Restoring Sight, Preserving Memory: The Interplay between Cataracts and Dementia
Restoring Sight, Preserving Memory: The Interplay between Cataracts and Dementia
Dr Saumya Harsh Mittal *1, Dr Akansha Kumari 2
1. Sr Consultant Neurologist, Department of Neurology, Yatharth Hospital, Omega 1, Greater Noida (https://orcid.org/0000-0003-0648-1063)
2. Observer, Department of Neurology, Yatharth Hospital, Omega 1, Greater Noida.
*Correspondence to: Dr. Saumya Harsh Mittal, Sr Consultant Neurologist, Department of Neurology, Yatharth Hospital, Omega 1, Greater Noida.
Copyright
© 2025 Dr. Saumya Harsh Mittal, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 Aug 2025
Published: 20 Aug 2025
DOI: https://doi.org/10.5281/zenodo.17043227
Abstract
Cataracts, characterized by the progressive opacification of the eye's natural lens, are one of the most common causes of visual impairment among older adults. Concurrently, dementia—marked by a decline in memory, cognition, and functional ability—presents a major public health challenge, particularly in aging populations. Emerging research suggests a significant association between visual impairment and the risk of cognitive decline and dementia. This review synthesizes current epidemiological data, clinical evidence, and biological theories linking cataracts and cognitive deterioration. Several longitudinal and population-based studies have shown that individuals with untreated cataracts are at an increased risk of developing dementia, while those who undergo cataract surgery may experience reduced dementia risk and even improvements in cognitive function. Proposed mechanisms include sensory deprivation, social isolation, depression, and shared neurodegenerative pathways such as oxidative stress and inflammation. Moreover, cataract surgery appears to restore not only vision but also cognitive engagement by enhancing sensory input and social participation. Despite strong observational support, limitations such as confounding factors and lack of randomized controlled trials warrant cautious interpretation. Nonetheless, early detection and treatment of cataracts may represent a novel, low-risk intervention in the broader strategy for dementia prevention. Future research should focus on causal inference, long-term cognitive outcomes post-surgery, and integration of ophthalmologic care into neurodegenerative disease prevention programs.
Keywords: Cataract, Dementia, Cognitive decline, Visual impairment, Sensory deprivation, Cataract surgery, Alzheimer’s disease, Neurodegeneration, Aging, Ophthalmology, Public health, Brain aging, Cognitive reserve, Inflammation, Oxidative stress
Restoring Sight, Preserving Memory: The Interplay between Cataracts and Dementia
Introduction
India is experiencing a rapid demographic transition, with projections indicating that by 2050, nearly 20% of the population—over 320 million individuals—will be aged 60 years and above¹. This aging shift has brought age-associated conditions such as visual impairment and dementia to the forefront of national health priorities. Cataract, the leading cause of blindness in India, accounts for over 60–80% of visual impairment cases among older adults². At the same time, dementia is emerging as a major public health concern, with an estimated 8.8 million Indians currently affected³.
The burden of visual impairment in India is substantial. According to the Longitudinal Ageing Study in India (LASI), approximately 34% of adults aged 45 years and older have distance vision impairment, while 43% experience near vision problems?. Cataracts remain the primary contributor, particularly among rural and low-income populations, where access to corrective surgery remains limited?. Despite advancements in surgical techniques and a growing number of cataract removal procedures performed annually, significant treatment gaps persist?.
Recent evidence suggests a strong association between visual impairment and cognitive decline, including dementia. In the LASI-DAD study, Indian adults with moderate to severe visual impairment demonstrated significantly lower performance across multiple cognitive domains, including memory, orientation, and executive functioning?. These findings are consistent with international studies, which have reported that individuals with visual impairment face a 1.3–2.0 times higher risk of developing dementia?.
Of particular interest is the emerging hypothesis that cataract surgery may mitigate this risk. Global data—including findings from the Adult Changes in Thought (ACT) study and large-scale meta-analyses—indicate that cataract extraction is associated with a 25–30% reduced risk of developing dementia?. The mechanisms proposed include improved sensory stimulation, increased mobility, better social engagement, and potential reversal of cortical atrophy linked to sensory deprivation¹?. Though similar data specific to the Indian population are limited, the public health implications are significant. Given that a large proportion of vision loss in India is preventable or treatable, cataract surgery may represent a low-cost, high-impact strategy to help preserve cognitive health in aging populations.
Despite the potential promise, current research in the Indian context remains sparse. Most available studies are cross-sectional in design, lack detailed longitudinal follow-up, and do not specifically assess dementia outcomes post-cataract surgery. Furthermore, socioeconomic, cultural, and healthcare access disparities unique to India complicate both diagnosis and management of visual and cognitive impairments¹¹.
Review of Literature
Cataract remains the leading cause of blindness and visual impairment in India. According to estimates from the National Programme for Control of Blindness and Visual Impairment (NPCBVI), cataracts account for over 66.2% of blindness and 80% of severe visual impairment in individuals aged 50 years and above.12 Data from the Rapid Assessment of Avoidable Blindness (RAAB) surveys in various Indian states, including Andhra Pradesh and Gujarat, consistently confirm this trend.13 Notably, the 2019 RAAB survey in Maharashtra reported that 61.6% of blindness in individuals aged ≥50 years was due to cataract.14
Despite the widespread availability of cataract surgery, challenges remain. Socioeconomic and geographic disparities continue to affect access to care. Cataract Surgical Rate (CSR) varies widely across states, with poorer access reported in rural and tribal regions.2 Women and individuals from lower-income households experience higher rates of cataract-related blindness, often due to delayed care-seeking and cultural barriers.15
The LASI study, covering over 72,000 individuals aged 45 and above, found that approximately 33.8% had distance visual impairment, and 43.0% had near vision impairment.4 While these impairments are not exclusively caused by cataracts, they are often closely linked—particularly among the elderly, where lens opacity is the dominant cause.16
India is currently home to more than 8.8 million people living with dementia, according to estimates derived from the LASI-DAD (Diagnostic Assessment of Dementia) sub-study. Dementia prevalence increases sharply with age, reaching 7.4% in adults aged 60 years and above and up to 24% in those aged ≥85 years.17
Studies show wide variation in prevalence due to differences in diagnostic tools, regional health disparities, and levels of public awareness. Community-based studies in both rural and urban populations have reported dementia prevalence ranging from 2% to 10%.18 In a study from rural northern India, dementia prevalence was found to be 6.0% among adults aged 60 and above, with significantly higher risk observed in women and individuals with no formal education.19
A key concern in India is the under diagnosis and poor recognition of dementia in both urban and rural settings. Cultural stigma, low levels of mental health literacy and inadequate geriatric care infrastructure contribute to this gap. As a result, the true burden of cognitive impairment is likely underreported.20
The co-existence of cataracts and cognitive impairment is common in India’s aging population, but few studies have examined them together. The LASI-DAD data provide early evidence of a strong association between visual impairment (often from cataracts) and cognitive deficits across memory, orientation, and executive function domains.17 These findings align with global evidence indicating that untreated visual impairment is associated with an elevated risk of developing dementia, independent of age, education, and comorbidities.21
Given the high and overlapping prevalence of cataracts and dementia in India, it is plausible that one may influence the progression or onset of the other. However, most existing literature in the Indian context is cross-sectional and lacks long-term follow-up to establish causal relationships.
Vision loss, particularly in later life, has been increasingly recognized as a potential contributor to cognitive decline and dementia. While vision impairment and cognitive impairment often co-occur due to shared aging processes (Figure 1), recent research suggests there may be both biological and psychosocial mechanisms that causally link the two. Understanding these pathways is critical, especially in countries like India where both conditions are prevalent but often underdiagnosed.
Figure 1: Mechanism Common to Dementia and Cataract
One of the most widely cited theories is the sensory deprivation hypothesis, which suggests that long-term loss of sensory input (e.g., from vision or hearing impairment) leads to decreased stimulation of the brain, ultimately resulting in structural and functional decline.22
Neuroimaging studies have demonstrated that individuals with untreated cataracts or other forms of visual loss show cortical thinning, particularly in areas associated with visual processing and cognition.23 For example, reduced activation in the occipital cortex and hippocampus—regions essential for memory and spatial orientation—has been observed in people with impaired visual acuity.24 A 2021 study by Whitson et al. found that participants with visual impairment had significantly smaller brain volumes and performed worse on memory tests, even after controlling for age and education.25
The cognitive load hypothesis proposes that when sensory systems are impaired, more cognitive resources are needed to process degraded input, leaving fewer resources for higher-order cognitive tasks.26 In older adults with vision loss, the brain may allocate excessive attention to interpreting unclear visual signals, thereby compromising working memory, reasoning, and executive function.27
This mechanism is supported by studies showing that visual impairment correlates with poor performance on attention- and processing speed-based cognitive tests, especially in early dementia stages.28
Visual impairment often leads to reduced mobility, withdrawal from social interactions, and increased dependence, all of which are known risk factors for cognitive decline.29 In India, where assistive infrastructure for the visually impaired is often lacking, these effects may be more pronounced.
Multiple cohort studies, including data from LASI-DAD, have shown that socially isolated individuals have a 40–50% higher risk of developing dementia.30 Visually impaired older adults are less likely to participate in cognitively stimulating activities such as reading, navigating new environments, or engaging in social gatherings.31 These limitations contribute to the “use it or lose it” paradigm, where underutilized cognitive networks deteriorate more rapidly.32
Vision impairment is strongly associated with depressive symptoms, which themselves are independent risk factors for cognitive decline.33 Depression is common in individuals with chronic visual conditions like cataract and age-related macular degeneration. In Indian studies, rates of depression among visually impaired older adults range from 30% to 45%, depending on severity and access to care.34
Depression may contribute to cognitive dysfunction via dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis, hippocampal atrophy, and increased levels of inflammatory cytokines—all of which are implicated in neurodegeneratio.35
Cataracts and dementia share several underlying biological mechanisms, particularly chronic oxidative stress and inflammation. Cataract formation results from protein aggregation and lens opacification due to oxidative damage, while similar mechanisms contribute to neuronal loss in Alzheimer's disease.36
Elevated markers such as C-reactive protein (CRP), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-α) have been associated with both conditions in aging populations.37 These shared pathways suggest a possible systemic link between visual decline and brain aging, beyond the direct sensory-cognitive interaction.
Emerging evidence suggests common vascular and genetic risk factors may predispose individuals to both cataracts and cognitive decline. Conditions like diabetes, hypertension, and atherosclerosis are strongly associated with both vision loss and dementia.38
Additionally, APOE-ε4, a genetic variant linked to Alzheimer's disease, has been associated with age-related cataract in some populations, although more research is needed to confirm this connection in the Indian context.39
Delirium and dementia are distinct yet interrelated neurocognitive disorders that commonly co-occur in older adults. Dementia is a progressive, chronic condition marked by gradual cognitive decline, while delirium is an acute, often reversible disturbance in attention and awareness, typically triggered by acute medical illness or stressors.40
The presence of dementia is one of the strongest risk factors for developing delirium. Studies show that individuals with dementia have a 2 to 5-fold increased risk of experiencing delirium during hospitalization.41 Moreover, delirium superimposed on dementia (DSD) is highly prevalent, affecting up to 89% of older adults with dementia in hospital settings.42 This combination complicates diagnosis and management, as the acute changes of delirium may be misattributed to chronic cognitive decline.
Importantly, emerging evidence suggests a bidirectional relationship between the two conditions. Not only does dementia increase the risk of delirium, but delirium itself may accelerate cognitive decline and potentially lead to new dementia diagnoses.43 A 2021 meta-analysis reported that older adults who experienced delirium had nearly 12-fold higher odds of developing dementia compared to controls (OR?=?11.9; 95% CI 7.3–19.6).44 Further, a prospective cohort study (DECIDE) found that even single episodes of delirium were associated with subsequent declines in MMSE scores and increased incidence of dementia, independent of baseline cognition.45
Pathophysiologically, both conditions share mechanisms such as neuroinflammation, oxidative stress, and cholinergic dysfunction, suggesting overlapping vulnerabilities.46 Clinically, delirium may serve as both a marker and a mediator of underlying neurodegeneration, highlighting its importance in dementia trajectories.47
Given the strong correlation, early recognition and prevention of delirium—particularly in patients with cognitive impairment—are critical. Interventions like the Hospital Elder Life Program (HELP) and caregiver-based tools such as PREDICT have shown promise in mitigating delirium risk.48
Cataract surgery is one of the most common and successful surgical procedures worldwide, primarily aimed at restoring visual function. Beyond improving vision, emerging evidence suggests that cataract surgery may also confer cognitive benefits, potentially delaying or reducing cognitive decline and dementia risk in older adults.49 This has important public health implications, particularly in aging populations burdened by both cataract and cognitive impairment.
Several longitudinal cohort studies from high-income countries have reported associations between cataract surgery and improved cognitive outcomes.
- Adult Changes in Thought (ACT) Study, USA: This prospective cohort study followed over 3,000 adults aged ≥65 years for up to 20 years. Participants who underwent cataract surgery exhibited a 30% lower risk of developing dementia compared to those with untreated cataracts.9 The study hypothesized that improved sensory input and increased social engagement post-surgery underlie this protective effect.
- Blue Mountains Eye Study, Australia: This population-based study demonstrated that cataract surgery was associated with slower cognitive decline over a 5-year period among older adults. Improved contrast sensitivity and visual acuity post-surgery correlated with better performance on memory and executive function tests.50
- Singapore Longitudinal Ageing Study: Cataract surgery was linked with better cognitive function, particularly in domains related to attention and visuospatial skills. The study emphasized the importance of early intervention before significant cognitive impairment develops.51
RCTs directly assessing cognitive outcomes following cataract surgery are rare, due to ethical and practical challenges in withholding surgery. However, some small-scale interventional studies provide preliminary evidence:
- A 2017 study by Harwood et al. demonstrated improvements in global cognitive scores measured by the Mini-Mental State Examination (MMSE) at 6 months post cataract surgery in older adults with mild cognitive impairment.52
- A pilot trial in the UK showed that patients receiving cataract surgery had improved executive function and processing speed 3 months after surgery compared to controls who had delayed surgery.53
Though limited in sample size and duration, these studies suggest cataract surgery may have short-term cognitive benefits, warranting larger and longer-term trials.
The cognitive improvements observed post-cataract surgery may be explained by several mechanisms:
- Enhanced Sensory Input: Restoration of visual acuity increases sensory stimulation to the brain, which can slow cortical atrophy linked to sensory deprivation.54
- Improved Mood and Social Engagement: Postoperative vision improvement often leads to increased social participation, physical activity, and reduced depressive symptoms—all protective factors against cognitive decline.31
- Neuroplasticity: Some studies propose that improved vision facilitates neural network reorganization, supporting cognitive resilience.55
There is a notable paucity of Indian studies specifically assessing cognitive outcomes post-cataract surgery. However, several indirect findings support potential benefits:
- The LASI highlights high prevalence of untreated cataract and its association with lower cognitive function.4
- Regional studies indicate that cataract surgery improves quality of life, mobility, and independence among older adults, factors linked to cognitive health.56
- Given the high cataract burden and growing dementia prevalence in India, integrating cognitive assessments into cataract care protocols may yield valuable insights and intervention opportunities.
- Most evidence derives from observational studies susceptible to confounding (e.g., healthier individuals more likely to undergo surgery).
- There is limited long-term follow-up assessing whether cognitive benefits persist or translate into reduced dementia incidence.
- Few studies include diverse populations or low-resource settings similar to India.
- Standardized cognitive outcome measures and large-scale RCTs are needed to strengthen causal inference.
Existing literature strongly suggests cataract surgery may offer cognitive benefits beyond vision restoration, potentially mitigating cognitive decline and dementia risk through multiple pathways. While global data are promising, further research—especially longitudinal and interventional studies in India—is essential to confirm these findings and inform integrated eye-brain health strategies.
Cataract surgery is generally considered a safe and effective intervention for restoring vision in older adults. However, patients with preexisting dementia represent a unique clinical subgroup that may face higher risks during the perioperative and postoperative periods. Given the rising prevalence of both cataract and dementia globally and in India, understanding the complications and challenges in this population is critical for optimizing care.
Multiple studies have documented that patients with dementia undergoing cataract surgery may experience different surgical outcomes compared to cognitively normal peers. Cognitive impairment can impact the ability to comply with preoperative instructions and postoperative care, potentially increasing complication risks.57
- A study by Lee et al. (2019) found that dementia patients had a slightly higher risk of postoperative delirium and required longer postoperative care and support.58
- In another cohort study, Katz et al. (2018) observed that individuals with dementia had increased rates of complications such as posterior capsule opacification (PCO) and secondary glaucoma following cataract surgery.59
General anesthesia or sedation is sometimes required for patients with advanced dementia who cannot cooperate during surgery. This introduces specific risks:
- Dementia patients are at higher risk for postoperative delirium and cognitive decline following anesthesia.60
- Regional anesthesia with minimal sedation is preferred when feasible to reduce these risks.61
- A systematic review by Culley et al. highlighted that anesthesia exposure might exacerbate existing cognitive impairment, although evidence specific to cataract surgery is limited.62
Common complications of cataract surgery include infection (endophthalmitis), inflammation, cystoid macular edema, and retinal detachment. In patients with dementia, complications may be more frequent or severe due to:
- Poor postoperative compliance: Difficulty in administering eye drops and attending follow-up appointments increases risks of infection and inflammation.63
- Increased falls risk: Visual rehabilitation is critical to reduce falls, but incomplete recovery or postoperative confusion can transiently elevate fall risk in dementia patients.64
- Behavioral issues: Agitation or inability to tolerate eye patching can complicate immediate postoperative care.65
A retrospective study by Wong et al. (2020) found a 20% higher rate of postoperative complications in patients with dementia, mostly related to poor wound healing and secondary glaucoma.66
While cataract surgery may improve cognitive function in some dementia patients by enhancing sensory input, surgery-related complications and hospitalizations can also trigger cognitive deterioration or delirium, especially in advanced dementia. This dual potential underscores the need for careful patient selection and tailored perioperative management.67
To reduce complications, several recommendations have emerged:
- Preoperative cognitive and functional assessment to stratify surgical risk and guide anesthesia choice.68
- Enhanced caregiver involvement to support medication adherence and postoperative monitoring.69
- Use of minimally invasive surgical techniques and regional anesthesia to reduce stress and recovery time.70
- Multidisciplinary teams involving ophthalmologists, geriatricians, and anesthesiologists to optimize outcomes.71
Indian literature on cataract surgery outcomes in dementia patients is limited but growing:
- A study in a tertiary care center in South India found that dementia patients had poorer visual outcomes due to delayed presentation and postoperative complications linked to poor compliance.72
- Cultural and infrastructural challenges exacerbate risks in rural areas, where caregiver support and follow-up services are limited.73
While cataract surgery can significantly improve quality of life, patients with preexisting dementia face higher risks of perioperative complications and postoperative challenges. Careful assessment, anesthesia planning, caregiver support, and tailored postoperative care are essential to minimize these risks and maximize benefits. More prospective studies, particularly from low- and middle-income countries including India, are needed to establish best practices.
India faces a growing burden of age-related cataract and dementia, both of which significantly impact quality of life and healthcare systems.74 Early intervention for cataract and integration of eye care with cognitive health services present a promising strategy to reduce disability and healthcare costs. This review highlights existing evidence on the public health impact and the need for integrated care models in India.
Cataract remains the leading cause of blindness in India, affecting approximately 8 million people, with many cases untreated due to limited access, socioeconomic barriers, and lack of awareness.75, 76 Dementia prevalence in India is estimated at 2.7% among adults over 60 years, with projections indicating a substantial increase due to population aging.77 Studies show a high co-occurrence of cataract and cognitive impairment, with vision loss linked to accelerated cognitive decline and reduced independence.78
Early detection and timely cataract surgery offer benefits beyond vision restoration. These include improved functional independence and reduced risk of falls, which contribute to maintaining both cognitive and physical health.79 Early cataract surgery has been associated with slower cognitive decline, emphasizing the need to reduce surgical backlogs and improve coverage.80 In contrast, delayed intervention increases the risk of irreversible disability, institutionalization, and increased healthcare costs.81 In the Indian context, delayed cataract surgery is common, especially in rural and marginalized populations, due to low awareness, affordability issues, and inadequate healthcare infrastructure.82
Integrated care approaches combining eye health, geriatric services, and cognitive assessment can optimize patient outcomes. The Longitudinal Aging Study in India (LASI) recommends embedding vision screening and cataract management into broader geriatric health programs to address multiple comorbidities concurrently. 83 Pilot projects integrating eye care with community health workers and primary care physicians have shown promise in improving early detection and referral rates for both cataract and cognitive impairment.84 Multidisciplinary collaboration involving ophthalmologists, neurologists, and mental health professionals facilitates comprehensive assessment and individualized care plans.85
Key barriers to integrated care in India include shortages of trained personnel, equipment, and infrastructure, particularly in rural areas.86 Low health literacy and stigma related to dementia further reduce healthcare-seeking behavior for cognitive symptoms. Fragmented care delivery, with poor coordination between specialties, limits continuity of care and follow-up. Additionally, high out-of-pocket expenses remain a significant barrier to access for low-income elderly populations.87
The National Programme for Health Care of the Elderly (NPHCE) includes provisions for eye health and mental health screening but requires stronger implementation at the grassroots level. NGOs and eye care systems such as the Aravind Eye Care System have pioneered scalable cataract surgery models demonstrating cost-effectiveness and significant social impact. Increasingly, there are calls to incorporate cognitive screening into routine eye care visits and to train ophthalmic personnel in recognizing early signs of dementia.88
Modeling studies suggest that scaling up cataract surgery coverage in India could avert millions of disability-adjusted life years (DALYs) and delay dementia onset in a significant fraction of the elderly population. Integrated care models improve patient satisfaction, reduce hospitalization rates, and lower healthcare costs through prevention and early intervention.89
India’s dual burden of cataract and dementia necessitates urgent public health action emphasizing early intervention and integrated care. Strengthening healthcare infrastructure, improving community awareness, and fostering multidisciplinary collaboration can substantially reduce the burden of visual and cognitive impairment, ultimately improving quality of life and reducing societal costs.90
Conclusion
Cataract and dementia represent two of the most significant and interrelated challenges facing India’s rapidly aging population. The epidemiological evidence underscores a high and growing burden of both conditions, with substantial overlap in older adults. Visual impairment due to cataract not only causes disability but also contributes to cognitive decline through complex biological mechanisms—including sensory deprivation, increased cognitive load, and shared pathophysiological pathways—as well as psychosocial factors such as social isolation and depression.
Emerging research highlights the potential cognitive benefits of timely cataract surgery, which may slow or partially reverse cognitive decline by restoring sensory input, improving mood, and facilitating social engagement. However, in patients with preexisting dementia, cataract surgery presents unique challenges, including increased risks of perioperative complications, postoperative delirium, and difficulties in adherence to postoperative care. These challenges necessitate careful patient assessment, tailored anesthesia and surgical approaches, and robust caregiver involvement to optimize outcomes.
From a public health perspective, the dual burden of cataract and dementia demands integrated, multidisciplinary care models in India. Early intervention through improved cataract detection and timely surgery can significantly reduce the progression of disability, enhance quality of life, and potentially delay dementia onset. However, barriers such as limited healthcare infrastructure, low awareness, socioeconomic constraints, and fragmented service delivery must be addressed. The integration of eye health with geriatric and cognitive care—leveraging community health workers and primary care platforms—offers a promising pathway to holistic management.
Policy frameworks like the National Programme for Health Care of the Elderly (NPHCE) provide a foundation, but scaling effective interventions requires concerted efforts in capacity building, public education, and system strengthening. Increasing cataract surgery coverage with attention to cognitive health, coupled with systematic screening for dementia in ophthalmic settings, can foster earlier diagnosis and intervention, ultimately reducing the national burden of blindness and cognitive impairment.
In conclusion, addressing cataract and dementia in tandem through early, integrated, and patient-centered care strategies holds significant promise for improving health outcomes among India’s elderly. Continued research, especially longitudinal and interventional studies in Indian populations, is essential to refine these strategies and inform evidence-based policies. Such efforts will be pivotal in mitigating the social, economic, and healthcare impacts of these interlinked conditions in India’s aging society.
References
1. United Nations Department of Economic and Social Affairs. World Population Prospects 2022.
2. Murthy GVS, et al. Current estimates of blindness and visual impairment in India. Br J Ophthalmol. 2005;89(3):257–60.
3. Nichols E, et al. Global burden of dementia, 1990–2016: a systematic analysis. Lancet Neurol. 2019;18(1):88–106.
4. Arokiasamy, P., Bloom, D. E., Lee, J., Feeney, K., & Ozolins, M. (2020). Longitudinal Ageing Study in India (LASI), Wave 1, 2017–18, India Report. International Institute for Population Sciences (IIPS). https://www.iipsindia.ac.in/lasi
5. Dandona L, Dandona R. Review of findings of the Andhra Pradesh Eye Disease Study. Community Eye Health. 2003;16(48):54–5.
Please view attached pdf to view complete references
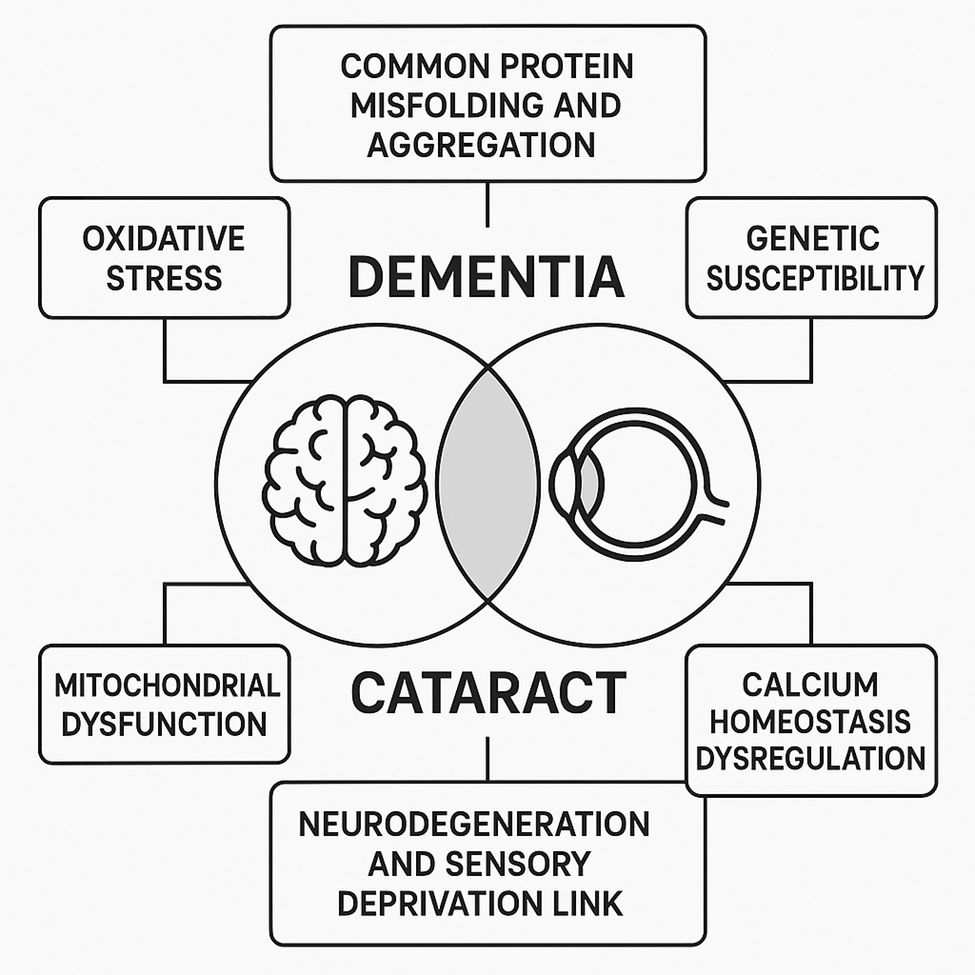
Figure 1