Pediatric Ectopic Lenses: Feedback from the Pediatric Ophtalmology Department – Morocco
Pediatric Ectopic Lenses: Feedback from the Pediatric Ophtalmology Department – Morocco
G.Daghouj1, S.Houti2, S.Dahrane3, M.Otssaso4, Z. Laftimi5, L. El Maaloum6, B. Allali7, A. El Kettani8
1,3,4,5,6,7,8. Pediatric Ophthalmology Department Casablanca Morocco.
2. Ophthalmology Department Casablanca Morocco.
*Correspondence to: G.Daghouj, Pediatric Ophthalmology Department Casablanca Morocco.
Copyright
© 2025 G.Daghouj This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 July 2025
Published: 12 August 2025
Abstract:
Ectopia lentis is a congenital displacement of the crystalline lens caused by abnormalities of the zonular fibers. It is a rare, progressive, and potentially severe condition that can compromise visual—and sometimes systemic—prognosis, particularly when associated with other malformations.
We conducted a retrospective descriptive study involving 63 children who underwent surgery for ectopia lentis at the pediatric ophthalmology department of Casablanca University Hospital between January 2010 and September 2022. Cases with traumatic etiology were excluded.
The mean age at surgery was 7.5 years, with a male predominance (70%). The most common reason for consultation was reduced visual acuity, often detected at school. A family history was found in 16% of cases. The condition was bilateral in all patients, with corrected visual acuity ranging from hand motion to 3/10. High myopia was present in 33% of cases. The lens was subluxated in 65%, with two cases of anterior chamber dislocation.
Associated ocular anomalies included: aniridia (5%), cataract (14%), ocular hypertension (2.5%), and peripheral retinal degenerative lesions (20%). All patients underwent phacophagy combined with anterior vitrectomy. Aphakia was corrected using aphakic glasses or contact lenses, along with amblyopia therapy. One 17-year-old girl received an Artisan intraocular lens. Final visual acuity was better than 5/10 in 30% of eyes.
Postoperative complications were rare, with two cases of retinal detachment and two cases of glaucoma. Visual prognosis depended on the degree and type of lens displacement as well as the presence of associated ocular lesions. Conservative management is reserved for mild, uncomplicated forms under close monitoring. The diagnosis of ectopia lentis should prompt a systematic etiological investigation, family screening, and long-term follow-up, even after surgical treatment.
Key words: Ectopia lentis – Pediatric – Lens surgery- Visual prognosis- Amblyopia.
Pediatric Ectopic Lenses: Feedback from the Pediatric Ophtalmology Department – Morocco
Introduction
Ectopic lentis is a congenital displacement of the lens related to a zonular anomaly (1) . Berry being the first who documented the first case of ectopia lentis in 1749 then came Stellwag to be the first to name it ' ectopia lentis ' in 1856 (2) . It is a rare, serious and progressive disease (3) . The lens displacement can occur in different directions and can be a source of serious ocular complications, dominated by ocular hypertension and retinal detachment. Treatment is mainly surgical. The visual prognosis is essentially linked to early diagnosis, the quality of medical and surgical management of ectopia as well as long-term follow-up and management of subsequent amblyopia (4) . The vital prognosis can be jeopardized by the associated general malformations, mainly cardiac. The aim of our work is to describe the clinical, epidemiological, therapeutic and progressive profile of this pathology.
Materials and Methods
This is a retrospective descriptive study of 126 eyes of 63 children with ectopia lentis collected in the pediatric ophthalmology department of Ibn Rochd University Hospital in Casablanca, over a period of 12 years from January 2010 to September 2022. We collected in our study children treated for ectopia lentis in the department, whose postoperative follow-up is assured for at least one and a half years, and we excluded all cases of traumatic ectopia lentis, adult ectopias or cases of children lost to follow-up or in whom postoperative follow-up was insufficient. Data collection is carried out from hospitalization medical records, assisted by an operating sheet completed by resident doctors on duty. The main variables studied were epidemiological data, functional signs, clinical and paraclinical examination data, etiological profile, management provided, postoperative complications as well as postoperative results with the evolutionary profile and visual acuity. We excluded traumatic lens subluxations from our study.
Results
We included 63 children with ectopia lentis (126 eyes) in our study. The mean age of the operated children was 7.5 years with a clear male predominance (70% were boys). The majority of children were diagnosed during school or preschool age . (Figure 1).
Figure 1: Distribution of patients by age group
The reason for consultation varies: 46% of children have a decrease in visual acuity noted by their parents, 18% have poor visual behavior. Strabismus was present in 18% of patients. Finally, 8 patients were diagnosed following school screening.
Figure 2: Distribution of patients according to the reason for consultation
For personal and family history, the notion of consanguinity was found in 36% of children, similar cases in the family in 16% and a delay in psychomotor development in 12% of cases. A On clinical examination, corrected visual acuity, when it could be quantified, was between hand movement and 3/10th. Refraction under cycloplegia found an average astigmatism of -3.75 with extremes ranging from -0.75 to -7.25, and an average myopia of -13D with extremes from -2 to the oversphere. Ectopy was bilateral in all patients, with in 3% of cases the presence of an anterior lens dislocation on admission (Photo 1)
Photograph 1: intraoperative ectopic lens.
The direction of lens displacement varies from one patient to another, dominated by displacement in the supero -temporal direction (30% of cases) and infero-nasal direction (22% of cases) (Figure 3).
Figure 3 : Direction of lens displacement
Photograph 3: Dislocated lens in the anterior chamber.
There are also other associated anomalies such as aniridia in 5% of cases and cataracts (photograph 2) in 14% of cases. We also found degenerative lesions of the retinal periphery in 20% of patients at the fundus; these were lasered preoperatively. Ocular hypertension was present in 2.5% of cases, which was well controlled under medical treatment.
Photograph 2: Ectopia lentis with cataract
The preoperative assessment systematically included a pre-anesthetic consultation , a search for homocysteinuria , as well as a cardiac ultrasound to detect any associated cardiac malformations. Marfan syndrome represented the main etiology, found in 40% of cases, followed by homocysteinuria in 8% of cases. In 50% of cases, ectopia lentis was isolated, without associated pathology.
Photo 4: ectopia lentis on homocysteinuria
Heart disease was diagnosed in 5 patients, mainly in the form of mitral regurgitation and aortic dilatation.
Surgically, management was primarily based on phacophagy with capsular bag removal and anterior vitrectomy, performed in 98.4% of cases. An Artisan implant was performed in two eyes in an 18-year-old patient.
All patients underwent follow-up in a pediatric ophthalmology clinic. The mean follow-up period for the study was 18 months.
Aphakia correction was based on the wearing of glasses or lenses, combined with treatment of amblyopia. Final visual acuity was greater than 5/10 in 30% of eyes, and between 1/10 and 5/10 in 46% of cases. (Figure 4)
Regarding post-operative complications: two patients presented retinal detachment, 3 eyes presented a strong inflammatory reaction well controlled under medical treatment, and finally two patients presented aphakic glaucoma .
Figure 4 : Final visual acuity
Discussion
Ectopic lentis is a rare congenital malformation, resulting from a displacement of the lens outside its normal position, due to asymmetric stretching or rupture of the zonular fibers. This pathology, although uncommon, can develop progressively and lead to severe visual complications if it is not treated early. It represents approximately 0.3% of congenital ocular anomalies, with an estimated prevalence of 0.2 per 10,000 births in France [1].
The majority of forms are autosomal dominant and present without systemic involvement [2,3]. However, a number of cases are associated with genetic syndromes, including Marfan syndrome and homocysteinuria , two etiologies that we found in 40% and 8% of cases, respectively. These results are consistent with data from the literature, which designate Marfan syndrome as the most frequently associated syndromic cause [4].
In our series, the mean age at diagnosis was 7.5 years, which is slightly lower than that reported by Wuchen et al. in the United States (7.7 years) [4] and by Sorath in Pakistan (9.4 years) [5]. This relatively early diagnosis may be explained by the specialization of our unit in the management of pediatric ophthalmology. However, a delay in consultation, often linked to a lack of parental awareness and the absence of systematic screening, remains a major limiting factor. This finding underlines the importance of medical and paramedical awareness to improve early diagnosis, which is essential to prevent amblyopia.
We observed a clear male predominance (70%), in agreement with several previous series [4,5]. In addition, the high rate of consanguinity (36%) in our population could explain the frequency of familial forms.
Clinically, decreased visual acuity or abnormal visual behavior was the main reason for consultation (74%), which is explained by the significant and progressive ametropia induced by lens displacement, making amblyopia common in these children.
The involvement was bilateral in 100% of cases, which is consistent with literature data, unilateral forms being extremely rare and often sporadic [6,7]. Regarding the orientation of the ectopy, the most frequent displacements in our series were temporo-superior (30%) and naso- inferior (22%), confirming the anatomical heterogeneity of the pathology.
Surgical management is essentially based on phacophagy associated with removal of the capsular bag and anterior vitrectomy, a technique that we performed in 98.4% of cases. This approach is validated by several studies to limit the risk of complications such as secondary glaucoma or retinal detachments [8]. Secondary implantation is discussed on a case-by-case basis; in our series, an Artisan implant was placed in a single patient aged 18, due to its ocular stability and technical feasibility.
The correction of aphakia was based on the wearing of glasses or contact lenses, in association with treatment of amblyopia. The final visual acuity was satisfactory in a significant proportion: greater than 5/10 in 30% of cases and between 1/10 and 5/10 in 46%, results comparable to those reported in other series [4,5]. The average follow-up of 18 months is however a limitation, not allowing a complete evaluation of the long-term results or late complications.
In summary, our study highlights the challenges of early screening, multidisciplinary management (ophthalmological, genetic, cardiological), and appropriate visual rehabilitation in ectopia lentis. Greater awareness among healthcare professionals, coupled with effective follow-up organization, would reduce visual sequelae and improve the quality of life of these patients. Table 1 compares epidemiological and clinical data in different studies.
In 50% of cases, ectopia lentis is isolated, without associated systemic abnormality. Among the syndromic forms, Marfan syndrome is the most common etiology, identified in 40% of cases, followed by homocysteinuria , found in 8% of cases. Table 2 presents a comparison of the frequencies of these two main etiologies reported in different studies. These data underline the importance of a rigorous general clinical examination, systematically supplemented by a plasma homocysteine measurement and, if necessary, a skin biopsy in order to guide the etiological diagnosis in the face of any ectopia lentis.
Table 1: Literature review comparing epidemiological and clinical data on ectopic lenses
|
Wen Y. Wu-Chen (USA) % |
Sorath . N (Pakistan) % |
J. Fuchs (Denmark) % |
Our series (Casablanca) % |
|
|
Marfan syndrome |
52.9 |
22 |
47.2 |
40% |
|
Weill syndrome Marchesani |
0 |
4 |
0.5 |
0 |
|
Homocysteinuria |
11.7 |
2 |
0.75 |
8% |
|
Syndrome d' Ehrles Danlos |
0 |
0 |
0 |
0 |
|
Ectopia lentis simple |
11.7 |
72 |
5.55 |
52% |
|
Ectopia pupillis |
17.6 |
0 |
14.64 |
0 |
|
Sulfite oxidase deficiency |
0 |
0 |
0.5 |
0 |
|
Wen Y. Wu-Chen (USA) |
Sorath . N (Pakistan) |
Nejjari.O (Fez) |
Our series (Casablanca) |
|
|
Age of diagnosis: years (number of patients) |
7.7 (11) |
9.4 (50) |
16 years old (18) |
7.5 years (63) |
|
Male gender |
52% |
60% |
68% |
70% |
|
Direction of the most common ectopy |
Lower (29.4%) |
Temporal (36.5%) |
Supertemporal (41%) |
Supertemporal (30%) |
|
Bilateral involvement |
100% |
100% |
100% |
100% |
|
Initial AV |
CLD at 2/10 |
CLD at 2/10 |
MDM at 1/10 |
MDM at 3/10 |
|
HTO |
6% |
13% |
4% |
2.5% |
|
|
|
|
|
|
Table 2 : Comparative table comparing the etiological profile of our study with the literature
Although the clinical diagnosis of ectopia lentis is generally easy, its therapeutic management constitutes a real challenge for the ophthalmologist. In the presence of moderate ectopia, without major refractive error or amblyogenic risk , optical correction associated with regular clinical monitoring remains the appropriate course of action.
However, in the majority of cases, especially in late diagnosis settings like ours, the lens is often significantly subluxated, generating significant and amblyogenic ametropia , making surgical management necessary.
Two main surgical techniques are used for the extraction of the ectopic lens: phacophagy with anterior vitrectomy via the limbal approach or vitrectomy via the pars plana. The choice between these approaches depends on multiple factors, including the technical skill of the surgeon, the anatomo-clinical type of ectopy, capsular stability, as well as the presence of associated ocular lesions [8,10].
Aphakia is most often corrected by wearing glasses or contact lenses, particularly in young children. Insertion of an intraocular lens (IOL) is less common before the age of two, but may be considered in some cases. The implant can be positioned in the posterior or anterior chamber, in the capsular bag using an intrasaccular ring, or fixed to the sclera, depending on the integrity of the capsular support.
In our series, as in most studies [9,11], the most frequently used technique was phacophagia associated with anterior vitrectomy via the limbal approach, followed by correction of aphakia with glasses.
Among postoperative complications, retinal detachment remains the most feared. It was observed in 1.5% of cases in our series. This risk is all the higher since peripheral retinal degenerative lesions are frequently associated with ectopia lentis, found in 20% of cases.
Conclusion
Ectopic lentis is a rare, progressive, and potentially serious condition. Although its diagnosis is often clinical, it requires rigorous, multidisciplinary management. It is an ophthalmological emergency, as any delay can compromise the long-term visual prognosis. Surgery remains the mainstay of treatment, particularly when the ectopy is severe, amblyogenic , or complicated.
The visual prognosis depends strongly on the degree of subluxation or dislocation of the lens, as well as the presence or absence of associated complications (glaucoma, retinal detachment, amblyopia) [2]. Appropriate optical correction and treatment of amblyopia are essential, even after surgical treatment.
The discovery of a case must systematically be the subject of a thorough etiological investigation and family screening, given the frequency of hereditary forms. Regular long-term monitoring is essential, both ophthalmologically and systemically.
Furthermore, advances in molecular genetics are opening up new perspectives in the understanding of hereditary forms, including isolated ones. A recent study conducted in China identified three new mutations in the FBN1 and LTBP2 genes in families with ectopia lentis, highlighting the importance of genetic diagnosis and family counseling in this complex pathology [12].
In summary, optimal management of ectopia lentis relies on early detection, appropriate surgical management, rigorous post-operative monitoring and, increasingly, on the contribution of genetic analyses, both for diagnosis and for family prevention.
References
1. Derrar R, Daoudi R. School delay revealing ectopia lentis in a 7-year-old child. Pan Afr Med J. May 2, 2014;18:7.
2. Kaur K, Gurnani B. Ectopia Lentis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited May 21, 2023]. Available at: http://www.ncbi.nlm.nih.gov/books/NBK578193/
3. Masson E. 359 Ectopic lenses: about 33 cases [Internet]. EM-Consulte. [cited May 21, 2023]. Available at: https://www.em-consulte.com/article/213392/article/359-ectopies-cristalliniennes-a-propos-de-33-cas
4. Moustaine M. Analysis of the management of ectopic lenses in the pediatric ophthalmology department of Ibn Rochd University Hospital in Casablanca: about 34 cases. ophthalmology.
5. El Hamidi M, Lahlou G, Dgadeg K, Daghouj G, Allali B, Lahbil D, et al. 359 Crystalline ectopias: about 33 cases. French Journal of Ophthalmology. Apr 2009;32:1S118.
6. Noorani S, Khan A, Rubab S, Choudhary KA. Management of Ectopia Lentis in Children.
7. 151-11.pdf [Internet]. [cited 23 May 2023]. Available at: https://cdim.fmp-usmba.ac.ma/mediatheque/e_theses/151-11.pdf
8. Wu-Chen WY, Letson RD, Summers CG. Functional and structural outcomes following lensectomy for ectopia lentis. J AAPOS. Aug 2005;9(4):353 ? 7.
9. Noorani S, Khan A, Rubab S, Choudhary KA. Management of Ectopia Lentis in Children.
10. Liu Y, Chen T, Jiang Y. What Should We Pay More Attention to Marfan Syndrome Expecting Ectopia Lentis: Incidence and Risk Factors of Retinal Manifestations. Journal of Personalized Medicine. March 2023;13(3):398.
11. Roussat B, Chiou AG, Quesnot S, Hamard H, Godde-Jolly D. Surgery for ectopia lentis in Marfan disease in children and young adults. J Fr Ophtalmol. 1995;18(3): 170-7 .
12. Huang L, Xu T, Gan J, Mao Y, Zhao L, Jiao X, et al. Zonule Associated Gene Variants in Isolated Ectopia Lentis and Glaucoma. J Glaucoma. March 20, 2023.
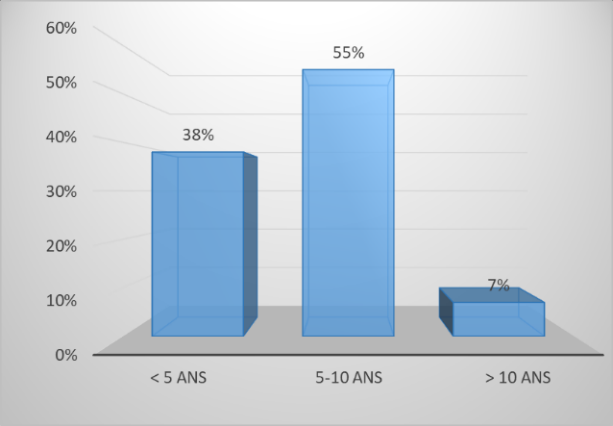
Figure 1

Figure 2
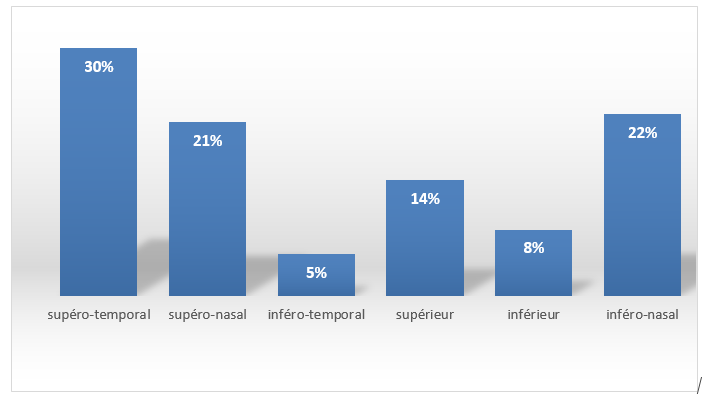
Figure 3
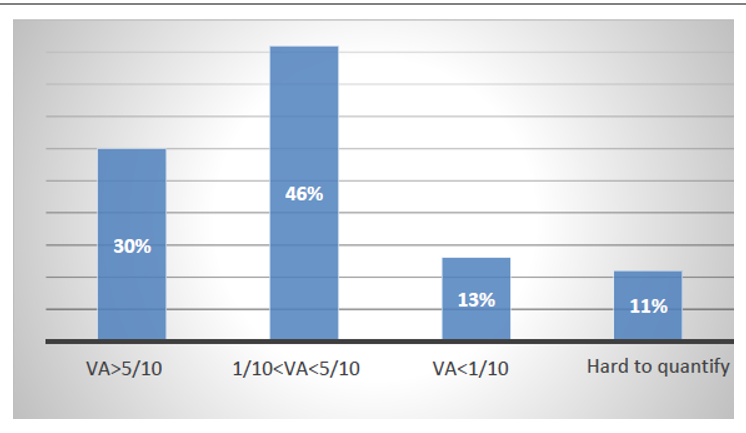
Figure 4
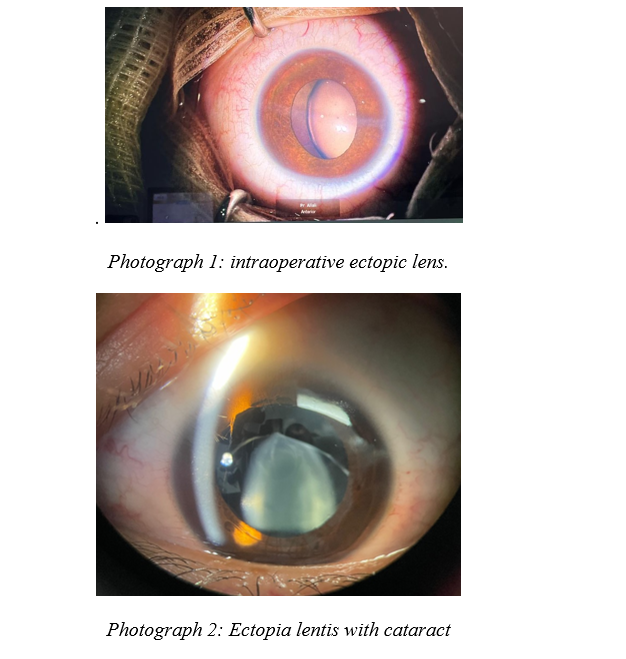
Figure 5
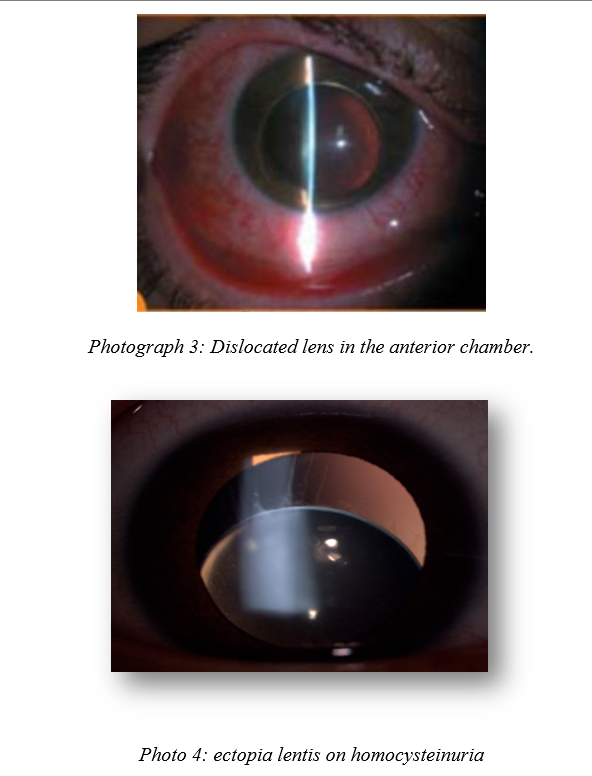
Figure 6