Medicine; Medical University of South Carolina.
Copyright
© 2025 Ethan Mitchel, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 July 2025
Published: 23 July 2025
Abstract:
Colon Cancer is the third most common type of cancer in the United States. Bowel obstruction is a potential complication of advanced colon cancer. Surgical treatment options include temporary colostomy and later colon resection if the is resectable or permanent colostomy if the cancer is unresectable. Alternatively, colonic stent placement could avoid temporary or permanent colostomy irrespective of the resectability. Colonic stenting can serve as a bridge therapy to surgery while the patient is being medically optimized, or as palliative care in cases of unresectable or metastatic cancer1. In patients as a bridge to surgery it is associated with less morbidity and mortality2. In this article, we report a case of a 59-year-old male with metastatic colon cancer complicated by large bowel obstruction, who underwent colonic stent placement with complete relief of bowel obstruction and avoided colostomy.
Colonic Stent Placement in Malignant Bowel Obstruction
Case
The patient is a 59-year-old male who was accidentally found to have liver lesions when he underwent (CTA) computed tomography angiography for chest pain (Figure 1). A subsequent positron emission tomography scan (PET) revealed metastatic disease in the liver (Figure 2), most likely originating from the primary sigmoid colon cancer (Figure 3). CT-guided liver biopsy of the liver lesion confirmed metastatic disease with histologic features consistent with a primary of colorectal origin. His blood test showed elevated colonic embryogenic antigen (CEA) of 38 ng/ml.
The patient was referred to Oncology, chemotherapy regimen of fluorouracil, oxaliplatin, and folinic acid (FOLFOX) was started. Five months later, the patient was admitted to the hospital with signs and symptoms of colonic obstruction. Prior to this hospitalization, the patient had received 7 cycles of FOLFOX, and his CEA significantly decreased to 7.79 ng/ml. A CT scan of the abdomen showed bowel obstruction secondary to the primary malignancy of the sigmoid colon with multiple metastatic foci in the liver. After multidisciplinary team discussion, we decided the colonic stent placement would be the best option for this patient and would avoid surgical colostomy and the recovery would be quick so that chemotherapy could be resumed without much delay. Patient gladly agreed to have colonic stent placement to relieve his large bowel obstruction.
Colonic stent placement was performed under general anesthesia. The patient was placed in the left lateral decubitus position and a double channel therapeutic gastroscope (Olympus America) was passed into the rectum until an area of complete colonic obstruction was reached in the sigmoid colon. The fluoroscopy was also used in this procedure. The luminal obstruction was so severe we have to use ERCP cannula and 0.025 in angled visiglide wire (Olympus America) under fluoroscopy to access the obstructed proximal part of the dilated colon through the tumor. Then a 25 mm x 90 mm Boston Scientific colonic stent was deployed (Figure5) successfully, and stool was visualized coming through the stent from the obstructed part of the colon (Figure 6). A follow-up x-ray of the abdomen was used to confirm there was no adverse event like perforation (free air under the diaphragm).
As soon as the the stent was placed, the patient experienced multiple bowel movements. Symptoms of nausea, vomiting, abdominal distension and abdominal pain had significantly improved immediately following the stent deployment. The patient was placed on a clear liquid diet initially and advanced to regular diet and discharged home two days after the stent placement. The patient resumed his chemotherapy and was seen for follow up couple of weeks later and he was doing remarkably well eating normally and without any gastrointestinal symptoms.
Figure 1. CTA of the chest showing multiple liver metastasis
Figure 2. PET scan showing multiple Liver metastasis
Figure 3. PET scan showing primary source of malignancy in sigmoid colon
Figure 4. Malignant obstruction in the sigmoid colon prior to stent placement.
Figure 5. Initial stent deployment with passage of stool
Figure 6. Stent placement and deployment.
Figure 7. Visualization of the post-procedure stent position and patency on fluoroscopy.
Discussion
Complete large bowel obstruction is a complication that can occur with colon cancer. Screening for colon cancer in the average risk patient begins at age 45 with a colonoscopy. The above mentioned patient has never had screening colonoscopy before. The prognosis of patients with colon cancer is dependent on their stage of diagnosis, the earlier the stage the better the outcome and long term disease free survival. If a patient presents with colorectal cancer with symptoms of a bowel obstruction or presence of metastasis, they typically have poor prognosis3.
In patients with malignant large bowel obstruction, colonic stenting avoids colostomy and allows early resumption of chemotherapy4. Surgical colon resection can result in complications like anastomotic leak, need for temporary or permanent colostomy, bleeding, infection, dehiscence, injury to surrounding structures, and adhesions that can lead to future repeat bowel obstruction5. Studies have shown that colonic stents have fewer complications and are associated with shorter hospital stays and earlier resumption of chemotherapy.
Patients with malignant bowel obstructions have symptoms such as nausea, vomiting, abdominal distension, obstipation and abdominal pain. For patients with metastatic disease who may not be the best surgical candidates, it is best to give them the fastest time to relieve symptoms. Colonic stenting is a relatively safe procedure that provides this opportunity.
This report presents the case of a malignant bowel obstruction of metastatic sigmoid colon cancer that was able to be treated by colonic stent placement. This intervention gave fast relief, a quick recovery time, and resumption of regular diet, chemotherapy and avoided colostomy.
References
1. Bayraktar, B., Ozemir, I.A., Kefeli, U., Demiral, G., Sagiro?lu, J., Bayraktar, O., Adali, G., Ozcelik, A., Tortum, O.B. Colorectal stenting for palliation and as a bridge to surgery: A 5-year follow-up study. World J Gastroenterol. 2015;21(31):9373-9.
2. Sagar, J. Role of colonic stents in the management of colorectal cancers. World J Gastrointest Endosc. 2016;8(4):198-204.
3. Winner, M., Mooney, S.J., Hershman, D.L., Feingold, D.L., Allendorf, J.D., Wright, J.D., Neugut, A.I. Incidence and predictors of bowel obstruction in elderly patients with stage IV colon cancer: a population-based cohort study. JAMA Surg. 2013;148(8):715-22.
4. de Gregorio, M.A., Mainar, A., Rodriguez, J., Alfonso, E.R., Tejero, E., Herrera, M., Medrano, J., D'Agostino, H. Colon stenting: a review. Semin Intervent Radiol. 2004;21(3):205-16.
5. Kirchhoff, P., Clavien, P.A., Hahnloser, D. Complications in colorectal surgery: risk factors and preventive strategies. Patient Saf Surg. 2010;4(1):5.
6. Ohno, M.,Nishida, A., Nishino, K., Hirayama, H., Takahashi, K., Morita, Y., Kishi, Y., Morita, Y., Bamba, H., Shiomi, H., Imaeda, H. Palliative stenting for malignant colorectal stenosis in the elderly. DEN Open. 2022;3(1):e168..
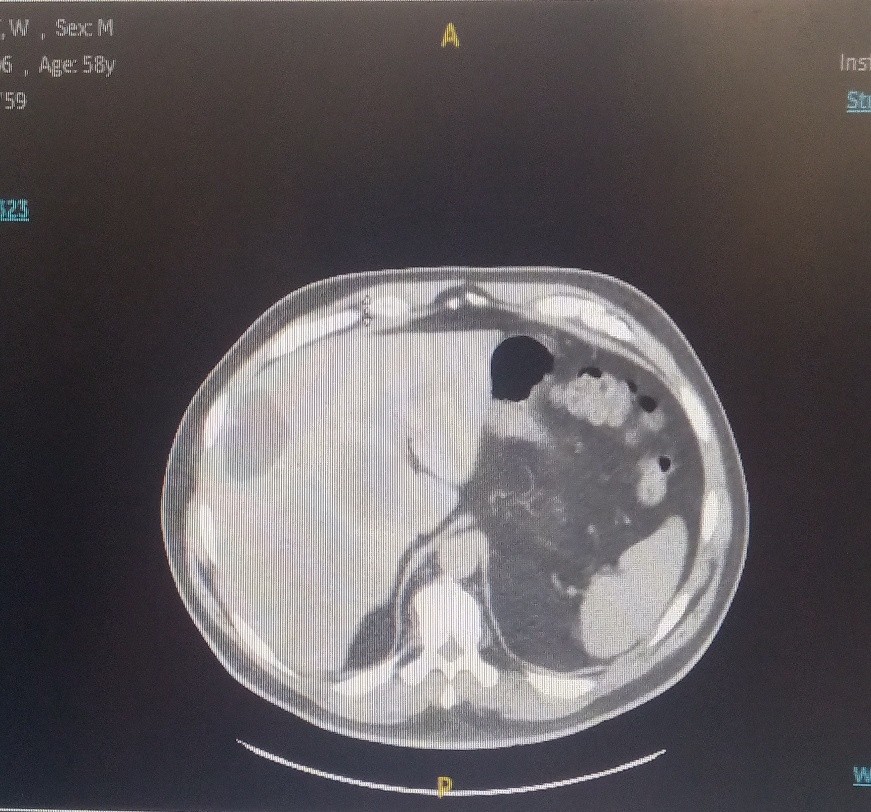
Figure 1
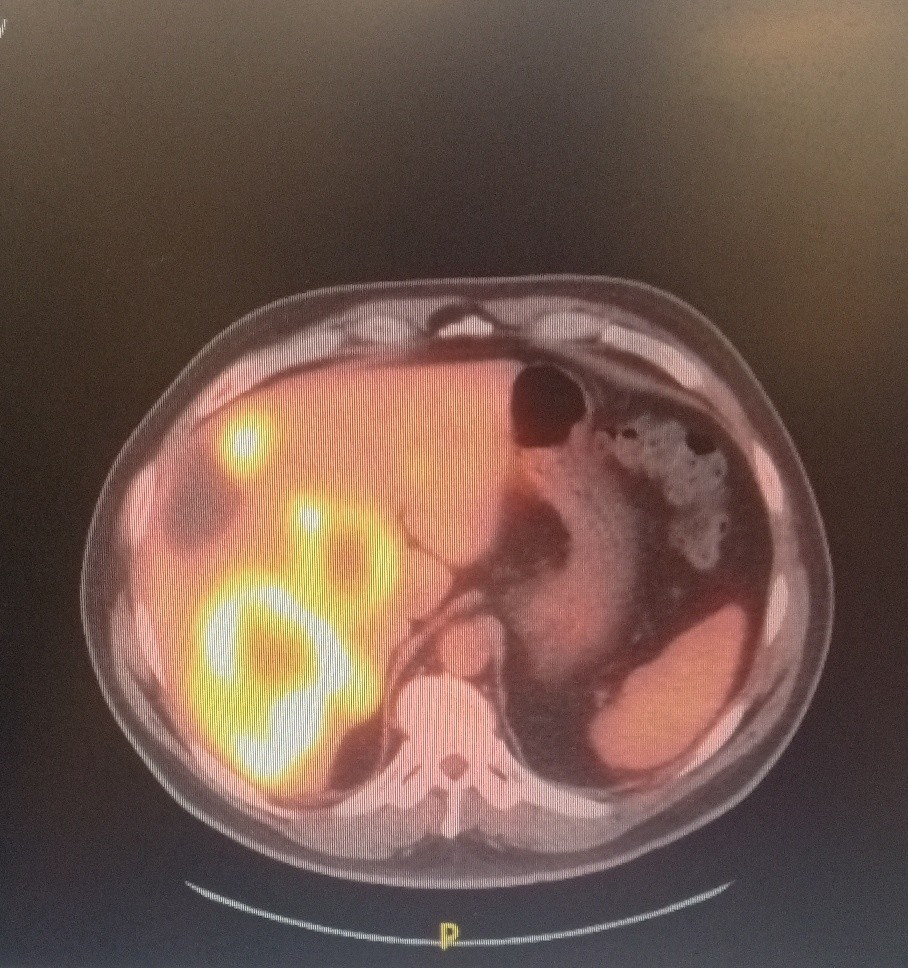
Figure 2
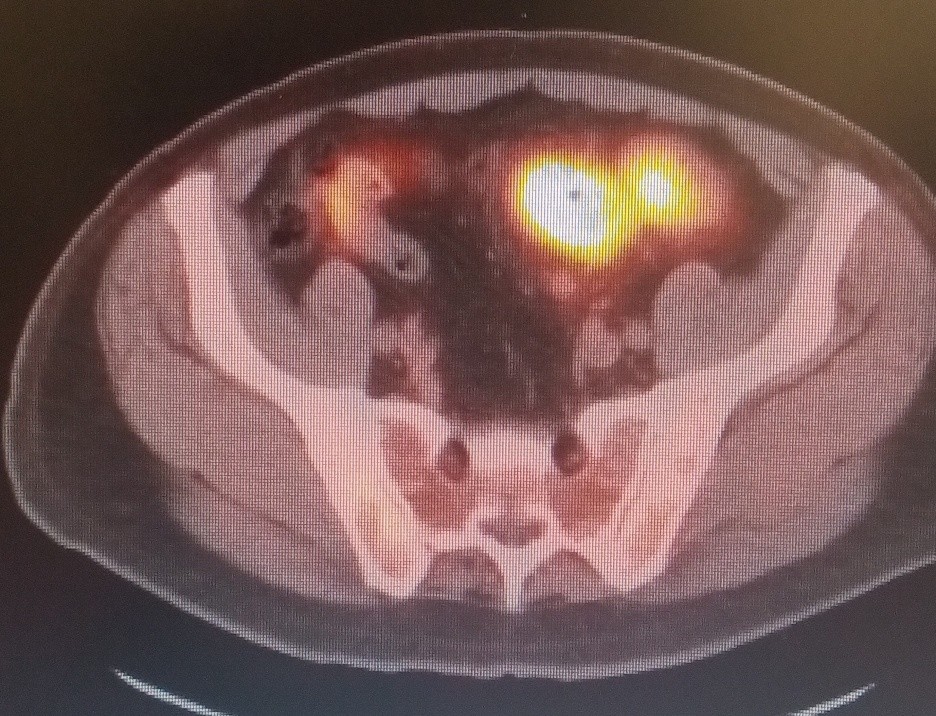
Figure 3

Figure 4
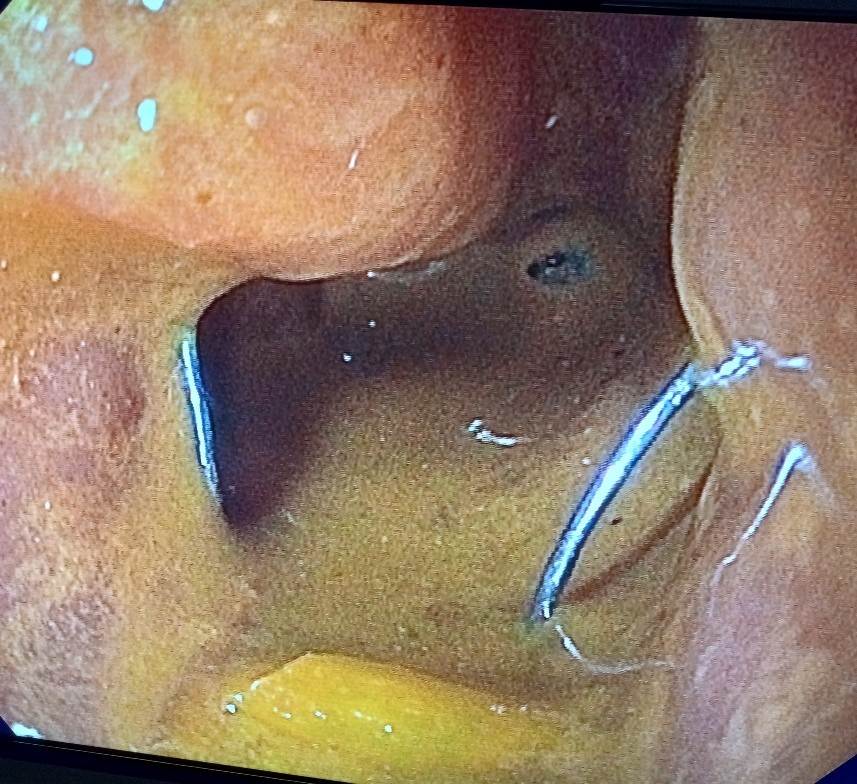
Figure 5

Figure 6

Figure 7