The correlation amongst insulin resistance indices( including TyG index, TyG-BMI,AIP, METS-IR along with results in patients with heart failure with preserved ejection fraction- A Short Communication
The correlation amongst insulin resistance indices( including TyG index, TyG-BMI,AIP, METS-IR along with results in patients with heart failure with preserved ejection fraction- A Short Communication
Dr Kulvinder Kochar Kaur *1, DR Gautam Nand Allahbadia2, Dr Mandeep Singh3
1. Dr Kulvinder Kochar Kaur, M.D (Obstt & Gynae, specialist reproductive endocrinology & Infertility specialist). Scientific Director Dr Kulvinder Kaur Centre For Human Reproduction 721,G.T.B. Nagar, Jalandhar-144001, Punjab,India.
2. Dr Gautam Nand Allahbadia M.D.(Obstt&Gynae),D.N.B, Scientific Director Ex-Rotunda-A Centre for Human Reproduction 672,Kalpak Garden,Perry Cross Road, Near Otter’s Club,Bandra(W)-400040
Mumbai, India.
3. Dr Mandeep Singh M.D.DM.(Std)(Neurology), Consultant Neurologist Swami Satyanand Hospital
Near Nawi Kachehri,Baradri, Ladowali road, Jalandhar, Punjab.
*Correspondence to: Dr Kulvinder Kochar Kaur, M.D Obstt & Gynae, specialist reproductive endocrinology & Infertility specialist, Scientific Director Dr Kulvinder Kaur Centre For Human Reproduction 721,G.T.B. Nagar, Jalandhar-144001, Punjab,India.
Orcid Number- https://orcid.org/0000-0003-1473-3419
Copyright.
© 2025 Dr Kulvinder Kochar Kaur This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 July 2025
Published: 01 Aug 2025
DOI: https://doi.org/10.5281/zenodo.16793922
Abstract
Having detailed the association amongst abdominal obesity(AO) ,type2 diabetes mellitus( T2DM), Heart failure with preserved ejection fraction (HFpEF ), and role of adipose tissue (AT) impairment with adipocytokines,role of Diabetic cardiomyopathy (DbCM) that is associated with greater HFpEF incidence,role of epigenetics, therapy inclusive of Sodium Glucose Transporter 2( SGLT 2)hampering agents, glucagon like peptide 1(GLP-1)-1 receptor agonist(GLP-1RA), as innovative mechanistic modes for the avoidance of HFpEF by utilization of GLP-1RA as innovative mechanistic modes for the avoidance of HFpEF, the countercontrolling Renin-Angiotensin system(RAS), part of escalated TG’s and diminished HDL-C in the formation of IR as well as metabolic syndrome(MetS) ,emphasized the significanceof triglyceride-glucose (TyG)index &other TyG indices for instance triglyceride-glucose body mass index (TyG-BMI) ],triglyceride-glucose waist circumference (TyG-WC), in addition to triglyceride-glucose waistto-height ratio (TyG-WHtR) marker for evaluating IR in contrast to the euglycemic-hyperinsulinaemic clamp test .Further we detailed role of TyG index as anticipator of HFpEF prognosis. Here we further detail howall indices inclusive of TyG)index, TyG-BMI, the atherogenic index of plasma (AIP), as well as the metabolic score for insulin resistance (METS-IR), might be a meaningful anticipator of HFpEF prognosis. Such observations emphasize the significance of evaluating IR indices, specifically the TyG index, in the risk evaluation as well as management approaches for HFpEF patients. Nevertheless, noticeably requirement exists to corroborate their observations of Chinese study in variable populations for guaranteeing their application along with generalization.
Key Words; Insulin resistance( IR); metabolic syndrome; HFpEF; type2 diabetes mellitus( T2DM; hypertriglyceridemia; TyG index; TyG-BMI; AIP; METS-IR
The correlation amongst insulin resistance indices( including TyG index, TyG-BMI,AIP, METS-IR along with results in patients with heart failure with preserved ejection fraction- A Short Communication
Introduction
Earlier havingdetailed the association amongst abdominal obesity(AO) ,type2 diabetes mellitus( T2DM), Heart failure with preserved ejection fraction (HFpEF ), and role of adipose tissue (AT) impairment on liberation of adipocytokines, & non coding RNA that possess a key role in the intraorgan crosstalk amongst AT & cardiovascularsystem(CVS). Adipocytokines inclusive of adiponectin,leptin,resistin,visfatin ,omentin,angiopoietin like protein, zinc—α-2glycoprotein,glypican 4,lipocalin 2,secreted frizzled – related protein(SFRP),retinol binding protein-4, TNFα ,IL-6 as well as IL-18. Additionally, Diabetic cardiomyopathy (DbCM)that as per the Framingham Heart Study men along with women which had DM possessed 2.4 as well as 5 fold greater incidence of Heart failure(HF) respectively . Patients of DM possessed greater prevalence of HF with variation from 19-26%Furthermore ,role of epigenetics inclusive of DNA methylation,histone post-translational modifications, histone acetylation, miRNAs,circRNA, lnc RNAs histonedeacetylase( HDAC)1-6; cardiac remodelling , cardiac fibrosis, cardiac hypertrophy , LV hypertrophy, modes of cell demise for instance cardiomyocyte apoptosis ,autophagy, pyroptosis and PI3K&other various signalling pathways. Recently we further updated therapy inclusive of Sodium Glucose Transporter 2( SGLT 2)hampering agents, glucagon like peptide 1(GLP-1)-1 receptor agonist(GLP-1RA), as innovative mechanistic modes for the avoidance of HFpEF by utilization of GLP-1RA. Particularly GLP-1RA in case of patients with obesity, or metabolic syndrome(MetS) or obese diabetic patients tackling the sequelae of obesity on the heart in addition to on HFpEF, the countercontrolling Renin-Angiotensin system(RAS) along with avoidance of cardiovascular injury in such a background. Lastly, GLP-1 axis is detailed in the form of anti diabetic, anti obesity along with anti cardiac remodeling pathway. Moreover, previously we have outlined part of escalated TG’s and diminished HDL-C in the formation of IR as well as MetS, &ii)emphasized the significanceof triglyceride-glucose (TyG)index &other TyG indices for instance triglyceride-glucose body mass index (TyG-BMI) ],triglyceride-glucose waist circumference (TyG-WC), in addition to triglyceride-glucose waistto-height ratio (TyG-WHtR) marker for evaluating IR in contrast to the euglycemic-hyperinsulinaemic clamp test .Further we detailed role of TyG index as anticipator of HFpEF prognosis[1-8]. Here we further detail howall TyG indices might be a meaningful anticipator of HFpEF prognosis.
Heart failure with preserved ejection fraction (HFpEF) represents a substantially prevalent, complicated, as well as,heterogeneous disorder, that has the properties of symptoms along with signs of heart failure (HF) without obvious left ventricular systolic dysfunction [9,10]. Although presently a diminishing tendency in the incidence of HF exists totally, the prevalence of HFpEF is persistently escalating , attributing to greater than 50%of newly diagnosed HF cases, with an incidence rate of about 27 cases per 10,000 person-years [11-13]. Acknowledged the restricted therapeutic avenues for HFpEF in addition to the considerable load added by its greater mortality as well as readmission rates on healthcare cost [14], it is of considerable significance to isolate patients at extensive risk dependent on modifiable clinical properties in addition to intervene on such variables to ameliorate their risks.
HFpEF commonly coexists with metabolic comorbidities, with greater than 80% of patients being overweight or obese [15], about 20-40% having diabetes, as well as greater than 40% suffering from hyperlipidemia [16].It has been corroborated that insulin resistance (IR) possesses a crucial part in the crosstalk amongst metabolic condition in addition to HFpEF [17, 18], significantly affecting cardiomyocyte working [18,19]. IR portrays a diminished sensitivity along with insulin responsiveness [20]. At present , plethora of non-insulin- dependent indices are frequently utilized in the form of surrogate markers for assessing IR. These are inclusive of the triglyceride-glucose (TyG) index, the TyG index with body mass index (TyG-BMI), the atherogenic index of plasma (AIP), as well as the metabolic score for insulin resistance (METS-IR). The TyG index is attained by calculating fasting plasma glucose (FBG) in addition to triglyceride (TG) quantities. Ideal cut-off values for the TyG index have been displayed in the form of 8.72 for males along with 8.92 for females [21, 22]. TyG-BMI is an exhaustive index that is a product of the TyG index with the BMI. The objective of index is to yield a greater exhaustive evaluation of a person’s IR status in addition to risks associated with obesity. Analogous readings for TyG-BMI have been displayed in the form of 224.59 for males along with 234.02 for females [22]. The calculation of AIP gets obtained in the form of the logarithm base 10 of the ratio of TG to high-density lipoprotein cholesterol (HDL-C). The AIP is utilized to asssess the association amongst lipid profiles as well as the risk of atherosclerosis. Despite it does not directly determine IR, greater quantities of AIP have an association with IR states. Readings varying from − 0.3 to 0.1 are correlated with low cardiovascular(CV) risk, 0.1 to 0.24 with medium CV risk, in addition to greater than 0.24 with extensive CV risk [23]. METS-IR is a scoring system that incorporates, plethora of metabolic specifications for quantfication of a person’s extent of IR. It is inclusive of pointers of FBG, BMI, TG, as well as HDL-C. A score greater than 40.16 on the METS-IR has been displayed to be associated with a significantly escalated risk of diabetes [24]. Noticeably, It is of considerable significance that at present there is no absolute extent for normal readings for such IR indices. The normal array possess the capacity of differing, based on the study population along with results of attraction . Thereby, the aforementioned thresholds need to be taken into account in the form of reference readings instead of conclusive parameters. Studies have illustrated that escalation of such indices are intricately correlated with escalated risks of all-cause mortality as well as inimical CV processes in different cardiovascular disease(CVD’s) [25, 26]. Nevertheless, the capacity of variable IR indices to anticipate all-cause mortality in addition to HF hospitalization in HFpEF patients has not been substantially evaluated, along with a head-to-head contrasting of their anticipative readings for clinical results in HFpEF is absent.
Thereby, the objective of such longitudinal cohort study was evaluation of in addition to contrasting the anticipative performance of four IR indices—i)TyG,ii) TyG-BMI, iii)AIP, as well asiv) METS-IR—for long-term results in the HFpEF population. Furthermore, they explored the conglomerative action of such indices on the present risk anticipation gadget, the Meta-Analysis Global Group in ChronicHeart Failure (MAGGIC) risk score [27].
Ni et al. [28], enrolled patients with HFpEF from January 2012 as well as and December 2023. The definitions of outcome was comprised of major adverse cardiovascular event (MACE), that incorporated all-cause mortality in addition to rehospitalization for heart failure. The plausible linear association was looked at the association amongst the IR indices along with MACE. Furthermore, to assess the conglomerative prognostic value of the TyG index, they performed exhaustive evaluation by utilization of area under the curve (AUC), the continuous net reclassification index (cNRI), as well as the integrated discrimination index (IDI).
They observed overall 8693 patients met the inclusion criteria in addition to, got included in the ultimate assessment. The average age of the patients was 70.59 ± 10.6 years, with 5045 (58.04%) being male. The Kaplan-Meier survival evaluation displayed that greater of the four IR indices was correlated with greater risk of MACE (all log-rank P < 0.05). Once considered lesser in the form of a continuous variable, the TyG index illustrated a significant correlation amongst MACE (HR 2.1, 95% CI 1.98–2.23, P < 0.001 in model 1; HR 1.81, 95% CI 1.73–1.9, P < 0.001 in model 2; HR 1.68, 95% CI 1.6–1.76, P < 0.001 in model 3). Once divided into quartiles, the highest quartile of the TyG index (Q4) was significantly correlated with MACE (HR 2.48, 95% CI 2.24–2.76, P < 0.001 in model 3). Kindred significant correlation were observed amongst TyG-BMI, AIP, METS-IR, as well as MACE. The TyG index was observed to escalate the risk stratification capacity of the MAGGIC score (AUC from 0.601 to 0.666). Once contrasted with other IR pointers, the TyG index illustrated superior differentiation in addition to reclassification capabilities in anticipating MACE. Furthermore, the TyG-BMI index displayed a U-shaped association amongst MACE, pointing that both an escalated along with a lesser TyG-BMI index readings were correlated with an escalated risk(see Figure1-3).
Figure1: Kaplan-Meier curves by the category of the IR indexes. TyG index (A), TyG-BMI (B), AIP (C), METS-IR (D). IR, insulin resistance; TyG, triglyceride-glucose; TyG-BMI, triglyceride-glucose index with body mass index; AIP, atherogenic index of plasma; METS-IR, metabolic score for insulin resistance
Figure2: RCS for the associations between the IR indexes and MACE. Red shadows and lines represent the 95% CI. TyG index (A), TyG-BMI (B), AIP (C), METS-IR (D). HR (95%CI) was adjusted according to the model 3. RCS, restricted cubic spline; IR, insulin resistance; MACE, major adverse cardiovascular event; HR, hazard ratio; CI, confidence interval; TyG, triglyceride-glucose; TyG-BMI, triglyceride-glucose index with body mass index; AIP, atherogenic index of plasma; METS-IR, metabolic score for insulin resistance
Figure3: Subgroup analysis of the IR indexes (per 1 SD) for MACE. TyG index (A), TyG-BMI (B), AIP (C), METS-IR (D). IR, insulin resistance; SD, standard deviation; MACE, major adverse cardiovascular event; TyG, triglyceride-glucose; TyG-BMI, triglyceride-glucose index with body mass index; AIP, atherogenic index of plasma; METS-IR, metabolic score for insulin resistance; HR, hazard ratio; CI, confidence interval; BMI, body mass index; CKD, chronic kidney disease; LVEF, left ventricular ejection fraction; LA, left atrial
Conclusion
Thereby, the conclusions drawn were full four IR indices are autonomously correlated with MACE in patients with HFpEF. Noticably, suchIR indices significantly escalate the anticipative correctness of the MAGGIC score, a broadly utilized risk assessment tool in HFpEF.
. Of such indices, the TyG index illustrated the greatest differentiatory as well as reclassification capabilities, yielding the highest conglomerative readings in anticipating MACE in addition to illustrating significant superiority in contrast to the other indices. Such observations emphasize the significance of evaluating IR indices, specifically the TyG index, in the risk evaluation as well as management approaches for HFpEF patients. Nevertheless, noticeably requirement exists to corroborate their observations in variable populations for guaranteeing their application along with generalization.
References:
1. Kulvinder Kochar Kaur,Allahbadia GN,Singh M. Role of Adipocyte impairment in Heart Failure Induction in subjects that are obese along with prediabetes and overt Diabetes mellitus -A Systematic Review.J Cardiol &Card Disord 2021;2(1):1-21.
2. Kulvinder Kochar Kaur,Allahbadia GN,Singh M. “Paradoxical Additional Role of SGLT2 Inhibitors Beyond Glycosuria in Controlling Obesity, NAFLD Treatment, Pancreatic β Cell Protection Besides Therapy for Diabetes Mellitus, CVOT and Renoprotection-A Minireview". Acta Scientific Gastrointestinal Disorders2021; 4 .7 (): 15-26
3. Kulvinder Kochar Kaur,Allahbadia GN,Singh M. Updating the Classification of Type 2 Diabetes Mellitus Subgroups by Ahlqvist for Achievemenof Individualized Treatment Approaches for greater DM C5ontrol from Initiation and Avoidance of End Stage Damage. Pancreat Disord Ther.2021; 11:218.
4. Kulvinder Kochar Kaur,Allahbadia GN,Singh M.Association of Iron Metabolism Abnormalities as Etiopathogenetic Factor in Alteration of Beta Cell Function and Impairment in Generation of Diabetes Mellitus: A Systematic Review. J Clinical Research and Reports, 2022;11(1); DOI:10.31579/2690-1919/241
5. Kulvinder Kochar Kaur,Allahbadia GN,Singh M.’An Update on Molecular Modes Implicated in Diastolic Impairment in Early Diabetic Cardiomyopathy;Probable Modes of Therapy &Avoidance-A Narrative Review’’. I J cardio & card diso; 2023;4(2)12-21.
6. Kulvinder Kochar Kaur,Allahbadia GN,Singh M.Diabetic Cardiomyopathy: An Update on Its PathophysiologyWith SpecifEmphasis on Epigenetics Modifications BesideTreatment – A Systematic Review. BOHR International Journal of Current Research in Diabetes and Preventive Medicine2022; 1(1):. 1–16.https://doi.org/10.54646/bijrdpm.001-changedto DOI (i.e., 10.54646/bijrdpm.2023.01
7. Kulvinder Kochar Kaur,Allahbadia GN,Singh M. ’Resurgence of idea of hypertriglyceridemia and Lesser serum (HDL-C) as predictive factors for insulin resistance (IR) & type 2 Diabetes mellitus development-A narrative review’’2025-undergalley proof.
8. Kulvinder Kochar Kaur,Allahbadia GN,Singh M.
9. Redfield MM, Borlaug BA. Heart failure with preserved ejection fraction: a review. JAMA. 2023;329(10):827–38. https:/ /doi.or g/10.10 01/j ama.2023.2020.
10. Borlaug BA. Evaluation and management of heart failure with preserved ejec¬tion fraction. Nat Rev Cardiol. 2020;17(9):559–73. h t t p s : / / d o i . o r g / 1 0 . 1 0 3 8 / s 4 1 56 9 - 0 2 0 - 0 3 6 3 - 2 .
11. Gerber Y, Weston SA, Redfield MM, et al. A contemporary appraisal of the heart failure epidemic in Olmsted County, Minnesota, 2000 to 2010. JAMA Intern Med. 2015;175(6):996–1004. h t t p s : / / d o i . o r g / 1 0 . 1 0 0 1 / j a m a i n t e r n m e d . 2 01 5 . 0 9 2 4 .
12. Bhambhani V, Kizer JR, Lima JAC, et al. Predictors and outcomes of heart fail¬ure with mid-range ejection fraction. Eur J Heart Fail. 2018;20(4):651–9. https:/ /doi.or g/10.10 02/e jhf.1091.
13. Tsao CW, Lyass A, Enserro D, et al. Temporal trends in the incidence of and mortality associated with heart failure with preserved and reduced ejection fraction. JACC Heart Fail. 2018;6(8):678–85. h t t p s : / / d o i . o r g / 1 0 . 1 0 1 6 / j . j c h f . 2 0 1 8 . 03 . 0 0 6 .
14. Dunlay SM, Roger VL, Redfield MM. Epidemiology of heart failure with pre¬served ejection fraction. Nat Rev Cardiol. 2017;14(10):591–602. h t t p s : / / d o i . o r g /1 0 . 1 0 3 8 / n r c a r d i o . 2 0 1 7 . 6 5 .
15. Haass M, Kitzman DW, Anand IS, et al. Body mass index and adverse cardio¬vascular outcomes in heart failure patients with preserved ejection fraction: results from the Irbesartan in Heart failure with preserved ejection fraction (I-PRESERVE) trial. Circ Heart Fail. 2011;4(3):324–31. h t t p s : / / d o i . o r g / 1 0 . 1 1 6 1 / C I RC H E A R T F A I L U R E . 1 1 0 . 9 5 9 8 9 0 .
16. Meta-analysis Global Group in Chronic Heart Failure (MAGGIC). The survival of patients with heart failure with preserved or reduced left ventricular ejection fraction: an individual patient data meta-analysis. Eur Heart J. 2012;33(14):1750–7. https:/ /doi.or g/10.10 93/e urheartj/ehr254.
17. Paneni F, Beckman JA, Creager MA, Cosentino F. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part I. Eur Heart J. 2013;34(31):2436–43. https:/ /doi.or g/10.10 93/e urheartj/eht149.
18. Capone F, Sotomayor-Flores C, Bode D, et al. Cardiac metabolism in HFpEF: from fuel to signalling. Cardiovasc Res. 2023;118(18):3556–75. 10.1093/cvr/cvac166.
19. Hahn VS, Petucci C, Kim MS, et al. Myocardial metabolomics of human heart failure with preserved ejection fraction. Circulation. 2023;147(15):1147–61. https:/ /doi.or g/10.11 61/C IRCULATIONAHA.122.061846.
20. Defronzo RA. Banting lecture. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. Diabetes. 2009;58(4):773–95. https:/ /doi.or g/10.23 37/d b09-9028.
21. Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Compari¬son with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95(7):3347–51. https:/ /doi.or g/10.12 10/j c.2010-0288.
22. Ramírez-Vélez R, Pérez-Sousa MÁ, González-Ruíz K, et al. Obesity- and lipid-related parameters in the identification of older adults with a high risk of Prediabetes according to the American Diabetes Association: an analysis of the 2015 Health, Well-Being, and Aging Study. Nutrients. 2019;11(11):2654. https:/ /doi.or g/10.33 90/n u11112654.
23. Dobiásová M. AIP–aterogenní index plazmy jako významný prediktor kardio-vaskulárního rizika: Od výzkumu do praxe [AIP–atherogenic index as a significant predictor of cardiovascular risk: from research to practice. Vnitr Lek. 2006;52(1):64–71.
24. Bello-Chavolla OY, Almeda-Valdes P, Gomez-Velasco D, et al. METS-IR, a novel score to evaluate insulin sensitivity, is predictive of visceral adiposity and incident type 2 diabetes. Eur J Endocrinol. 2018;178(5):533–44. h t t p s : / / d o i . o r g /1 0 . 1 5 3 0 / E J E - 1 7 - 0 8 8 3 .
25. Ramdas Nayak VK, Satheesh P, Shenoy MT, Kalra S. Triglyceride glucose (TyG) index: a surrogate biomarker of insulin resistance. J Pak Med Assoc. 2022;72(5):986–8. https:/ /doi.or g/10.47 391/ JPMA.22-63.
26. Tao LC, Xu JN, Wang TT, Hua F, Li JJ. Triglyceride-glucose index as a marker in cardiovascular diseases: landscape and limitations. Cardiovasc Diabetol. 2022;21(1):68. https:/ /doi.or g/10.11 86/s 12933-022-01511-x. Published 2022 May 6.
27. Pocock SJ, Ariti CA, McMurray JJ, et al. Predicting survival in heart fail¬ure: a risk score based on 39 372 patients from 30 studies. Eur Heart J. 2013;34(19):1404–13. https:/ /doi.or g/10.10 93/e urheartj/ehs337.
28. NiW, JiangR, XuD, ZhuJ, ChenJ, LinU, Zhou H. Association between insulin resistance indices and outcomes in patients with heart failure with preserved ejection fraction . Cardiovascular Diabetology2025 24:32.
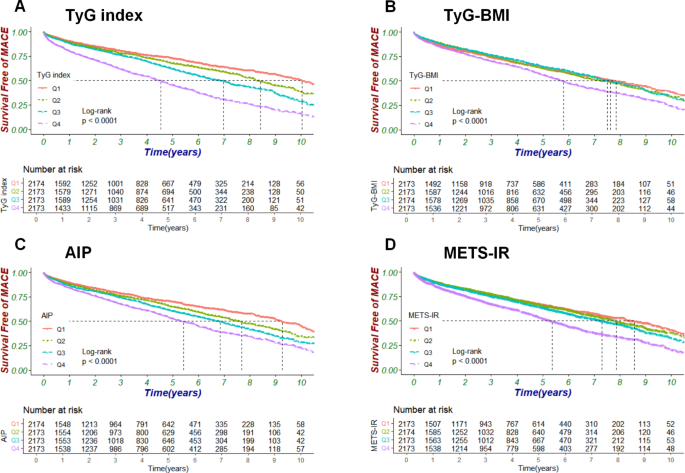
Figure 1
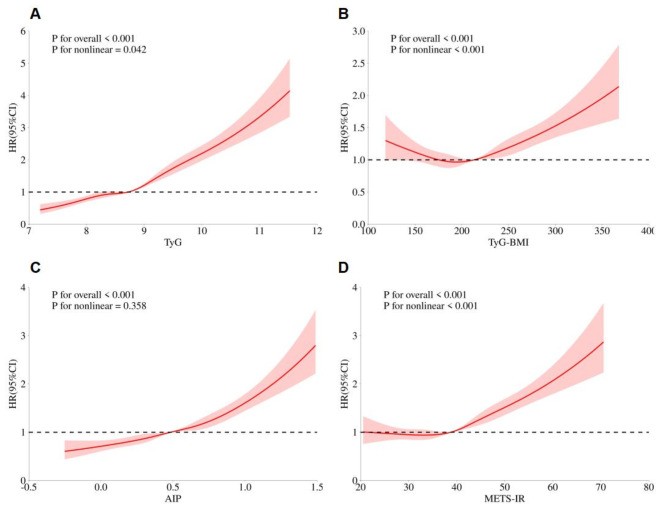
Figure 2
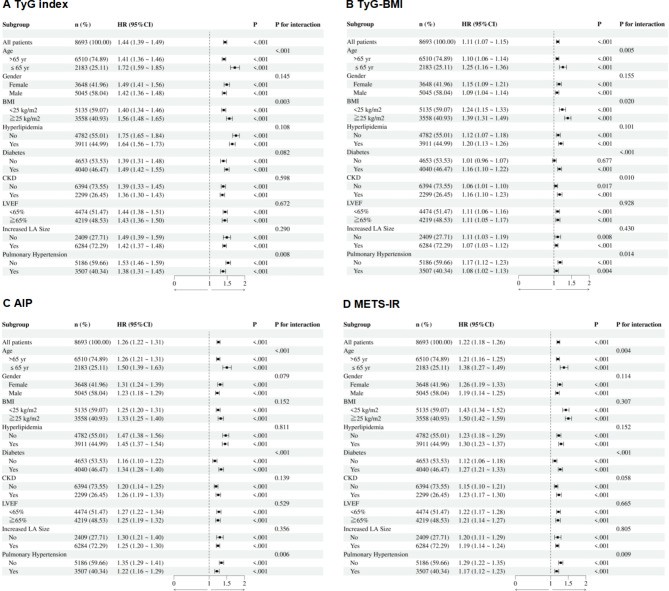
Figure 3