Idiopathic Intracranial Hypertension in a Non-Obese Patient: An Unusual Presentation
Idiopathic Intracranial Hypertension in a Non-Obese Patient: An Unusual Presentation
Dr. Khaled Skafi*, Dr. Yasmina Chaa1, Dr. Ayman Mabchour2, Dr. Nacima Kisma
- Department of Ophthalmology, Hospital Civil Marie Curie, Belgium.
- Department of Ophthalmology, Hospital Erasme in Brussels, Belgium.
- Department of Ophthalmology, CHIREC Hospital Group, Belgium.
*Correspondence to: Dr. Khaled Skafi, Department of Ophthalmology, University Hospital of Brussels, Belgium.
Copyright
© 2025 Dr. Khaled Skafi, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 July 2025
Published: 06 August 2025
Abstract:
Purpose: To report an unusual presentation of idiopathic intracranial hypertension in a non-obese female patient and to emphasize the importance of considering this diagnosis even in individuals who do not meet the typical demographic characteristics.
Observations: A 33-year-old female with a body mass index of 24.1 presented with swelling of the optic nerve heads in both eyes and transient episodes of blurred vision, more pronounced in the left eye. Despite a normal magnetic resonance imaging scan of the brain, a lumbar puncture demonstrated an elevated opening pressure of the cerebrospinal fluid with normal composition, confirming the diagnosis of idiopathic intracranial hypertension. Treatment with a high dosage of the carbonic anhydrase inhibitor acetazolamide led to improvement of the swelling of the optic nerve heads and the visual field defects. After seven years of follow-up, the patient developed headaches and worsening of vision due to the development of a thrombosis in the lateral venous sinuses, which was successfully treated with the placement of two venous stents, resulting in complete resolution of symptoms.
Conclusions and Importance: This case illustrates that idiopathic intracranial hypertension can also occur in individuals with a normal body mass index and that recent weight gain, even without obesity, may play a role in the development of this condition. A thorough medical history and a complete diagnostic approach are essential to establish the correct diagnosis. Furthermore, individuals with idiopathic intracranial hypertension who do not fit the classical patient profile may represent a distinct subgroup requiring tailored diagnostic and therapeutic management.
Keywords: Idiopathic intracranial hypertension; Papilledema; Visual field defects; Non-obese patient; Cerebrospinal fluid pressure; Venous sinus thrombosis.
Idiopathic Intracranial Hypertension in a Non-Obese Patient: An Unusual Presentation
Introduction
The term papilledema refers to swelling of the optic disc secondary to increased intracranial pressure. [1] Though this condition is associated with different etiologies, it is most commonly caused by idiopathic intracranial hypertension (IIH). [2] The diagnosis of IIH is based on the fulfillment of the modified Dandy criteria, including symptoms and signs of increased intracranial pressure (ICP); absence of localizing neurologic signs, except for unilateral or bilateral sixth nerve palsies; presence of an increased cerebrospinal fluid (CSF) opening pressure, yet with normal CSF composition; elimination of hydrocephalus, mass, structural, or vascular lesions on imaging; exclusion of any other cause of increased intracranial pressure. [3]
While this disorder primarily affects obese women of childbearing age, [4] a few cases of IIH in non-obese individuals have been reported in the scientific literature. [5,6] Given these rare occurrences in non-obese individuals, we have herein presented an unusual case of IIH, characterized by bilateral papilledema in a non-obese patient without any familial IIH history and with an elevated CSF opening pressure. This reported observation clearly highlights that a thorough evaluation and differential diagnosis is relevant when patients present with optic disc swelling, and it stresses the need to consider all potentially associated factors, such as the patient's medical history and recent weight changes, in order to reach an accurate diagnosis and initiate effective treatment strategies.
Case Presentation
A 33-year-old female patient with bilateral optic disc swelling was referred to our uveitis clinic for a second opinion. She reported experiencing episodes of transient visual obscurations accompanied by narrowing of the left visual field. These symptoms have persisted for the past three years. Her medical history revealed a history of migraines and bilateral laser-assisted in situ keratomileusis (LASIK). She was not on any medications. Her weight was 56 kg, her height 152 cm, and her body mass index (BMI) was 24.1.
Upon examination at our department, the patient’s best-corrected visual acuity (BCVA) was 20/20 in both eyes. The pupillary and slit-lamp examinations were unremarkable. However, fundus examination revealed bilateral optic disc swelling, which was more pronounced in the left eye (Fig. 1).
Standard automated perimetry revealed concentric narrowing of the visual field, more marked in the left eye compared to the right, in addition to decreased foveal sensitivity in both eyes (Fig. 1). Optical coherence tomography (OCT) displayed thickened retinal nerve fiber layers, whereas the macular structure appeared normal. No optic disc drusen were noted on fundus autofluorescence. Fluorescein angiography revealed sublte hyperfluorescence with late diffusion of the nasal optic discs margins. An indocyanine green angiography was performed as well, without yielding notable findings.
To rule out infectious or inflammatory causes, the patient underwent laboratory testing. IgM serologies were negative for Toxoplasma gondii, CMV, VZV, EBV, Borrelia Burgdorferi and Bartonella Henselae. Serologies were negative for HIV, syphilis, rickettsiae and leptospirosis as well. IgG serologies were positive for Toxoplasma gondii, HSV1-2, VZV, CMV and EBV. TB screening (QuantiFEROn-TB gold) was negative.The brain magnetic resonance imaging (MRI) was unremarkable.
Despite initiating oral methyprednisolone therapy at a dose of 0.8mg/kg/day for one month, the optic disc swelling did not improve.
Faced with this isolated disc swelling, without any signs of inflammation or infection, we conducted a directed history.
This second medical history-taking revealed that the patient had gained seven kilograms over the past two years, although without being classified as overweight. Therefore, the observed findings were likely consistent with IIH. A lumbar puncture was thus performed, revealing an elevated CSF opening pressure at 60cm H?O with normal CSF composition.
Figure 1: Color fundus images showing optic disc swelling in the right (top left) and the left (top right) eye and corresponding visual field (automated 30/2 Humphrey visual field) showing annular scotoma on the left (bottom right) more marked than the right (bottom left) eye.
Figure 2: Color fundus images showing a marked improvement of the optic discs swelling (top images) as well as a reduction in visual field defects (bottom) in both eyes several months after initiation of oral acetazolamide (right eye on the left, left eye on the right).
The patient was then treated with oral acetazolamide at a high dosage (750 mg three times a day) and this therapeutic strategy resulted in a prompt improvement of both papilledema and visual field during follow-up (Fig. 2). After almost seven years, while still on the same dosage of acetazolamide, the patient complained of headaches and visual deterioration. The MRI revealed lateral sinuses thrombosis, and venous sinus stenting (2 stents) was performed. This single procedure abolished the headaches and improved the patient’s visual fields.
Discussion
This case of papilledema in a non-obese patient with IIH underscores the complexity of diagnosing and managing this disorder in individuals who do not fit the typical profile.
While the patient presented with bilateral optic disc swelling, transient visual blurring, and visual field defects, she had a BMI of 24.1, thus within the normal weight range. As this observation aligns with other reported cases of IIH occurring in non-obese individuals, we assume that IIH can affect patients outside of the typical demographic group. Indeed, the patient’s recent weight gain (approximately 15% of her initial body weight) had initially been underestimated. Whereas MRI showed no abnormalities, lumbar puncture revealed an elevated CSF opening pressure of 60cm H?O with normal CSF composition, representing a key diagnostic criterion for IIH.
Treatment with the carbonic anhydrase inhibitor acetazolamide, which is commonly employed to reduce intracranial pressure, was associated with improvements in both papilledema and visual fields. This outcome is consistent with standard IIH treatment protocols, thus demonstrating that these therapies are also effective in non-obese patients.
While IIH is usually observed in obese women of childbearing age, several case reports have previously described atypical presentations, such as familial IIH or uncharacteristic IIH specificities in non-obese women. Familial IIH is relatively rare, and it may be unrecognized when not associated with obesity. In the literature, several reports have highlighted genetic components that are likely to contribute to this condition in non-obese patients. In 2022, Behbehani et al. described a family with IIH spanning three generations, including one father and three offspring involving two males and one female, all being non-obese individuals. [5] Furthermore, other authors have discussed atypical IIH specificities recorded in non-obese patients. In a retrospective 2024 study involving 246 IIH patients, Horev et al. demonstrated that non-obese patients were likely younger and presented higher rates of severe papilledema, scleral flattening, and optic nerve dural ectasia compared with obese patients. [6]
Pathological processes other than obesity that have been linked to IIH development include hormonal dysregulation and alterations in the metabolic neuroendocrine axis. [7] In addition, a number of drugs, such as vitamin A derivatives, tetracycline-class antibiotics, recombinant growth hormone, as well as lithium, were found to be strongly associated, corticosteroids to be moderately associated, and other drugs like cyclosporine, progestin-only contraceptives, as well as others, to be only weakly associated with IIH development. [8] A significant disruption to the normal CSF circulation can similarly lead to intracranial pressure elevation. [9] Regarding CSF dynamics, it is important to note that IIH cases with normal CSF opening pressures have been reported. Indeed, in 2013, Suh SY et al. reported on IIH cases with normal opening pressures at lumbar puncture, further underscoring the complexity of the diagnosis. [10] The presented case underscores the importance of a thorough anamnesis during the clinical examination. An elaborate clinical history can help consider new diagnostic hypotheses. This case also highlights the significant clinical consequences of delayed diagnosis. In our patient, the diagnosis of IIH was only established after three years of persistent symptoms and misattributed optic disc swelling. As a result, she developed pronounced and lasting visual field defects, particularly in the left eye. Earlier recognition and appropriate intervention could potentially have mitigated this irreversible visual damage. This emphasizes the importance of always keeping IIH in the differential diagnosis of bilateral optic disc swelling, notably in non-obese patients.
Conclusion
The clinical case presented herein confirms IIH as a heterogeneous condition observed across various patient groups, including non-obese individuals. Notably, normal CSF pressures do not exclude the diagnosis of IIH, emphasizing the necessity of a comprehensive diagnostic approach. Non-obese patients with IIH represent a distinct subgroup with unique characteristics that may require tailored management strategies. Recognizing these differences likely helps mitigate the risk of both under- and misdiagnosis. Future research should focus on elucidating the mechanisms underlying IIH in non-obese patients and developing diagnostic and therapeutic guidelines specific to this subgroup.
Patient Consent: Written consent to publish this case has been obtained from the patient.
Acknowledgements and Disclosures
Funding: No funding or grant support.
Conflicts of Interest: The authors have no financial disclosures
Authorship: All authors attest that they meet the current International Committee of Medical Journal Editors (ICMJE) criteria for Authorship.
Acknowledgements: None.
References
1. Rigi M, Almarzouqi SJ, Morgan ML, Lee AG. Papilledema: epidemiology, etiology, and clinical management. Eye Brain [Internet]. 2015;7:47–57. Available from: http://dx.doi.org/10.2147/EB.S69174
2. Crum OM, Kilgore KP, Sharma R, Lee MS, Spiegel MR, McClelland CM, et al. Etiology of papilledema in patients in the eye clinic Setting. JAMA Netw Open [Internet]. 2020;3(6):e206625. Available from: http://dx.doi.org/10.1001/jamanetworkopen.2020.6625
3. Thurtell MJ, Wall M. Idiopathic intracranial hypertension (pseudotumor cerebri): recognition, treatment, and ongoing management. Curr Treat Options Neurol [Internet]. 2013;15(1):1–12. Available from: http://dx.doi.org/10.1007/s11940-012-0207-4
4. Grech O, Mollan SP, Wakerley BR, Alimajstorovic Z, Lavery GG, Sinclair AJ. Emerging themes in idiopathic intracranial hypertension. J Neurol [Internet]. 2020;267(12):3776–84. Available from: http://dx.doi.org/10.1007/s00415-020-10090-4
5.Behbehani R, Ali A, Al-Mousa AJ, Albuloushi SN. Familial non-obese idiopathic intracranial hypertension. Am J Ophthalmol Case Rep [Internet]. 2022;27(101619):101619. Available from: http://dx.doi.org/10.1016/j.ajoc.2022.101619
6. Horev A, Ben-Arie G, Zlotnik Y, Koltochnik M, Ben Chaim O, Biederko R, et al. Clinical and radiological characteristics of non-obese female patients with idiopathic intracranial hypertension. J Clin Med [Internet]. 2024;13(6):1547. Available from: http://dx.doi.org/10.3390/jcm13061547
7. Virdee J, Larcombe S, Vijay V, Sinclair AJ, Dayan M, Mollan SP. Reviewing the recent developments in idiopathic intracranial hypertension. Ophthalmol Ther [Internet]. 2020;9(4):767–81. Available from: http://dx.doi.org/10.1007/s40123-020-00296-0
8. Tan MG, Worley B, Kim WB, Ten Hove M, Beecker J. Drug-induced intracranial hypertension: A systematic review and critical assessment of drug-induced causes. Am J Clin Dermatol [Internet]. 2020;21(2):163–72. Available from: http://dx.doi.org/10.1007/s40257-019-00485-z
9. Bothwell SW, Janigro D, Patabendige A. Cerebrospinal fluid dynamics and intracranial pressure elevation in neurological diseases. Fluids Barriers CNS [Internet]. 2019;16(1):9. Available from: http://dx.doi.org/10.1186/s12987-019-0129-6
10. Suh SY, Kim S-J. IIH with normal CSF pressures? Indian J Ophthalmol [Internet]. 2013;61(11):681–2. Available from: http://dx.doi.org/10.4103/0301-4738.119416.
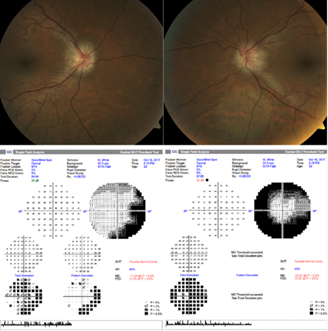
Figure 1
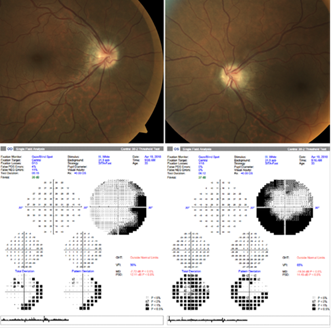
Figure 2