Our Experience of Bipolar Latissmus Dorsi Transfer for Elbow Flexion in Brachial Plexus Injuries
Our Experience of Bipolar Latissmus Dorsi Transfer for Elbow Flexion in Brachial Plexus Injuries
Dr. Hassan Tahir1*, Dr. Aimen qavi2, Dr. Asma Sarfaraz3, Dr. Rabia Anwar4, Dr. Obaid ur Rahman5
*Correspondence to: Dr. Hassan Tahir, Pakistan.
Copyright.
© 2025 Dr. Hassan Tahir This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 Aug 2025
Published: 29 Aug 2025
DOI: https://doi.org/10.5281/zenodo.17038827
Abstract
Objective: Upper extremity functional reconstruction after brachial plexus injury is a challenging task for a reconstructive surgeon. Patients experiencing brachial plexus injuries bare wearisome economical and social burden. A number of reconstructive options are described for restoration of elbow flexion. We aim to share our experience of elbow flexion reconstruction with pedicled bipolar Latissimus dorsi flap at single plastic and reconstructive surgery center.
Methods: During the time period of 4 years i.e., January 2019 to December 2022, 12 patients underwent elbow flexion reconstruction with bipolar latissimus dorsi flap after brachial plexus injuries. All procedures were planned and performed after serial clinical examinations and EMG-NCS studies. Post operatively patients were followed for routine checkup and physiotherapy.
Results: Among the patients undergoing elbow flexion reconstruction, 11 patients were male and one female patient. Average age was 25.66 (range 5-50 years). Average time elapsed since the time of injury was 12 months in adult population and 6.66 years in pediatric population. All patients gained MRC grade for elbow flexion (M4) and average range of elbow flexion was 120° degrees.
Conclusion: Latissimus dorsi is a useful option for elbow flexion reconstruction. Excellent range of motion and MRC (medical research council) grades of muscle strength can be achieved.
Keywords: Brachial plexus injury, Obstetric brachial plexus injury, elbow flexion, bipolar latissimus dorsi transfer.
Our Experience of Bipolar Latissmus Dorsi Transfer for Elbow Flexion in Brachial Plexus Injuries
Introduction
Brachial Plexus injuries are commonly encountered after a high velocity road traffic accident [1-6]. Most commonly affected injury pattern is the C5 to T1 (75%) C5-C6 root injuries (20-25%) and C8-T1 root injury being the least commonly affected (2-3.5%) [7]. In other cases, lower trunks i.e., C8 – T1 or pan plexus injuries are encountered. Upper extremity functional reconstruction after brachial plexus injury is a challenging task for a reconstructive surgeon. Patients experiencing brachial plexus injuries bare wearisome economical and social burden. Not only the patient but the family suffers until the patient is able to perform essential tasks. Early reconstructive options include nerve repair and nerve transfers (8). Later on elbow flexion restoration can be done via tendon transfers (9). Tendon transfer can be done primarily as in cases with late presentations or as a secondary procedure (failed primary nerve repair, suboptimal results of nerve transfers).These transfers can be pedicled or as a free functioning muscle transfer. Among the reconstructive options described, pedicled options include triceps to biceps transfer, steindlers flexoplasty, unipolar/bipolar pectoralis major transfer and unipolar/bipolar latissimus dorsi transfer (10, 11, 12, 13). Unipolar transfer was described in 1955 by Schottstaedt et al. and bipolar transfer was described in 1973 by Zancolli and Mitre. Of these bipolar transfer is a reliable option when available. It provides a good motor function both in means of power as well as in means of range of motion. In brachial plexus injuries bipolar latissimus dorsi can be reliably transferred for elbow flexion reconstruction. We aim to introduce our modification of latissimus dorsi wrap around technique.
Methodology
This study was conducted during the time period of 4 years i.e., January 2019 to December 2022, at the Department of Plastic and Reconstructive surgery, Liaquat National Hospital, Karachi, Pakistan. Patients presenting with brachial plexus injuries with functional latissimus dorsi were included. Patients with pan plexus injuries or those with non-functioning latissimus dorsi were excluded from the study. Twelve patients underwent elbow flexion reconstruction with bipolar latissimus dorsi flap after brachial plexus injuries. All muscle flaps were harvested in a routine manner in a lateral decubitus position, bean bag placed under the torso and an axillary roll to avoid any chance of compression of the axillary nerve. Markings are done with identification of the landmarks and the incision is marked. Appropriate incision is given on the ipsilateral side of the back of which elbow flexion is to be restored. Skin flaps are raised separating the muscle from the overlying subcutaneous tissue of the back, identifying the midline, the posterior axillary fold i.e., the lateral border of the muscle, the superior attachment (the inferior angle of scapula) and the inferior attachment (the iliac crest). Prior to diving the attachments the muscle was marked with sutures at 5cm distance to maintain the resting muscle tension. Flap was elevated from the underlying tissue and rolled. A pocket was created in the infra-clavicular region and coracoid process was identified and dissected. A subperiosteal dissection was done to create a space around the radius to wrap the muscle around it. The muscle was retrieved in the respective limb at the level of anti-cubital fossa (fig 1). New origin was secured at the coracoid process with ethibond 2-0. The insertion was secured at the radius. Post operatively the limb was kept immobilized in a splint with elbow at 90° and arm in a sling with abduction pillow. Active flexion within splint was allowed after 4 weeks. Splint was removed at 9 weeks and active elbow extension was began (15-20° per week). All procedures were planned and performed after serial clinical examinations and EMG-NCS studies. Post operatively patients were followed for routine checkup and physiotherapy. All data was collected on a routine OPD audit proforma & operative notes, relevant pictures and videos were taken after taking written and informed consent from patients, keeping patient identity and details confidential.
Figure 1- Intraoperative photographs of bipolar Latissimus dorsi transfer. a) Demonstrating tubed muscle, b) showing tubed flap transferred to the proximal and distal fixation sites.
Results
A total of twelve patients underwent elbow flexion restoration with bipolar latissimus dorsi transfer. Pediatric population comprised of 25% (3 patients), presenting with obstetric brachial plexus injury. Rest of the population (75%) were adult patients who sustained brachial plexus injury after a road traffic accident (7 patients), gunshot injury (1 patient) and fall from height (1 patient). Mean age in our study was 25.66 (range 5-50 years). Right upper extremity was involved in the majority of the patients (66.66%). All patients underwent detailed preoperative clinical examination and diagnostic EMG-NCS for confirmation. Level of injury as determined on imaging and electrophysiological examination showed evidence of pre-ganglionic injury in 9 patients (including two with obstetric brachial plexus injury) and post-ganglionic injury in 3 patients (including one with obstetric brachial plexus injury). Average time elapsed between time of injury in adult population was around 12 months and in pediatric population was 6.66 years. All patients had preoperative elbow flexion range of 10-15 degrees. All patients achieved power of M4 on MRC scale and elbow flexion up to 130° (range 100-130°) (fig 2). Mean time to return to work was 6.41 months.
Table 1 - Demographics of the patients along with mode of injury and pre-operative & post-operative flexion power.
|
S.No |
Gender |
Age (Yrs.) |
Involved extremity |
Other deficits |
Etiology |
Pre-operative Flexion Power |
Post -operative Flexion Power |
Time to return to work (months) |
|
1 |
Male |
22 |
right |
No |
Brachial Plexus injury (fall from height) |
M1 |
M4 |
6 |
|
2 |
Male |
32 |
right |
No |
Brachial Plexus injury |
M1 |
M4 |
5 |
|
3 |
Male |
40 |
right |
No |
Brachial Plexus injury |
M3 |
M4 |
11 |
|
4 |
Male |
20 |
right |
yes |
Brachial Plexus injury |
M0 |
M4 |
6 |
|
5 |
Male |
35 |
Left |
No |
Brachial Plexus injury |
M3 |
M4 |
5 |
|
6 |
Female |
8 |
Left |
yes |
Obstetric Brachial Plexus injury |
M0 |
M4 |
6 |
|
7 |
Male |
5 |
Left |
yes |
Obstetric Brachial Plexus injury |
M1 |
M4 |
7 |
|
8 |
Male |
7 |
right |
No |
Obstetric Brachial Plexus injury |
M1 |
M4 |
3 |
|
9 |
Male |
28 |
right |
No |
Brachial Plexus injury |
M2 |
M4 |
4 |
|
10 |
Male |
50 |
right |
No |
Brachial Plexus injury |
M3 |
M4 |
8 |
|
11 |
Male |
18 |
Left |
yes |
Brachial Plexus injury |
M1 |
M4 |
5 |
|
12 |
Male |
45 |
right |
No |
Brachial Plexus injury (gunshot injury) |
M3 |
M4 |
11 |
Figure 2- Demonstrating 6-months post-operative function of an eight year old girl after restoration of elbow flexion with bipolar latissimus dorsi transfer.
Discussion
Patients with brachial plexus injury may have varying deficits, involving shoulder, elbow and hand/wrist. Of these three joints most intricate functions are carried out by hand. An operational elbow with good mobility and stability is of outmost importance for a person to perform his routine activities (eating, personal hygiene, social interaction and professional activities) (16, 17). Elbow with a good strength and flexion has been defined in a number of studies, concluding that a useful function can be achieved with a strength of ≥ M4 and elbow flexion of 90-100° (18, 19). Elbow flexion reconstruction can be achieved by nerve transfers (8) in early presentation after brachial plexus injury, spinal accessory nerve transfer to musculocutaneous nerve, intercostal nerve transfer to musculocutaneous nerve, and Oberlin transfer. In case of late presentation and other nerve injuries, tendon transfers are a reliable option (9). A number of these transfers have been defined and are in practice, such as, Steindler flexoplasty, triceps to biceps transfer, uni/bipolar pectorlais major transfer and latissimus dorsi transfer. Schottstaedt et al. in 1955 described unipolar transfer of the latissimus dorsi for restoration of elbow flexion. Later Zancolli in 1973 and Stern in 1982 defined bipolar latissimus dorsi transfer for elbow flexion restoration (15, 20). Although unipolar latissimus dorsi is a useful & recommended option and a number of studies and case reports have been published (21, 22, 23, 24) it has certain drawbacks which limit its use, 1) indirect line of pull, 2) limited improvement in supination, 3) potentially difficult distal fixation, and 4) brachial plexus compression (24, 25, 26, 27). On the other hand bipolar latissimus dorsi transfer has several advantages over unipolar transfer, these include, 1) stabilization of shoulder joint, 2) straight line of pull, 3) better elbow flexion and 4) better range of motion (15, 17, 28, 29, ). Keeping in view the advantages and results from previous studies, we performed bipolar latissimus dorsi transfer in all our patients. Key points about the transfer include, 1) preoperative evaluation of the function of the muscle being transferred through clinical examination and electrophysiological studies, 2) a meticulous technique of harvest protecting the neurovascular bundle, 3) marking the resting length of the muscle for proper restoration of the muscle tension. All the patients in our study achieved excellent results. There was minor wound dehiscence in one patient and seroma at the donor site in 2 patients. Both complications were managed conservatively.
Conflict of Interest: We have no conflict of interest.
Disclosures: We have no disclosures to disclose.
References
1. Narakas AO. The treatment of brachial plexus injuries. Int Orthop. 1985;9:29-36.
2. Jain DK, Bhardwaj P, Venkataramani H, Sabapathy SR. An epidemiological study of traumatic brachial plexus injury patients treated ata an Indian centre. Indian J Plast Surg. 2012 sep;45(3):498-503. Doi: 10.4103/0970-0358. 105690
3. Solla, D. J. F., de Oliveira, A. J. M., Riechelmann, R. S., Martins, R. S., & Siqueira, M. G. (2020). Functional outcome predictors after spinal accessory nerve to suprascapular nerve transfer for restoration of shoulder abduction in traumatic brachial plexus injuries in adults: the effect of time from injury to surgery. European Journal of Trauma and Emergency Surgery, 1-7.
4. Segal, D., Cornwall, R., & Little, K. J. (2019). Outcomes of Spinal Accessory–to–Suprascapular Nerve Transfers for Brachial Plexus Birth Injury. The Journal of Hand Surgery, 44(7), 578-587.
5. Faglioni, W., Siqueira, M. G., Martins, R. S., Heise, C. O., & Foroni, L. (2014). The epidemiology of adult traumatic brachial plexus lesions in a large metropolis. Acta neurochirurgica, 156(5), 1025-1028
6. Martin, E., Senders, J. T., DiRisio, A. C., Smith, T. R., & Broekman, M. L. (2018). Timing of surgery in traumatic brachial plexus injury: a systematic review. Journal of neurosurgery, 130(4), 1333-1345.
7. Sakallariou VI, Badilas NK, Mazis GA, Stavropoulos NA, Kotoulas HK, Kyriakopoulos S, Tagkalegkas I, Sofianos IP. Brachial plexus injuries in adults: evaluation and diagnostic approach. ISRN Orthop. 2014 Feb 9;2014;726103. Doi: 10.1155/2014/726103.
8. Vekris MD, Beris AE, Lykissas MG, Korompilias AV, Vekris AD, Soucacos PN. Restoration of elbow function in severe brachial plexus paralysis via muscle transfers. Injury. 2008 Sep 1;39(3):15-22. 5.
9. de Moraes FB, Kwae MY, da Silva RP, Porto CC, de Paiva Magalhães D, Paulino MV. Evaluation of elbow flexion following free muscle transfer from the medial gastrocnemius or transfer from the latissimus dorsi, in cases of traumatic injury of the brachial plexus. Revista Brasileira de Ortopedia. 2015 Nov 1;50(6):660-5.
10. Rao PD, Rao RV, Srikanth R. Triceps to biceps transfer for restoration of elbow flexion following upper brachial plexus injury. Ind J Plastic Surg: Offici Pub Assoc Plastic Surg Ind. 2017 Jan;50(1):35.
11. Tsai TM, Kalisman M, Burns J, Kleinert HE. Restoration of elbow flexion by pectoralis major and pectoralis minor transfer. J Hand Surg. 1983 Mar 1;8(2):186-90.
12. Steindler A. Muscle and Tendon transplantation at the elbow. In: Arbor A, Edwards JW, eds. Instructional course lectures on reconstructive surgery. Ann Arbor: JW Edwards; 1944:276-283.
13. Monreal R. Steindler flexorplasty to restore elbow flexion in C5-C6-C7 brachial plexus palsy type. J Brach Plexus Peripheral Nerve Injur. 2007 Dec;2(1):15
14. Schottstaedt ER, Larsen LJ, Best FC. Com-plete muscle transposition. J Bone Joint Surg, 3lA. 1955;397.
15. Zancolli E, Mitre H. Latissimus dorsi transfer to restore elbow flexion: an appraisal of eight cases. JBJS. 1973 Sep 1;55(6):1265-75.
16. Chen WS. Restoration of elbow flexion by latissimus dorsi myocutaneous or muscle flap. Arch Orthop Trauma Surg 1990;109:117e20.
17. Kawamura K, Yajima H, Tomita Y, Kobata Y, Shigematsu K, Takakura Y. Restoration of elbow function with pedicled latissimus dorsi myocutaneous flap transfer. J Shoulder Elb Surg 2007;16(1):84e90.
18. Gutowski KA, Orenstein HH. Restoration of elbow flexion after brachial plexus injury: the role of nerve and muscle transfers. Plastic Reconst Surg. 2000 Nov 1;106(6):1348-58.
19. Bengtson KA, Spinner RJ, Bishop AT, Kaufman KR, Coleman-Wood K, Kircher MF, et al. Measuring outcomes in adult brachial plexus reconstruction. Hand Clin. 2008 Nov 1;24(4):401-15.
20. STERN, P. J., NEALE, H. W., GREGORY, R. 0. and KREILEIN, J. G. (1982). Latisshnus dorsl musculocutaneous flap for elbow flexion, The Journal of Hand Surgery, 7: 25-30
21. Agrawal NK, Choudhary AN, Agrawal P. Unipolar pedicled latissimus dorsi transfer for elbow reanimation in traumatic brachial plexus injuries. Int J Res Med Sci 2020;8:387-95.
22. Sadek AF, Ellabban MA. Unipolar Latissimus Dorsi Transfer for Restoration of Elbow Flexion in Residual Post-traumatic Brachial Plexus Palsy Associated with Distal Humeral Fractures. J Hand Microsurg. 2021 Dec 1;15(3):203-211. doi: 10.1055/s-0041-1739962. PMID: 37388566; PMCID: PMC10306985.
23. Monaisa B, Phiri S, Ndobe E (2020) Paediatric Elbow Flexion Reconstruction with the Latissimus Dorsi Muscle Flap, Case Report and Literature Review. J Med Res Surg. 1(4): pp. 1-3.
24. Bhatnagar A. Uni-polar Latissimus Dorsi Transfer for Restoration of Elbow Function in High Voltage Axillary Burn Leading to Brachial Plexus Injury. Journal of Peripheral Nerve Surgery (Volume 1, No. 1, July 2017).;57:59.
25. Brogan DM, Leversedge FJ. Surgical Technique and Anatomical Considerations for the Modified L'Episcopo Tendon Transfer. Hand (N Y). 2019 Jan;14(1):34-41. doi: 10.1177/1558944718803746. Epub 2018 Oct 7. PMID: 30295084; PMCID: PMC6346371.
26. Hsueh YH, Tu YK. Surgical reconstructions for adult brachial plexus injuries. Part I: Treatments for combined C5 and C6 injuries, with or without C7 injuries. Injury. 2020 Apr 1;51(4):787-803.
27. Mordick TG 2nd, Britton EN, Brantigan C. Pedicled latissimus dorsi transfer for immediate soft-tissue coverage and elbow flexion. Plast Reconstr Surg. 1997 May;99(6):1742-4. PMID: 9145150.
28. Stevanovic MV, Cuéllar VG, Ghiassi A, Sharpe F. Single-stage Reconstruction of Elbow Flexion Associated with Massive Soft-Tissue Defect Using the Latissimus Dorsi Muscle Bipolar Rotational Transfer. Plast Reconstr Surg Glob Open. 2016 Sep 28;4(9):e1066. doi: 10.1097/GOX.0000000000001066. PMID: 27757363; PMCID: PMC5055029.
29. Chaudhry S, Hopyan S. Bipolar latissimus transfer for restoration of elbow flexion. J Orthop. 2013 Jul 17;10(3):133-8. doi: 10.1016/j.jor.2013.06.004. PMID: 24396229; PMCID: PMC3861676.
30. Cambon-Binder A, Belkheyar Z, Durand S, Rantissi M, Oberlin C. Elbow flexion restoration using pedicled latissimus dorsi transfer in seven cases. Chirurgie de la Main. 2012 Dec 1;31(6):324-30..
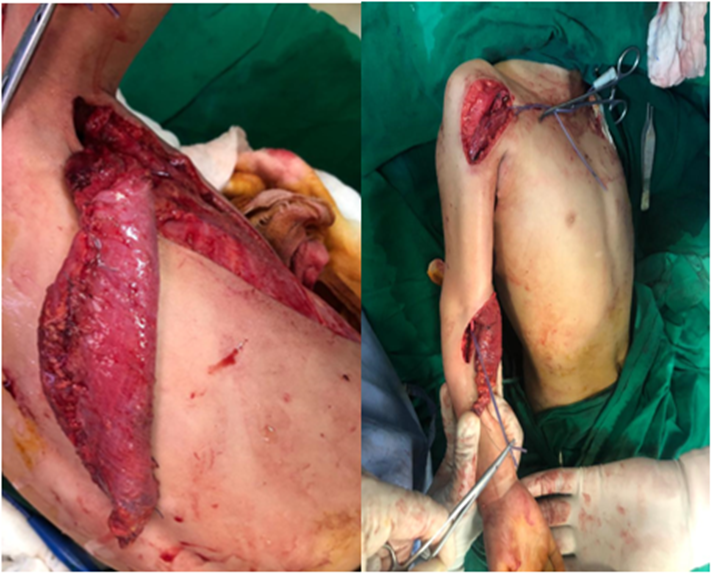
Figure 1

Figure 2