Rabies Masquerading as Guillain–Barré Syndrome in an Endemic Region: A Diagnostic Dilemma in the Absence of Exposure History
Rabies Masquerading as Guillain–Barré Syndrome in an Endemic Region: A Diagnostic Dilemma in the Absence of Exposure History
Dr Abhisek Guin MD1*, Dr Niket Yende MD2, Dr Anu Singh MD3
*Correspondence to: Dr. Abhisek Guin, Senior Resident (SR) in the Department of Neurology , AIIMS Rishikesh, India.
Copyright
© 2025 Dr. Abhisek Guin, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 Aug 2025
Published: 01 Sep 2025
DOI: https://doi.org/10.5281/zenodo.17043296
Abstract
Rabies, a fatal viral encephalitis caused by Rabies lyssavirus, typically presents in encephalitic or paralytic forms. We report a 22-year-old male from a rabies-endemic region who presented with symmetrical ascending flaccid quadriparesis and sensory disturbances, initially misdiagnosed as Guillain–Barré syndrome (GBS). Lack of a definitive bite history and initial absence of encephalitic signs delayed diagnosis. Progressive cranial neuropathies, behavioral changes, and classical phobic spasms—hydrophobia and aerophobia—emerged later, raising suspicion of rabies. Confirmatory tests, including RT-PCR of saliva and nuchal skin biopsy immunofluorescence, detected rabies viral RNA and antigen. Despite supportive care, the patient succumbed to dysautonomia-induced cardiac arrest. Post-mortem findings confirmed Negri bodies. This case highlights the diagnostic challenges of paralytic rabies, especially in the absence of exposure history, and underscores the importance of maintaining high clinical suspicion in endemic settings.
Rabies Masquerading as Guillain–Barré Syndrome in an Endemic Region: A Diagnostic Dilemma in the Absence of Exposure History
1. Introduction
Rabies is invariably a fatal zoonotic viral encephalitis caused by Rabies lyssavirus, a neurotropic virus of the Rhabdoviridae family [1]. The virus is typically transmitted through the saliva of infected animals, most commonly dogs, via bites or scratches. Clinically, rabies presents in two major forms: the furious (encephalitic) variant, characterized by hydrophobia, aerophobia, and agitation; and the paralytic (dumb) variant, which accounts for approximately 20–30% of human cases [1,3]. The paralytic form may resemble Guillain–Barré syndrome (GBS) because of its presentation with ascending symmetrical flaccid paralysis [4]. The absence of classical encephalitic signs in the early stages contributes to diagnostic delays [3,5]. Here, we report a case of paralytic variant of rabies presenting as symmetrical ascending flaccid quadriparesis.
Figure 1. (a) T2-weighted MRI of the brain at basal ganglia level showing no abnormal signal intensity. (b) T2-weighted MRI at midbrain level also appears normal.
Case Report
A 22-year-old previously healthy male presented with a five-day history of symmetrical weakness, beginning in the lower limbs and progressing to involve the trunk and upper limbs. This was accompanied by a tingling sensation in both lower limbs, circumferentially distributed up to the knees. Neurological examination revealed generalized areflexia, with muscle strength graded 1/5 in the lower limbs and 3/5 in the upper limbs. There was loss of fine touch and pain sensation below the knees. Bowel and bladder functions were preserved, and no cranial nerve involvement were noted initially.
He reported an antecedent diarrheal illness two days prior to the onset of neurological symptoms. There was no history of dog bite, or recent vaccination. Nerve conduction studies showed sensory-motor axonal neuropathy in the lower limbs, while upper limb conduction were within normal limits. Cerebrospinal fluid (CSF) analysis did not reveal albuminocytological dissociation. Given the clinical picture of acute flaccid paralysis with sensory involvement and recent gastrointestinal illness, a provisional diagnosis of Guillain–Barré syndrome was made, and intravenous immunoglobulin (IVIG) therapy was initiated.
From the sixth day of illness, he developed progressive bulbar and bilateral facial weakness, along with features of dysautonomia. The patient also complained of diplopia. Examination revealed a left lateral rectus palsy. From the eighth day onward, behavioral disturbances including irritability and irrelevant speech emerged. Over 2–3 days, his condition worsened; he developed visual hallucinations, episodes of aggression, and loss of orientation.
In light of the new cranial nerve findings and emerging behavioral symptoms, the possibility of Bickerstaff brainstem encephalitis (BBE) or Bickerstaff–GBS overlap was considered. Anti-GQ1b IgG antibody testing was planned. His electrolytes and metabolic parameters were within normal limits. EEG and MRI brain did not reveal any abnormality.
On day 10, the clinical course deviated unexpectedly. During feeding via Ryle’s tube, he exhibited marked fear responses, suggestive of hydrophobia. He developed sudden fearful reactions and pharyngeal spasms when exposed to minimal stimuli such as a fan or a breeze across the face—findings consistent with aerophobia. These symptoms prompted reconsideration of the diagnosis with strong suspicion of paralytic rabies.
RT-PCR testing of saliva and immunofluorescence staining of a nuchal skin biopsy were performed, confirming the diagnosis by detecting rabies viral RNA and nucleoprotein antigen, respectively.
The patient’s condition deteriorated rapidly. His sensorium worsened, and he became unresponsive to commands. He developed severe autonomic instability, culminating in sudden cardiac arrest and death approximately two weeks after symptom onset. Post-mortem brain biopsy revealed widespread deposition of rabies viral antigens and classical Negri bodies.
Discussion
This case aligns predominantly with the paralytic form of rabies, supported by the initial clinical features of symmetrical flaccid paralysis, areflexia, and sensory disturbances followed by cranial nerve palsies, hallucinations, and classical phobic spasms—hydrophobia and aerophobia. Paralytic rabies is probably underdiagnosed because it mimics Guillain–Barré syndrome (GBS) and lacks typical encephalitic symptoms in the initial stages. [7]. The diagnosis is further delayed due to numerous instances arising from small or unobserved exposures, such as scratches or saliva contacting wounds or mucosa, without a definitive bite history [2,5]. In many instances, identifiable exposure may be absent or even forgotten due to a prolonged incubation period, typically ranging from 1 to 3 months, though it might extend to several years [12,7].
After inoculation, rabies virus entry is genotype-dependent. Canine rabies virus binds to nicotinic acetylcholine receptors at the neuromuscular junction, aided by neural cell adhesion molecules (NCAM/CD56), whereas bat lyssaviruses may infect via unidentified skin receptors. The virus spreads centripetally via retrograde transport along motor neurons, progressing trans-synaptically every 12 hours. Infection involves spinal motor neurons, interneurons, and dorsal root ganglia (DRG), especially large proprioceptive afferents. This explains sensory deficits such as bilateral leg paresthesia seen in our case. Love et al. described sensory abnormalities—including hyperesthesia, segmental anesthesia, proprioceptive loss, and abdominal pain—in atypical rabies cases [12]. Sheikh et al. confirmed DRG pathology with serial nerve conduction studies revealing absent or declining SNAPs. Viral spread continues to contralateral and lower spinal segments and ascends through brainstem and corticospinal pathways. Once in the CNS, rapid viral amplification occurs in the spinal cord, brainstem, thalamus, basal ganglia, and hippocampus regardless of clinical subtype. Weakness may result from immune-mediated injury to anterior horn cells, axonal degeneration, direct immune attack on axons, or autoimmune peripheral nerve involvement [8]. Serial nerve conduction studies may show progressive CMAP reduction [9]. As infection advances, manifestations include progressive limb weakness, bulbar involvement, facial diplegia, oculomotor palsy, behavioral abnormalities, psychosis, altered sensorium, and phobic spasms. Dysfunction of sensory nerves in the heart and autonomic plexuses, or involvement via intraspinal propagation, contributes to dysautonomia in later stages.[1] Our patient died of cardiac arrest due to dysautonomia approximately two weeks after illness onset, which aligns with the average survival time reported in paralytic rabies cases [13]
CSF analysis may reveal mild pleocytosis with normal protein levels. EEG and MRI are often normal and nondiagnostic, especially in paralytic forms as seen in our case [3,16,17]. RT-PCR of saliva and immunofluorescence staining of nuchal skin biopsies detect viral RNA and nucleoprotein antigen with sensitivities ranging from 50% to 100%, highest when serial samples are tested [5,19]. Postmortem detection of Negri bodies—eosinophilic cytoplasmic inclusions in infected neurons—remains a classic hallmark but may be absent early [4].
Paralytic rabies may initially mimic GBS, with fever, gastrointestinal symptoms, and symmetrical ascending paralysis with sensory loss—especially without clear exposure history. The emergence of neuropsychiatric symptoms and classical phobic spasms should prompt suspicion of rabies. This highlights the critical need for high clinical suspicion and early molecular diagnostics in endemic areas for timely management and public health action.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given consent for their clinical information to be reported in the journal. The patient understands that their name and initials will not be published, and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflicts of interest
None declared.
Financial support and sponsorship
Nil.
References
1. Hemachudha T, Ugolini G, Wacharapluesadee S, et al. Human rabies: neuropathogenesis, diagnosis, and management. Lancet Neurol. 2013 May;12(5):498–513. doi:10.1016/S1474-4422(13)70038-3.
2. Fooks AR, Banyard AC, Horton DL, et al. Current status of rabies and prospects for elimination. Lancet. 2014 Sep 27;384(9951):1389–99. doi:10.1016/S0140-6736(13)62707-5.
3. Warrell MJ, Warrell DA, Mahalingam R. Rabies encephalitis. Lancet. 2004 Mar 20;363(9413):849–58. doi:10.1016/S0140-6736(04)15641-9.
4. Jackson AC, Wunner WH. Rabies: scientific basis of the disease and its management. 3rd ed. Oxford: Academic Press; 2013.
5. Dacheux L, Larrous F, Mailles A, et al. A reliable diagnosis of human rabies based on analysis of skin biopsy specimens. Clin Infect Dis. 2008 Nov 1;47(9):1410–7. doi:10.1086/592566.
6. Sudarshan MK, Madhusudana SN, Mahendra BJ, et al. Assessing the burden of human rabies in India: results of a national multi-center epidemiological survey. Int J Infect Dis. 2007 Jan;11(1):29–35. doi:10.1016/j.ijid.2006.05.011.
7. Hemachudha T, Wacharapluesadee S, Wilde H, et al. Challenges in the diagnosis and management of human rabies: a case report and review of the literature. Ann Neurol. 2005 Sep;58(3):394–400. doi:10.1002/ana.20554.
8. Sheikh KA, Jackson AC, Ramos-Alvarez M, et al. Paralytic rabies: immune attack on nerve fibers containing axonally transported viral proteins. Neurology. 1998 Apr;50 Suppl 4:S183–4.
9. Sheikh KA, Yun J, Boulis NM, et al. Peripheral nerve and spinal cord pathology in paralytic rabies. Ann Neurol. 2005 Sep;58(3):389–93. doi:10.1002/ana.20553.
10. Chopra JS, Malik S, Koul RL. Guillain-Barré syndrome—clinical profile in 32 cases. Neurol India. 1980 Sep;28(3):204–10.
11. Fooks AR, Johnson N, Freuling CM, et al. Rabies. Nat Rev Dis Primers. 2017 Sep 21;3:17091. doi:10.1038/nrdp.2017.91.
12. Love S. Unusual forms of rabies: a clinical and pathological study. Lancet. 1944 May 27;243(6297):1015–22.
13. Hemachudha T, Phanuphak P, Wilde H, et al. Rabies and other lyssavirus diseases. Lancet. 2002 Aug 24;360(9341):509–19. doi:10.1016/S0140-6736(02)09844-9.
14. Israsena N, Mahavihakanont A, Hemachudha T, Wacharapluesadee S, Mitrpant C. Rabies virus infection and microRNAs. Adv Virus Res. 2011;79:329–44. doi:10.1016/B978-0-12-387040-7.00015-9.
15. Jackson AC. Pathogenesis. In: Jackson AC, editor. Rabies: scientific basis of the disease and its management. 3rd ed. Oxford: Academic Press; 2013. p. 299–349.
16. Kumar A, Prakash S, Pandey S, et al. MRI features in human rabies encephalitis. Neurol India. 2012 Nov-Dec;60(6):626–8. doi:10.4103/0028-3886.104060.
17. Lopez-Barreiro A, Bataller L, Artigas C, et al. MR imaging findings in human rabies encephalitis. AJNR Am J Neuroradiol. 1995 Sep;16(8):1703–7.
18. Banyard AC, Fooks AR, Horton DL, et al. Laboratory diagnosis of rabies. Virus Res. 2014 Sep;197:150–63. doi:10.1016/j.virusres.2014.06.014.
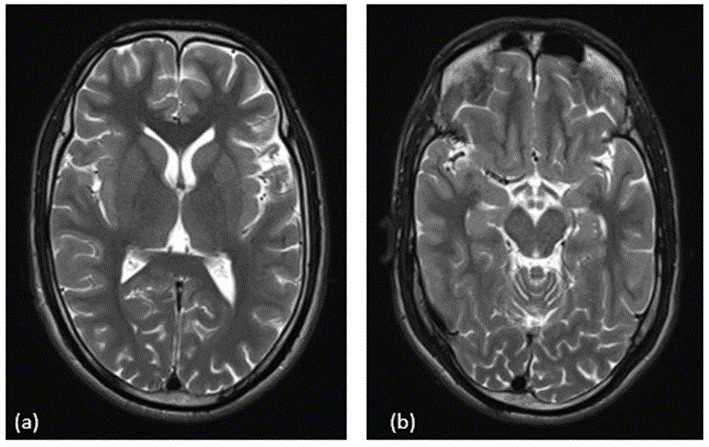
Figure 1