Atrial Fibrillation - Pharmacologic Cardioversion with Intravenous Calcium Gluconate
Atrial Fibrillation - Pharmacologic Cardioversion with Intravenous Calcium Gluconate
Ramachandran Muthiah*
*Correspondence to: Ramachandran Muthiah, Morning star hospital, Enayam Thoppu, Kanyakumari District, India.
Copyright.
© 2025 Ramachandran MuthiahThis is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 Aug 2025
Published: 01 Sep 2025
DOI: https://doi.org/10.5281/zenodo.17053196
Abstract:
A 66 year old known hypertensive and stroke patient presented with sudden onset of tachycardia and ECG revealed Paroxysmal Atrial Fibrillation (AF). Echocardiography revealed structurally normal heart with no intracardiac thrombi or spontaneous echo contrast. The arrhythmia was refractory to Diltiazem and amiodarone and it was reverted to sinus rhythm by intravenous calcium gluconate.
Atrial Fibrillation - Pharmacologic Cardioversion with Intravenous Calcium Gluconate
Introduction
Atrial fibrillation (AF) is the most common serious cardiac arrhythmia in the surgical setting and its incidence varies according to the type of surgery as 3% in adults aged ≥ 45 years undergoing non?cardiac surgery [1], but it is much higher (30%) in thoracic surgery [2]. Most patients developing AF after surgical intervention convert to sinus rhythm spontaneously [3] and this self?limited arrhythmia that usually does not always results hemodynamic compromise and death. However, evidence since the 1980s shows that POAF (postoperative AF) has a poor prognosis, with an increased risk of postoperative complications [4]. The rapid irregular ventricular rate can decrease coronary flow, leading to myocardial ischemia [5], decreased diastolic filling time and cardiac output, loss of atrial contraction [6] and all these effects on the cardiopulmonary hemodynamics can lead to hypotension. Long?term risk of complications such as stroke after non?cardiac surgery is 0.78% during the follow?up period of 2.1 years [7] and the cumulative risk of stroke at 1 year after discharge was 1.47% compared to 0.36% in those with no AF.
Case Report
The staff nurse in the postoperative surgical care unit noticed sudden onset of rapid irregular heart rate in the ECG monitor in a 66 year old male patient who underwent surgical resection for strangulated right sided inguinal hernia 6 hours before. He is an Asian black, 175 cm height, obese with BMI (body mass index 34 (weight 85 kg), blood pressure 130/80 mmHg with drugs, pulse rate 84 bpm and regular before surgery. He was a known hypertensive, not a smoker, alcoholic and diabetic. He had stroke one year back, but not taking any anticoagulants, antiplatelets and antiarrhythmic drugs before. He had repeated episodes of wheezing before surgery and is on amlodipine for hypertension which is under control. On examination, he was drowsy and not fully recovered from anaesthesia, afebrile, not anemic, not cyanosed, no clubbing and no pedal edema. Peripheral pulses were normally felt. Bruit over both carotids, Jugular venous pressure not elevated, No precordial bulge and apical impulse in the normal location. First heart sound varying in intensity. No murmurs or additional sounds, emphysematous chest with scattered rales and rhonchi in the lung fields and had right sided hemiparesis with aphasia. He suffered from right sided inguinal hernia for which he never underwent surgery before. He developed sudden onset of acute abdominal pain and referred to the surgical specialist.
Blood, liver and renal parameters were normal. Troponin T was < 0.01 ng/ml. X-ray chest showed emphysematous changes in the lung fields. Echocardiography revealed normal study. His ECG shown in Figure (1) before surgery seems to be normal. The ECG taken at the onset of rapid heart rate (180 bpm) was shown in Figure (2). He was treated with intravenous diltiazem 5 mg three bolus doses at 5 minutes interval. The ECG taken after intravenous diltiazem shown in Figure (3) revealed persistence of arrhythmia with a heart rate of 136 bpm. Then he was treated with intravenous amiodarone 150 mg bolus followed by 300 mg infusion. Following intravenous amiodarone, the patient developed hypotension with respiratory distress suddenly and the ECG taken was shown in Figure (4) revealed persistence of arrhythmia (nodal rhythm) with a heart rate of 115 bpm. The patient was supported with dopamine infusion and oxygen. Hypotension persisted and then he was supported with noradrenaline infusion. Hypotension still persisted with worsening of respiratory function and persistence of arrhythmia with the heart rate of 110 bpm. 10 ml of 10% solution of calcium gluconate (1 mL of 10% calcium gluconate contains 9.3 mg of elemental calcium) was given intravenously slowly on an emergency basis. Cardiopulmonary function was restored immediately with the reversion of arrhythmia to sinus rhythm as shown in Figure (5) and blood pressure was maintained at 120/70mm Hg. The heart rate was regular at a rate of 107 bpm.
Figure 1- 66 years old male with normal ECG before surgery.
Figure 2- 66 years old male with tachycardia after surgery
Figure 3- 66 years old male with tachycardia after IV diltiazem
Figure 4- 66 years old male with tachycardia after IV amiodarone
Figure 5- 66 years old male with normal sinus rhythm after IV calcium gluconate
Etiopathogenesis
Following non?cardiac surgery, AF usually occurs during the first 4 days and its pathophysiology is not well understood [8]. The possible mechanisms are shown in Table 1.
|
1. |
activation of the sympathetic nervous system due to the stress of surgery increases heart rate and catecholamines release |
|
2. |
clinical circumstances such as hypovolemia, intraoperative hypotension, anemia, trauma, and pain can also affect the sympathetic activity |
|
3. |
electrophysiological disturbances and metabolic imbalances (e.g., hypoglycemia or electrolytes disturbances). |
|
4. |
Hypoxia |
|
5. |
Hypervolemia |
Table 1. Mechanisms of postoperative atrial fibrillation in non cardiac surgery
Hypoxia leads to pulmonary vein vasoconstriction and increase right ventricular pressure and right atrial stretch. Also, hypoxia can cause ischemia of the myocardial atria cells and alters its conductivity. Hypervolemia increases the intravascular volume, which causes stretching of the right atrium. The independent predictors are increased age (55-74 , > 75 years), male gender, preoperative heart rate ≥ 72 beats/minute [9] and increased extent of operation [10]. Elevated preoperative B?type natriuretic peptide (BNP) measurements are independent predictor of POAF (postoperative atrial fibrillation) after thoracic surgery [11].
The prevalence of atrial fibrillation is much greater in aged population. Elderly patients > 40 years presenting with AF may have occult or masked hyperthyroidism (apathetic hyperthyroidism) in 10 to 30% of cases [12] Measurement of total T4 and T3 may be misleading since these concentrations are reduced in patients with heart disease or other serious illnesses. and a measurement of serum TSH provides a good evidence of Thyrotoxicosis [13],[14],[15].
Many elderly patients tolerate atrial fibrillation well without therapy because the ventricular rate is slow as a result of concomitant AV nodal disease [16]. The autonomic nervous system can trigger AF in susceptible patients through heightened vagal or adrenergic tone called as neurogenic AF. In adrenergic AF, the ventricular response is rapid and flutter does not occur. Beta-blockers are the first-line choice because of their beneficial effects in the hyper-adrenergic post-operative state [17] and patients usually are resistant to class Ia and Ic drugs. Intravenous diltiazem or metoprolol are commonly used for AF with a rapid ventricular response and Landiolol received FDA approval in November 2024, a beta adrenergic blocker indicated for short-term reduction of ventricular rate in adults with supraventricular tachycardia (including atrial fibrillation/atrial flutter) [18]. Sinus node dysfunction presents with a tachycardia, most commonly AF that terminate abruptly and is followed by a long offset pause before the resumption of sinus rhythm. For older patients with AF of unknown cause, the term "idiopathic AF" is often used. ‘Lone’ AF is the term which is often used to describe AF of unidentifiable cause in patients younger than 60 years [19] and it is distinguished from idiopathic AF [20], which implies uncertainty about its origin without reference to the age of the patient or associated cardiovascular pathology [21] and its prevalence varies from 1.6% to 31%. However, with modern diagnostic methodologies, many experts now feel that a cause for atrial fibrillation can be found in virtually all patients and the most recent major-organization guidelines state that the term “lone AF” should no longer been used [22]. Persistent AF is a prolonged episode of AF that typically lasts more than seven days and requires medical intervention to restore sinus rhythm [23]. AF burden varies considerably among individuals, moreover, even in patients with paroxysmal AF, AF patterns range from multiple short AF bursts (staccato rhythm) to a few long AF episodes (legato rhythm) [24],[25]. The age at the onset of vagal AF is 40 to 50 years and the ventricular response is relatively low (100 to 120 bpm). Digoxin and β blockers may aggravate the syndrome and class Ia agents may be particularly beneficial because of their vagolytic effects. The anticholinergic activity of long-acting disopyramide makes this a relatively attractive choice for patients with vagally induced AF and propafenone is not recommended because its (weak) intrinsic beta-blocking activity which may aggravate this type of paroxysmal AF. Familial AF with autosomal dominant mode of inheritance due to an abnormal genetic chromosomal loci was identified at chromosome 10q region [26] and in vagal fibrillation, the paroxysmal AF does not progress to chronic AF.
The proportion of stroke rising from 6.5% for ages 50 to 59 years to approximately 31% for ages 80 to 89 years and nonvalvular AF is the most powerful precursor of stroke in this population up to 15% [27]. Carotid artery disease is believed to be responsible for 10 to 20% [28] and most of them are related to embolism from a vulnerable plaque [29]. Thus patients with AF who experience symptoms of cerebral ischemia require careful evaluation of other causes, especially if they have been therapeutically anticoagulated.
Controlling risk factors is essential to prevent the onset of AF, and to try to maintain sinus rhythm over the long term [30]. In this patient systemic hypertension was well controlled with drugs and prophylactic anticoagulants and antiarrhythmic drugs were not prescribed to attribute AF as the etiology for the neurologic deficit. Carotid artery disease as evidenced by bruit over both carotids [31] is the clinically documented etiology for the neurological deficit happened before in this patient.
Discussion
Etiologically AV conduction system disease is unlikely since the heart rate was rapid. Elderly patients who are felt to have lone AF actually have a sick sinus syndrome [32] as the underlying cause. Sinus node dysfunction (SND) is most often related to age-dependent progressive fibrosis of the sinus nodal tissue and surrounding atrial myocardium [33]. Intravenous calcium gluconate may inhibit the sinus node and can cause cardiac arrest particularly in patients with sinus node dysfunction andso it is not the cause for AF in this case. Troponin T was normal and so coronary artery disease is not contributing. Thyroid function tests were normal and there was no left ventricular hypertrophy and diastolic dysfunction to attribute the etiology. Systemic hypertension was controlled with drugs. Triggering foci for paroxysmal AF from the pulmonary veins are more often in younger individuals. Increased vagal or sympathetic tone may cause AF in susceptible individuals. Vagal AF is characterized by slow ventricular response and sympathetic AF tends to disappear at rest. Severe infection is uncommon since the patient was afebrile with normal blood leukocyte count. The clinical and Echocardiographic features are not favourable for massive pulmonary embolism. X-ray chest revealed emphysematous changes in the lung fields attributing pulmonary pathology as the possible etiology of paroxysmal AF in this patient and surgery is the stress related precipitating factor.
Eventhough Ic agents (Flecainide) is the most appropriate drug for paroxysmal AF in structurally normal heart [34], it is not preferred since neurological dysfunction is the most frequent side effect of Flecainide. Diltiazem act as an arteriolar dilator by inhibiting calcium entry and a dose related fall in peripheral vascular resistance leading to drop in blood pressure. On intravenous amiodarone, patient developed hypotension refractory to vasopressors with respiratory distress suddenly and a marked reduction in heart rate as shown in Figure (4). Amiodarone has a significant negative dromotropic effect on AV conduction due to its intrinsic β blocking property and also has an appreciable calcium channel blocking effect. Pulmonary toxicity is the most serious adverse effect of amiodarone due to a hypersensitivity reaction [35]. The mechanism for the refractory hypotension may be due to the combined calcium channel blocking effects of both diltiazem and amiodarone. The respiratory distress is may be due to the hypersensitivity reaction of amiodarone in the lungs [36] which was aggravated by the preexisting lung disease.
10 ml of 10% solution of calcium gluconate was given intravenously on an emergency basis. Cardiopulmonary function was restored immediately with the reversion of arrhythmia to sinus rhythm as shown in Figure (5) and blood pressure was maintained at 120/70mm Hg. The heart rate was regular at a rate of 107 bpm. Calcium has a positive inotropic effect on the myocardium, increasing both the force of contraction and the maximum unloaded shortening velocity of cardiac muscle and rises the blood pressure and heart rate [37]. The rise in heart rate abolished the arrhythmia having the low heart rate and restore the sinus rhythm by overdrive suppression [38]. Calcium has a definite role in the stimulation of corticosteroid production [39],[40] and a significant increase in 11-hydroxy cortcosteroids can be demonstrated after intravenous calcium gluconate administration. These steroids may neutralize the hypersensitivity reaction occurred due to amiodarone therapy in the setting of preexisting lung disease manifested as increased respiratory distress. Thus the pulmonary function was restored at optimum with the normalization of blood pressure, rhythm and heart rate. Stunned atrium is defined as a state of temporary mechanic atrial dysfunction with preserved bioeletrical function. It may follow up to 38-80% successful cardioversions performed to convert atrial fibrillation to regular sinus rhythm. Lack of effective atrial contractility leads to hemodynamic changes, which may result in thrombus formation with subsequent thromboembolic events [41] and so the patient was advised warfarin for a minimum period of 4 weeks with maintaining the therapeutic INR of 2 to 3 to prevent thromboembolic episodes due to atrial stunning [42] following pharmacologic cardioversion with intravenous calcium gluconate.
Electrical cardioversion was not preferred since the patient is having chronic obstructive lung disease in the form of emphysematous changes. Emphysema can cause air trapping and reduced lung capacity, making it harder for the lungs to recover after the electrical shock [43]. In pulmonary disease, electrical cardioversion may not restore the sinus rhythm and may result in frequent recurrence of AF. Pharmacologic and electrical cardioversion may be ineffective in the management of atrial fibrillation in patients with COPD(chronic obstructive pulmonary disease) until respiratory decompensation has been corrected [44]. Calcium gluconate prevent the fall in blood pressure induced by calcium channel antagonists and restore the blood pressure to control values [45],[46].
Conclusion
Thus intravenous calcium gluconate play a role for Pharmacologic Cardioversion of Paroxysmal Atrial Fibrillation refractory to drugs having calcium channel blocking properties, resulting to hemodynamic compromise in pulmonary disease.
References
[1]. Bhave, P.,D., Goldman, L.,E., Vittinghoff, E., Maselli, J., Auerbach, A (2012) Incidence, predictors, and outcomes associated with postoperative atrial fibrillation after major noncardiac surgery, American Heart Journal, 164, 918-924.
[2] Maisel, W.,H., Rawn, J.,D., Stevenson, W.,.G (2001) Atrial fibrillation after cardiac surgery, Annals of Internal Medicine, 135, 1061-1073.
[3]Walsh, S.,R., Tang, T., Gaunt, M.,E., Schneider, H.,J (2006) New arrhythmias after non?cardiothoracic surgery, British Medical Journal, 333, 715
[4]Polanczyk, C.,A., Goldman, L., Marcantonio, E.,R., Orav, E.,J., Lee T.,H (1998) Supraventricular arrhythmia in patients having noncardiac surgery: clinical correlates and effect on length of stay, Annals of Internal Medicine, 129 , 279-285.
[5]Kochiadakis, G., E., Skalidis, E., I., Kalebubas, M.,D., Igoumenidis, N.,E., Chrysostomakis, S.,I., Kanoupakis, E., M., Simantirakis, E., N., Vardas, P.,E (2002) Effect of acute atrial fibrillation on phasic coronary blood flow pattern and flow reserve in humans, European Heart Journal, 23, 734-741.
[6]Heintz, K., M., Hollenberg, S., M (2005) Perioperative cardiac issues: postoperative arrhythmias, Surgical Clinics of North America, 85, 1103-1114.
[7]Gialdini, G., Nearing, K., Bhave, P.,D., Bonuccelli, U., Iadecola, C., Healey, J.,S., Kamel, H (2014) Perioperative atrial fibrillation and the long?term risk of ischemic stroke, Journal of American Medical Association (JAMA), 312, 616- 622.
[8]Danelich, I.,M., Lose, J.,M., Wright, S.,S., Asirvatham, S.,J., Ballinger, B.,A., Larson, D.,W., Lovely, J., K (2014) Practical management of postoperative atrial fibrillation after noncardiac surgery, Journal of American College of Surgery, 219, 831-841.
[9]Passman, R.,S., Gingold, D.,S., Amar, D., Lloyd?Jones, D., Bennett, C.,L., Zhang, H., Rusch, V.,W (2005) Prediction rule for atrial fibrillation after major noncardiac thoracic surgery, Annals of Thoracic Surgery, 79, 1698-1703
[10]Onaitis, M., D'Amico, T., Zhao, Y., O'Brien, S., Harpole, D (2010) Risk factors for atrial fibrillation after lung cancer surgery: analysis of the Society of Thoracic Surgeons General Thoracic Surgery Database, Annals of Thoracic Surgery, 90, 368-374.
[11] Simmers, D., Potgieter, D., Ryan, L., Fahrner, R., Rodseth, R., N (2015) The use of preoperative B?type natriuretic peptide as a predictor of atrial fibrillation after thoracic surgery: systematic review and meta?analysis, Journal of Cardiothoracic and Vascular Anesthesia, 29, 389-395.
[12] Forfar, J.,C., Toft, A (1982) Thyrotoxic AF- an underdiagnosed condition, British Medical Journal, 285, 909—910.
[13]Sawin, C.,T., Geller, A., Wolf, P.,A., et al (1994) Low serum thyrotropin concentration as a risk factor for AF in older persons, New England Journal of Medicine, 331, 1249.
[14]Woeber, K.,A (1992) Current concepts-Thyrotoxicosis and Heart, New England of Medicine, 327,94.
[15] Moran,C., Schoenmakers,N., Halsall, D., Oddy, S., Lyons,G., Berg, S.,V.,D., Gurnell, M., Chatterjee,K (2024) Approach to the Patient With Raised Thyroid Hormones and Nonsuppressed TSH, The Journal of Clinical Endocrinology & Metabolism, 109, 4, 1094–1108.
[16] Aronow, W.,S., Banach, M (2009) Atrial Fibrillation: The New Epidemic of the Ageing World, Journal of Atrial Fibrillation, 1, 1, 6, 154.
[17]Dan,G.,A., Rubio,A.,M., Agewall, S., Boriani, G., Borggrefe, M., Gaita, F., Gelder, I.,V., et al (2018) ESC Scientific Document Group, Antiarrhythmic drugs–clinical use and clinical decision making, Asia-Pacific Heart Rhythm Society (APHRS) and International Society of Cardiovascular Pharmacotherapy (ISCP), EP Europace, 20, 5, 731–732.
[18]Lawrence Rosenthal, Rottman, J.,N (2025) Atrial Fibrillation Treatment & Management, Medscape, Updated: Jan 22.
[19]Potpara, T.,S.,Lip, G.Y.H. (2014) Lone atrial fibrillation – an overview, International Journal of Clinical Practice, 68, 418-433.
[20]Fuster, V., Ryde´n, L.,E., et al (2001) ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: executive summary, Circulation, 104, 2118–2150.
[21]Bockus,L., Kassar,A., Chahine, Y., Chamoun, N., Haykal, R., Li,J., Wang,D.,Brien, K.,O., Tian, R., Sotoodehnia, N., Ordovas, K., Akoum, N (2025) Atrial fibrillation is associated with higher oxygen extraction in the human heart, American Heart Journal, 287, 130-137.
[22] Reiffel, J.,A (2025) 'Lone' Atrial Fibrillation is a Four Letter Word, The American Journal of Medicine, ISSN 0002-9343.
[23] Heart Rhythm 2025 Features Advances in AI that Enhance Safety of Atrial Fibrillation Treatment, April 24.
[24] Wineinger, N.,E., Barrett, P.,M., Zhang, Y., et al (2019) Identification of paroxysmal atrial fibrillation subtypes in over 13,000 individuals, Heart Rhythm, 16,1, 26–30.
[25]Cai, Minsi, Heijman, Jordi (2025) Challenges and Opportunities for Atrial Fibrillation Management, Cardiology Discovery, 5,2, 149-161.
[26]Campuzano, O., Serra, A.,P., Iglesias, A., Brugada, R (2016) Genetic basis of atrial fibrillation, Genes & Diseases, 24, 3, 4, 257-262.
[27] Ullah, Mohammad. (2008) Prevention of Stroke in Nonvalvular Atrial Fibrillation, Cardiovascular Journal, 1, 64-71.
[28] Barrett, K.,M., Brott, T.,G (2017) Stroke Caused by Extracranial Disease, Circulation Research, 120, 496-501.
[29] Mechtouff, L., Rascle, L., Crespy, V., Canet-Soulas, E., Nighoghossian, N., Millon, A (2021) A narrative review of the pathophysiology of ischemic stroke in carotid plaques: a distinction versus a compromise between hemodynamic and embolic mechanism, Annals of Translational Medicine, 9,14, 1208.
[30] Sellal, J.,M., Hammache, N., Echivard, M (2025) La fibrillation atriale en: diagnostic et prise en charge [Atrial fibrillation in 2025: Diagnosis and treatment]. Rev Med Interne (French medical journal), 12, S0248-8663.
[31] Lucerna, A., Espinosa, J (2025) Carotid Bruit. [Updated 2023 Feb 13]. In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, January.
[32]Aminah Wali (2025) Arrhythmia, Sick Sinus Syndrome, Cardiology Advisor, July 18.
[33] Kantharia, B.,K., El-Chami, M.,F (2025) Sinus Node Dysfunction, Medscape,
Updated: July 08.
[34] Olshansky, B., Mina, K., Chung, Steven, M., Pogwizd, Nora Goldschlager (2017) Treatment of Arrhythmias, Arrhythmia Essentials, 357-396,
[35] Martin, W.J. et al. (1988) Amiodarone Pulmonary Toxicity, CHEST, 93, 5, 1067 – 1075.
[36] Meter, M., Prusac, I.,K., Glavaš, D., Meter, D (2021) Acute respiratory failure on a low dose of amiodarone - is it an underdiagnosed and undertreated condition? Respiratory Medicine Case Reports, 5, 34, 101500.
[37] Eisner, D.,A., Caldwell, J.,L., Kistamás, K., Trafford, A.,W (2017) Calcium and Excitation-Contraction Coupling in the Heart, Circulation Research, July 7, 121,2, 181-195.
[38] Cabo, C., Wit, A.,L (1997) Cellular Electrophysiologic Mechanisms of Cardiac Arrhythmias, Cardiology Clinics, 15, 4, 517-538.
[39]Gilbon, Y (1970)Influence of intravenous administration of calcium gluconate on 11-hydroxycorticosteroid secretion by the adrenal cortex, Journal of Clinical Endocrinology, 31,336-338.
[40] Davies, E., Kenyon, C.,J., Fraser, R (1985) The role of calcium ions in the mechanism of ACTH stimulation of cortisol synthesis, Steroids, 45, 6, 551-560.
[41]Dabek, J., Gasior, Z., Monastyrska-Cup, B., Jakubowski, D (2007) Kardiowersja a og?uszenie przedsionków [Cardioversion and atrial stunning], Pol Merkur Lekarski (Polish medical journal, Poland), 22, 129, 224-228.
[42] Lucà, F., Giubilato, S., Di Fusco, S.,A., Piccioni, L., Rao, C.,M., Iorio, A., Cipolletta, L., D'Elia, E., Gelsomino, S., Rossini, R., Colivicchi, F., Gulizia, M.,M (2021) Anticoagulation in Atrial Fibrillation Cardioversion: What Is Crucial to Take into Account, Journal of Clinical Medicine, 21, 10, 15, 3212.
[43]Pahal, P., Avula, A., Afzal, M (2025) Emphysema [Updated Mar 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
[44] Lopez, C.,M., House-Fancher, M.,A (2005) Management of atrial fibrillation in patients with chronic obstructive pulmonary disease, Journal of Cardiovascular Nursing. 20, 2, 133-140.
[45] Weiss, A.,T., Lewis, B.,S., Halon, D.,A., Hasin, Y., Gotsman, M.,S (1983) The use of calcium with verapamil in the management of supraventricular tachyarrhythmias, International Journal of Cardiology, 4, 3, 275-284.
[46]Roguin, N., Shapir, Y., Blazer, S., Zeltzer, M., Berant, M (1984) The use of calcium gluconate prior to verapamil in infants with paroxysmal supraventricular tachycardia, Clinical Cardiology, 7, 613.
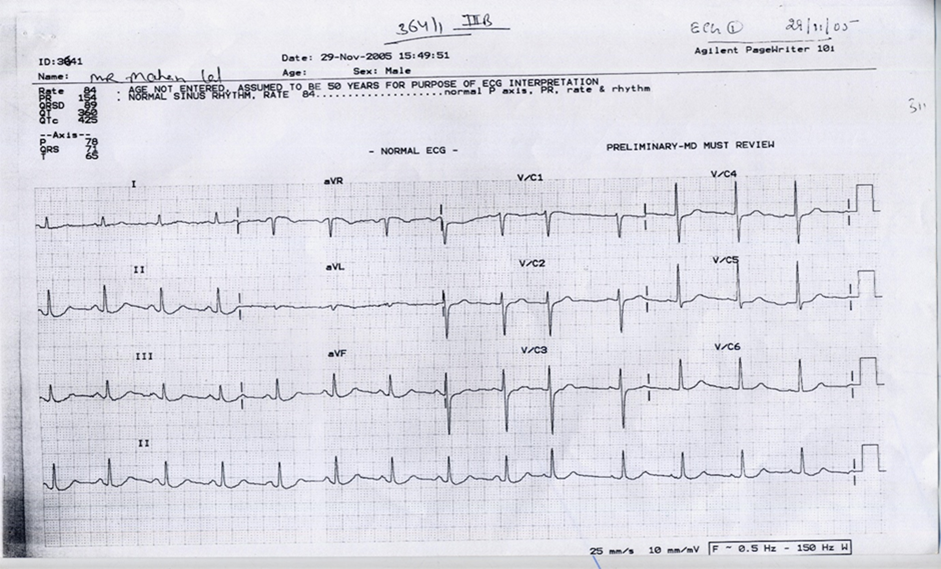
Figure 1
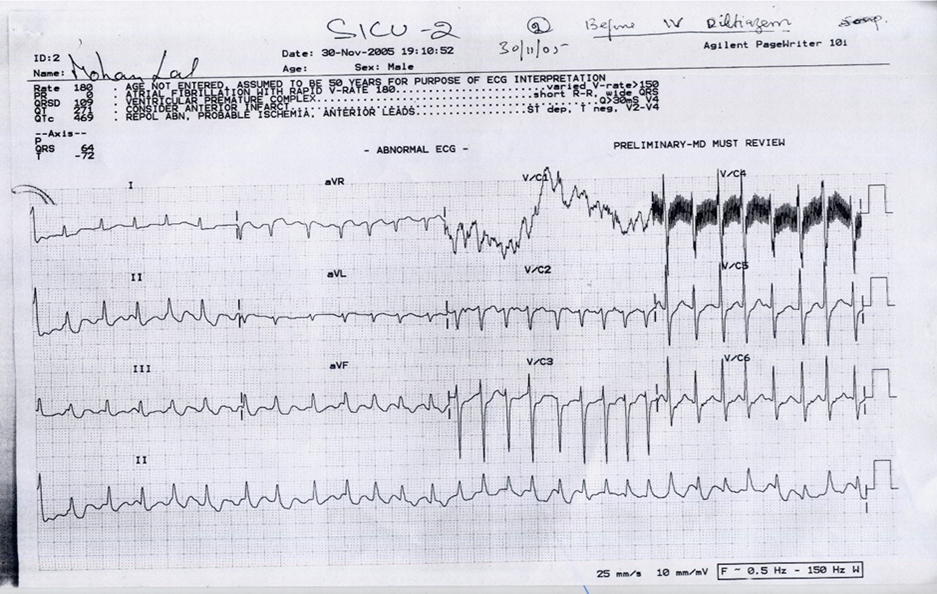
Figure 2
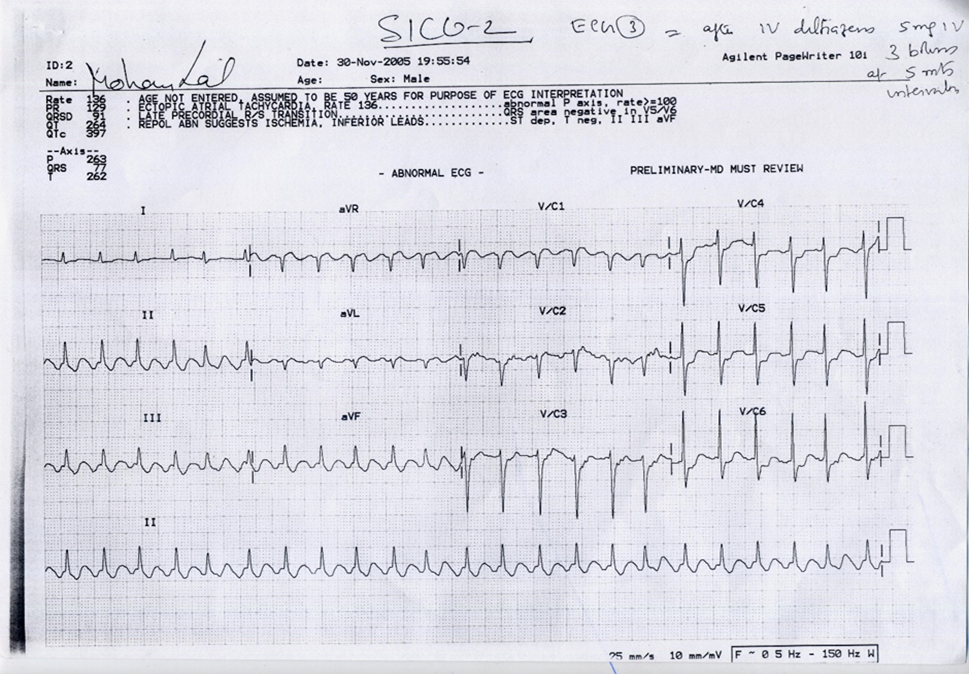
Figure 3
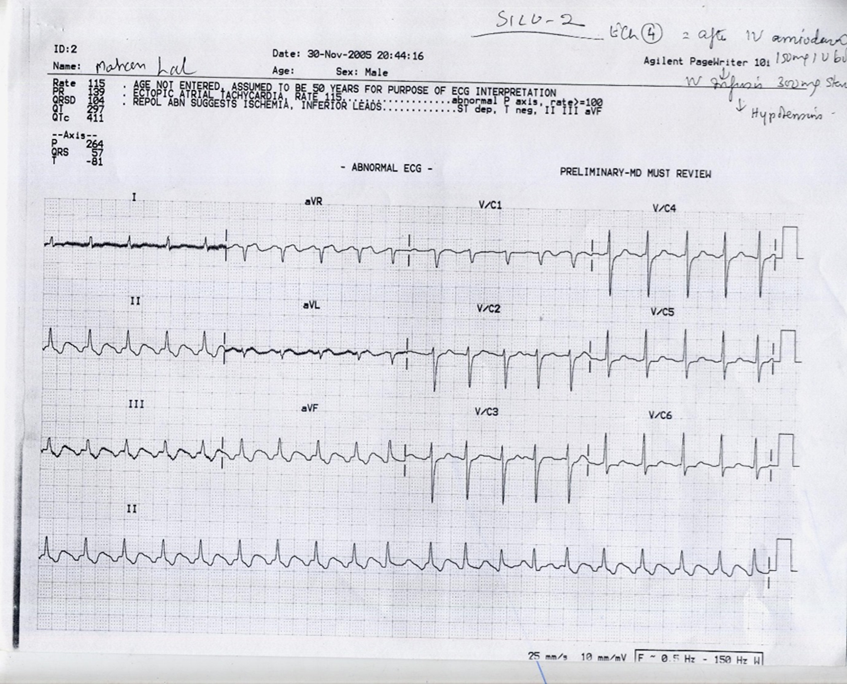
Figure 4
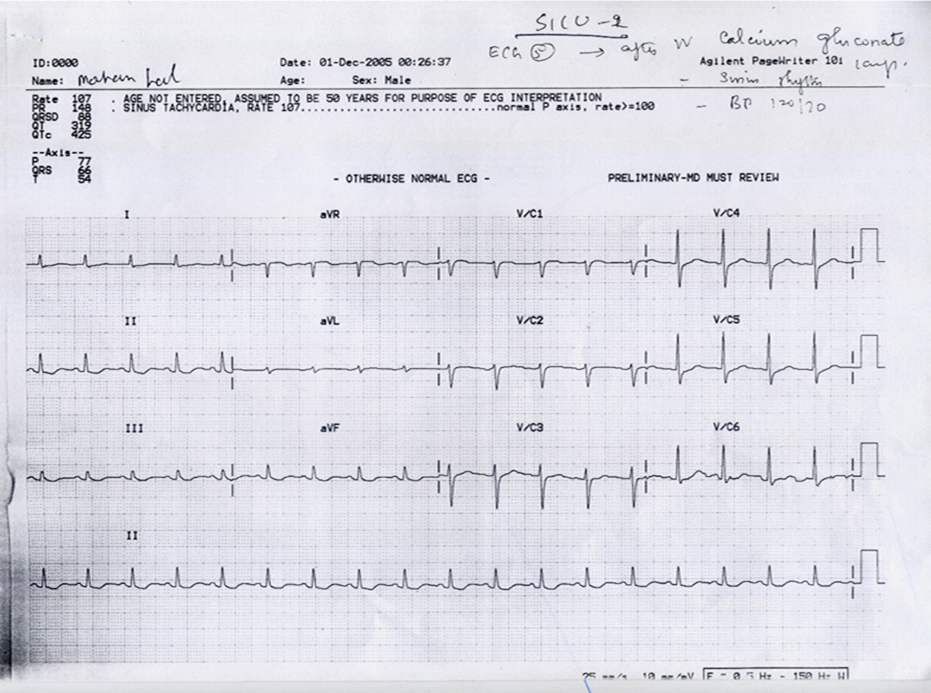
Figure 5