Exclusive Radiotherapy in the Management of Mandibular Solitary Plasmacytoma: A Rare Case in an Elderly Patient
Exclusive Radiotherapy in the Management of Mandibular Solitary Plasmacytoma: A Rare Case in an Elderly Patient
Dr. Mohammed Sameer 1, Dr. Vipul Goyal 2*
1,2. M.ch Surgical Oncology Senior Resident, Cochin Cancer Research Centre, Ernakulam, Kerala, India.
*Correspondence to: Dr. Vipul Goyal, M.ch Surgical Oncology Senior Resident, Cochin Cancer Research Centre, Ernakulam, Kerala, India.
Copyright.
© 2025 Dr. Vipul Goyal This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 Aug 2025
Published: 21 Aug 2025
DOI: https://doi.org/10.5281/zenodo.17596651
Abstract
Background: Solitary plasmacytoma (SP) is a rare plasma cell neoplasm characterized by a localized proliferation of monoclonal plasma cells without systemic involvement. Mandibular localization is exceptional and presents a diagnostic and therapeutic challenge due to the anatomical complexity and risk of progression to multiple myeloma (MM).
Objective: This case report aims to explore the effectiveness of exclusive radiotherapy in treating an unresected solitary bone plasmacytoma (SBP) of the mandible in an adult patient.
Case Presentation: We report the case of an 80-year-old man with a solitary bone plasmacytoma (SBP) of the mandible, initially presenting as dental mobility and mandibular swelling. Imaging revealed a left parasymphyseal mandibular lesion initially suspected to be osteomyelitis. Histopathological analysis confirmed a mature plasma cell neoplasm. Extensive staging, including bone marrow biopsy and FDG-PET, confirmed the solitary nature of the lesion. Given the patient's refusal of surgery, exclusive conformational radiotherapy was delivered to a total dose of 46 Gy in 23 fractions, with good tolerance. Post-treatment evaluation showed significant tumor regression and stable clinical condition.
Discussion: Mandibular plasmacytomas are extremely rare and may mimic inflammatory or infectious lesions. Diagnosis relies on imaging, histopathology, and exclusion of systemic disease. Radiotherapy remains the cornerstone of treatment, achieving high local control rates. However, long-term follow-up is crucial due to the significant risk of progression to MM.
Conclusion: This case highlights the effectiveness of exclusive radiotherapy in the management of solitary mandibular plasmacytoma and underscores the importance of thorough diagnostic workup and multidisciplinary evaluation. Further studies are needed to optimize therapeutic strategies in such rare and complex presentations.
Exclusive Radiotherapy in the Management of Mandibular Solitary Plasmacytoma: A Rare Case in an Elderly Patient
Introduction
Solitary plasmacytoma (SP) is histologically characterized by a localized accumulation of monoclonal neoplastic plasma cells, without signs of systemic plasma cell proliferation, absence of bone marrow dissemination, and a unique lesion. It is a rare form of plasma cell neoplasm, accounting for 5 to 10% of all plasma cell neoplasms according to the literature (1,2). It can be classified into two groups based on its location: solitary bone plasmacytoma (SBP) or intramedullary plasmacytoma, and extramedullary plasmacytoma (EMP) (1,3). The bone forms are the most common and primarily affect the vertebrae, but also the ribs, clavicles, sternum, and long bones (4). Mandibular involvement has been rarely described in the literature.
The frequent progression of solitary bone plasmacytoma to multiple myeloma, reported in 55% of cases in the literature, continues to raise questions about its nosological authenticity (5).
Based on a case of solitary bone plasmacytoma of the mandible, complemented by a literature review, we aim to revisit the diagnostic, therapeutic, and evolutionary aspects of this condition
Objective
The aim of this case report is to examine the role of exclusive radiotherapy in the curative treatment of an unresected mandibular solitary plasmocytoma in an elderly patient.
Case Presentation
Our patient is an 80-year-old man, married, and the father of one son who died in a road traffic accident. He has a history of hypertension and diabetes, both well controlled with medical treatment. He was admitted to our department for the management of a solitary plasmacytoma of the mandible. The disease appears to have started approximately three months prior to admission, with the onset of localized swelling and dental mobility, prompting him to consult his dentist. A panoramic dental X-ray and a CT scan of the facial bones were performed, revealing a semi-recent left parasymphyseal mandibular fracture with significant mandibular osteocondensation and an associated anterior periosteal reaction. These findings were highly suggestive of chronic osteomyelitis complicating the aforementioned fracture. There was also evidence of phlegmon involving the soft tissues surrounding the left mandibular body in the area of the fracture, without any clearly organized collection.
Figure 1: Left mandibular osteolytic lesion on orthopantomogram in a patient with plasmacytoma.
Figure 2: CT scan slice showing osteolysis of the left mandibular ramus caused by the solitary plasmacytoma.
The patient was then referred to an Ear-Nose-Throat (ENT) Doctor who completed the assessment with an Magnetic Resonance Imaging (MRI) of the facial bones. The imaging revealed a fracture of the horizontal branch of the left mandible, with significant surrounding soft tissue infiltration and moderate enhancement, findings that could be compatible with osteomyelitis. No true mass effect or cervical lymphadenopathy was noted.
Figure 3 : Axial MRI images: T2-weighted (A) and T1-weighted (B) sequences showing a left mandibular lesion with high signal intensity, suggestive of a solitary plasmacytoma.
The ENT Doctor subsequently performed a surgical biopsy of the left mandibular stump, which revealed a mature plasma cell neoplasm with lambda and IgM monotypy. The cells were CD138 positive and CD20 negative, with a Ki-67 index of 1–2%. Immunofixation showed the presence of two monoclonal immunoglobulins (IgM kappa and IgM lambda). The biological workup revealed no hypercalcemia or renal dysfunction. Bone marrow analysis showed a polymorphic marrow without cytological evidence of plasma cell tumor infiltration.
As part of the staging workup, an FDG-PET scan confirmed that the mandibular plasmacytic lesion was solitary, with a few benign-appearing lymph nodes in the cervico-thoracic region. The case was discussed in a multidisciplinary hematology meeting, and given the patient's refusal of surgery, the decision was made to proceed with exclusive radiotherapy.
Figure 4: PET-CT scan slice showing hypermetabolism corresponding to the left mandibular fracture involvement, with a SUVmax of 8.6 compared to a hepatic reference of 3.6.
Upon admission to our department, the clinical examination found a patient in good general condition (Performance Status 1), asymptomatic in terms of pain (Visual Analog Scale, VAS score 0), weighing 85 kg for a height of 1.80 m.
The locoregional examination revealed hypoesthesia in the territory of the left mandibular branch (V3), along with a slight leftward deviation of the mouth.
There was also a swelling of the lower left mandibular region, in the context of prior dental avulsions (teeth 27 and 34), with ongoing healing progressing well.
A planning CT scan was then performed using a five-point thermoplastic mask and knee supports to ensure immobilization. Alignment was done using wall lasers positioned at the level of the tragus. The images were transferred from the treatment planning system (TPS) to the contouring console.
The planned treatment consisted of normofractionated conformational radiotherapy, with a total dose of 46 Gy delivered in 23 fractions (five sessions per week), targeting exclusively the mandibular tumor mass, without irradiation of lymph node areas.
Target volume delineation included:
- GTV-T: the visible tumor mass
- CTV-T: obtained by adding a 5 mm margin around the GTV-T
- PTV-T: defined by adding a 10 mm margin around the CTV-T
Regarding treatment delivery, helical tomotherapy was selected, using a single arc to deliver the dose.
During the course of treatment, the patient developed grade 2 radiomucositis (CTCAE), managed with mouthwashes containing sodium bicarbonate, xylocaine, and corticosteroids, as well as grade 2 radiodermatitis, treated with emollients and adhesive dressings, both of which improved with appropriate care.
At the post-radiotherapy follow-up visit, a significant regression of the tumor mass was noted. However, the hypoesthesia in the V3 territory persisted. An MRI was scheduled to better evaluate the tumor response to radiotherapy.
Discussion
Plasma cell neoplasms account for 1 to 2% of all human malignancies. Several clinical forms exist, among which solitary plasmacytoma represents less than 10% of these proliferations. It was first described by Schridde in 1905 (6,7). Solitary plasmacytoma is classified into two groups. The most common is solitary bone plasmacytoma (SBP), which frequently evolves into a multiple form. It commonly affects the axial skeleton and rarely involves the jaws. When it does, only about 4.4% of SBPs occur in the mandible, most often in areas rich in bone marrow such as the body, angle, and ramus of the mandible8.
The second group is solitary extramedullary plasmacytoma (SEP) (9).
The etiology of solitary plasmacytoma remains uncertain, but several hypotheses have been proposed, involving the role of radiation exposure, chemical agents, viral infections, and genetic factors. Cytogenetic studies have identified losses of chromosomes 13, 1p, and 14q, and gains of chromosomes 19p, 9q, and 1q. Interleukin-6 is considered a key growth factor in the pathogenesis of this condition (10).
SBP most often occurs in patients aged 50 to 80 years, with a mean age of onset around 60. It is rare before the age of 4011. The condition is more frequent in men, with a reported male-to-female ratio of 2:112.
The clinical presentation of solitary plasmacytoma of the mandible (SPM) is not specific; facial swelling, dental mobility, and sensory disturbances are the most frequent clinical signs. In rare cases, a solitary plasmacytoma of the mandible may be discovered during a pathological fracture, post-extraction bleeding, or a dental joint disorder in the case of condylar localization (13).
Malignant plasma cells produce cytokines and release an osteoclast-activating factor that stimulates osteoclasts to resorb bone; consequently, on radiographic examination, they appear as well-defined osteolytic lesions with either unilocular or multilocular radiolucency (10,14). According to Lae et al., three radiographic patterns have been described in SBP: multilocular 'soap bubble' lesions, unilocular radiolucency (as seen in our patient) with a cystic appearance, and poorly defined destructive bone resorption (15). CT helps to refine the radiological image and assess the extension toward cortical and soft tissues. MRI remains a valuable imaging modality for detecting bone-involved plasmacytomas, assessing soft tissue involvement and bone marrow infiltration, and evaluating disease throughout the body. Solitary plasmacytomas show low signal intensity on T1-weighted images and high signal intensity on T2-weighted images, with homogeneous enhancement after gadolinium contrast injection (16).
In our case, there were signs of periosteal reaction with cortical destruction, potentially extending widely into the surrounding tissues.
Under the microscope, plasma cells exhibit varying degrees of differentiation within a sparsely cellular stroma. Sukpanichnant et al. classified plasmacytomas into mild, moderate, and severe dysplasia based on the degree of plasma cell differentiation (19). Nuclei may be binucleated. The spherical nuclei are eccentrically located and display regular or irregular chromatin margination, often in a cartwheel pattern (18). Occasionally, the chromatin appears coarsely clumped, showing a clock-face configuration. The cells present a pale, globular perinuclear cytoplasmic area known as a hof. Pseudoangiomatous areas, multinucleated giant cells, amyloid deposition, and myxoid changes may also be observed in some cases. Plasma cells may contain intracytoplasmic inclusions (Russell bodies) and intranuclear inclusions known as Dutcher bodies. Immature plasma cells have larger or more irregular nuclei, less condensed chromatin, and may display prominent nucleoli. These immature cells are larger and more pleomorphic, with abundant, mildly basophilic cytoplasm (10).
The neoplastic process is secretory in approximately 99% of cases, producing monoclonal immunoglobulins of either light or heavy chains, which can be detected in the serum or urine (15). In accordance with the literature, the present case revealed elevated serum lambda light chains, exceeding the normal range. To diagnose a case of solitary bone plasmacytoma (SBP) and to exclude multiple myeloma (MM), thorough clinical investigations are required, including skeletal radiological survey, bone marrow aspiration, complete blood count, serum calcium levels, and renal function tests (15). Specific diagnostic criteria for SBP were proposed by Bataille and Sany (20)[Table 1].
The present case meets all of the aforementioned criteria. In addition to laboratory investigations, determining monoclonal restriction to either kappa or lambda light chains is a crucial approach in the evaluation of suspected plasmacytoma.
Table 1: Specific Diagnostic Criteria for Solitary Bone Plasmacytoma (SBP)
From a therapeutic perspective, surgical treatment may be considered for diagnostic purposes, in the presence of neurological complications such as spinal cord compression, or to treat or prevent a pathological fracture in bone weakened by tumor-induced osteolysis. In the specific case of mandibular involvement, surgical intervention is feasible in the vast majority of situations.
Complete resection may be indicated for peripheral, easily accessible lesions; however, it should not be mutilating, especially since radiotherapy offers comparable efficacy while allowing better preservation of function (5,6,21,22)
Moreover, the radiosensitivity and radiocurability of solitary bone plasmacytoma have been documented for over half a century (20, 23). Radiotherapy is considered the standard treatment for solitary bone plasmacytoma. When administered at optimal doses of 40 to 50 Gy, it provides a local control rate exceeding 90%, with excellent tolerance and rapid, durable pain relief.
A dose–response effect was reported by Mendenhall et al.(24), who observed a 94% local control rate at doses above 40 Gy, compared to 69% at lower doses. Similarly, Frassica et al.(25), in a series of 46 patients, reported a 15.6% local failure rate when the radiotherapy dose was below 45 Gy, while the local control rate was 100% with higher doses.
The addition of chemotherapy is not recommended, as it has not been shown to improve outcomes in terms of recurrence or progression to multiple myeloma (4, 5).
Predictive factors for local recurrence appear to include, in addition to insufficient radiotherapy doses, the anatomical location of the solitary bone plasmacytoma — with spinal or pelvic lesions being more difficult to manage than peripheral ones — the persistent presence of monoclonal protein after treatment, as well as tumor size (5)
The median survival rate of solitary plasmacytoma is longer than that of multiple myeloma due to the localized nature of the disease. However, clinical remission remains rare (26). SBPs carry a high risk of progression to multiple myeloma (65% to 84% at 10 years and nearly 100% at 15 years), whereas SEPs have a lower risk of progression (10% to 30% at 10 years) but a higher risk of local recurrence (27). Scientific data suggest that patients with an SBP larger than 4 to 5 cm are at increased risk of developing multiple myeloma (28).
Due to the progressive nature of SBP and the extended period (6 to 8 months) required to achieve maximal radiotherapy response, periodic monitoring is essential. A complete blood count, serum biochemistry (calcium and creatinine), and systematic evaluation of potential biomarkers such as persistent M-protein, clonal expansion of free light chains (FLC), and the presence of clonal plasma cells are standard practices (10). PET/CT, when available, can be particularly useful for follow-up in skeletal studies
Conclusion
Solitary plasmacytoma of the mandible is a rare entity, often difficult to diagnose and manage due to its potential for local aggressiveness and progression to multiple myeloma. Through this case, we highlight the efficacy of exclusive radiotherapy in achieving local control of the disease, even in anatomically complex locations such as the mandible. A thorough diagnostic evaluation, precise treatment planning, and close post-treatment monitoring remain essential. Further studies and larger case series are required to refine therapeutic strategies, particularly for aggressive or atypical forms. This work contributes to the literature supporting radiotherapy as an effective conservative treatment in selected cases
References
1. Dimopoulos MA, Moulopoulos LA, Maniatis A, Alexanian R. Solitary plasmacytoma of bone and asymptomatic multiple myeloma. Blood. 2000 Sep 15;96(6):2037-44. PMID: 10979944.
2 - Wiltshaw E. The natural history of extramedullary plasmacytoma and its relation to solitary myeloma of bone and myelomatosis. Medicine (Baltimore). 1976 May;55(3):217-38. doi: 10.1097/00005792-197605000-00002. PMID: 1272069.
3 - Frizzera G. Castleman's disease and related disorders. Semin Diagn Pathol. 1988 Nov;5(4):346-64. PMID: 2464187.
4 - Facon T, Yacoub-Agha I, Leleu X. Myélome multiple. Encycl. Med. Chir. (Elsevier), Hématologie, 13-014-E-10, 2003, 15 p
5 - Kochbati L, Ben Romdhane NK, Mrad K, Nasr C, Ben Salah DE, Ben Romdhane K, Maalej M. Solitary bone plasmocytoma: treatment and outcome features. Cancer Radiother. 2004 Apr;8(2):70-4. English, French. doi: 10.1016/j.canrad.2003.11.003. PMID: 15063873.
6 - Mendenhall WM, Mendenhall C, Mendenhall NP. Solitary plasmacytoma of bone and soft tissues. Am J Otolaryngol 2003; 24:395–9.
7 - S Chittemsetti VR Guttikonda T Sravya PK Manchikatla Plasmocytome solitaire de la mandibule : une entité rareJ Oral Maxillofac Pathol20192311369
8 - Seoane, J., Aguirre-Urizar, J. M., Esparza-Gómez, G., Suárez-Cunqueiro, M., Campos-Trapero, J., & Pomareda, M. (2003). The spectrum of plasma cell neoplasia in oral pathology. Medicina oral: organo oficial de la Sociedad Espanola de
9 - RW Tsang BA Campbell GS Goda CR Kelsey YM Kirova RR Parikh Radiothérapie pour le plasmocytome solitaire et le myélome multiple : lignes directrices de l'International Lymphoma Radiation Oncology GroupInt J Radiation Oncol Biol Phys20181014794808
10 - Rao K, Priya NS, Umadevi HS, Smitha T, Reshma V, Grace Shebha A. Plasmocytome osseux solitaire du maxillaire – Un rapport de cas rare Int J Clin Dent Sci. 2011;2:37–40
11 - Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod., 83 (2) (Feb. 1997), pp. 265-271, 10.1016/s1079-2104(97)90015-9
12 - E. M. Canger, P. Çelenk, A. Alkan, and Ö. Günhan, “Mandibular involvement of solitary plasmocytoma: a case report,” Med. Oral Patol. Oral Cir. Bucal., p. 3.
13 - “Florencio M, Jose L, Gil-Diez, Campano F.J, Jose R, Del Hoyo A. Mandibular lesion as the first evidence of Multiple Myeloma. J. Craniomaxillofac. Surg. 1989;17:315-317”.
14 - Singh A, Singh V, Sharma N. Plasmocytome solitaire de la mandibule : rapport de cas rare. Int J Med Dent Sci. 2012 ; 1 : 28–32
15 - Lae ME, Vencio EF, Inwards CY, Unni KK, Nascimento AG. Myeloma of the jaw bones: a clinicopathologic study of 33 cases. Head Neck. 2003 May;25(5):373-81. doi: 10.1002/hed.10210. PMID: 12692874.
16 - Pham, A., & Mahindra, A. (2019). Solitary plasmacytoma: a review of diagnosis and management. Current hematologic malignancy reports, 14, 63-69.
17 - Murat Canger, E., Çelenk, P., Alkan, A., & Günhan, Ö. (2007). Mandibular involvement of solitary plasmocytoma: a case report. Medicina Oral, Patología Oral y Cirugía Bucal (Internet), 12(1), 07-09.
18 - Valetti, C., Grossi, C. E., Milstein, C., & Sitia, R. (1991). Russell bodies: a general response of secretory cells to synthesis of a mutant immunoglobulin which can neither exit from, nor be degraded in, the endoplasmic reticulum. Journal of Cell Biology, 115(4), 983-994.
19 - Sukpanichnant S, Cousar JB, Leelasiri A, Graber SE, Greer JP, Collins RD. Diagnostic criteria and histologic grading in multiple myeloma: histologic and immunohistologic analysis of 176 cases with clinical correlation. Hum Pathol. 1994 Mar;25(3):308-18. doi: 10.1016/0046-8177(94)90204-6. PMID: 8150462.
20 - Bataille R, Sany J. Solitary myeloma: clinical and prognostic features of a review of 114 cases. Cancer. 1981 Aug 1;48(3):845-51. doi: 10.1002/1097-0142(19810801)48:3<845::aid-cncr2820480330>3.0.co;2-e. PMID: 7248911.
21 - Bencheikh R, Benhammou A, Rabeh G, Benbouzid MA, Boulaich M, Essakali L, Kzadri M. Plasmocytome solitaire osseux de la mandibule [Solitary bony plasmocytoma of the mandible]. Rev Stomatol Chir Maxillofac. 2007 Apr;108(2):135-8. French. doi: 10.1016/j.stomax.2006.05.004. Epub 2007 Mar 9. PMID: 17350056.
22- Moukhlissi, M., Bouamama, I., Bouchbika, Z., Benchekroun, N., & Benider, A. (2011). Plasmocytome solitaire osseux. Cancer/Radiothérapie, 15(6-7), 633.
23 - Maalej M, Moalla M. Plasmocytomes solitaires osseux : problèmes nosologiques et thérapeutiques. Tunis Med 1989;67:661–4.
24 - Mendenhall CM, Thar TL, Million RR. Solitary plasmocytoma of bone and soft tissue. Int J Radiat Oncol Biol Phys 1980;6:1497–501
25 - Frassica DA, Frassica FJ, Schray MF, Sim FH, Kyle RA. Solitary plasmocytoma of bone: Mayo Clinic experience. Int J Radiat Oncol Biol Phys 1989;16:43–8.
26 - Suryavanshi H, Patankar S, Dhumal S, Choudhari S. Solitary plasmacytoma of jaw bone: A case report and systematic review of fifty cases from literature. J Oral Maxillofac Pathol. 2021 Jan-Apr;25(1):205. doi: 10.4103/jomfp.JOMFP_251_20. Epub 2021 May 14. PMID: 34349446; PMCID: PMC8272505.
27 - Solitary plasmacytomas: outcome and prognostic factors after definitive radiation therapy. Cancer. 2011;117(19):4468–4474. doi: 10.1002/cncr.26031
28 - Tsang RW, Gospodarowicz MK, Pintilie M, Bezjak A, Wells W, Hodgson DC, Stewart AK. Solitary plasmacytoma treated with radiotherapy: impact of tumor size on outcome. Int J Radiat Oncol Biol Phys. 2001 May 1;50(1):113-20. doi: 10.1016/s0360-3016(00)01572-8. PMID: 11316553..
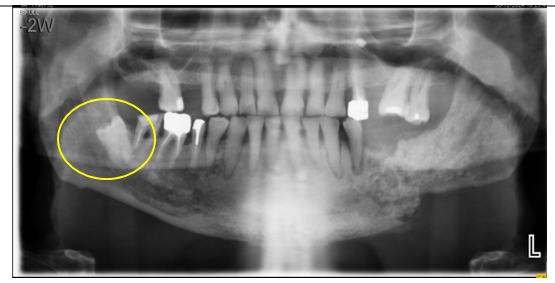
Figure 1
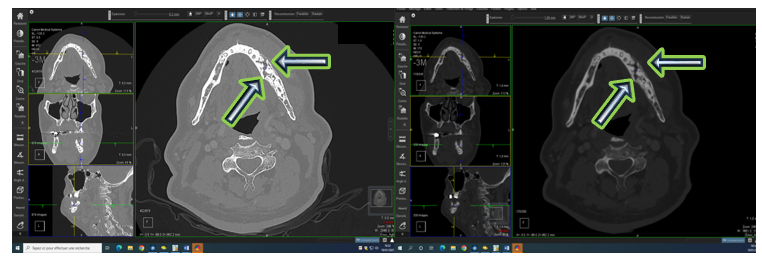
Figure 2
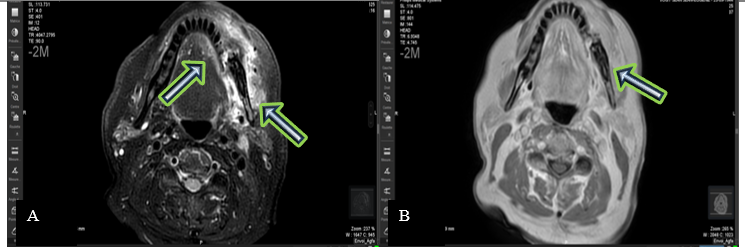
Figure 3
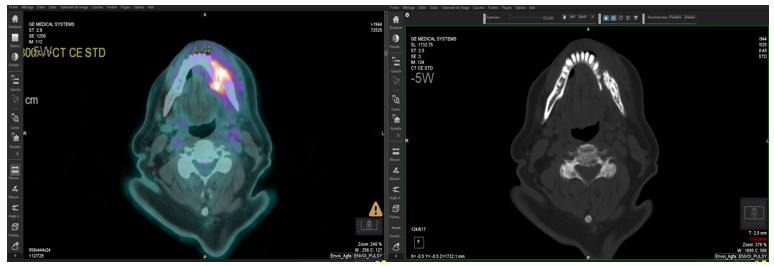
Figure 4
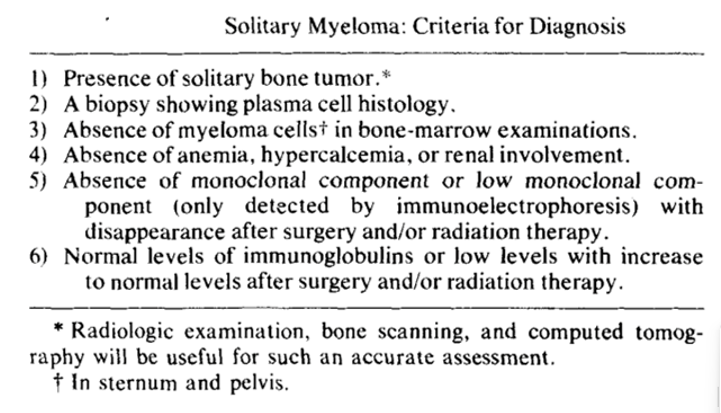
Figure 5