Tracheal Resection and Anastomosis for Malignant Tumours: A Tertiary Centre Experience
Tracheal Resection and Anastomosis for Malignant Tumours: A Tertiary Centre Experience
Deepa Swaminathan 1*, S Bhargavi 2, K Karthikesh 3
1. Head and Neck Surgical Oncologist, KG Hospital, Coimbatore, Tamil Nadu, India.
2 Surgical Oncologist, Sri Ramakrishna Hospital, Coimbatore, Tamil Nadu, India
*Correspondence to: Deepa Swaminathan, Head and Neck Surgical Oncologist, KG Hospital, Coimbatore, Tamil Nadu, India.
Copyright.
© 2025 Dr Deepa Swaminathan This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 Sep 2025
Published: 11 Sep 2025
DOI: https://doi.org/10.5281/zenodo.17284957
Abstract
Primary neoplasms of trachea are rare and uncommon malignancies that account for about 0.2% of respiratory malignant lesions, representing a low rate of all airway neoplasm deaths. In the early stages of the disease, symptoms often lack specificity often leading to misdiagnosis as other respiratory conditions. In most cases, wherever resectable, surgical resection is the treatment of choice. Radiotherapy (RT) is reserved for adjuvant settings or in cases with extensive disease or those who are medically unfit for surgery. Here we report three cases of malignant tracheal tumors with description of the surgical techniques employed along with a review of literature on this condition. This article underscores the importance of clinical suspicion, endoscopic and CT evaluation in timely diagnosis. Appropriate surgical resection and reconstruction is still the best modality to achieve long term survival with a decent quality of life.
Key Words- tracheal tumours, tracheal resection, adenoid cystic carcinoma, papillary carcinoma thyroid.
Tracheal Resection and Anastomosis for Malignant Tumours: A Tertiary Centre Experience
Introduction
Primary neoplasms of trachea are rare and uncommon malignancies that account for less than 0.01% of all tumours and about 0.2% of respiratory malignant lesions, representing a low rate of all airway neoplasm deaths [1-3]. The most common histologic types are squamous cell carcinoma (SCC), representing about 50–66%, and adenoid cystic carcinoma (ACC), accounting for 10–15% of them [4]. Several malignant histologies, of different grade, have also been described, as mucoepidermoid carcinoma, non-squamous bronchogenic carcinoma, sarcoma, carcinoid tumours, melanomas [5,6]. Another possibility, though less frequent, is tracheal involvement by well differentiated thyroid carcinoma (WDTC). This scenario is exemplified by a rate of 3.4–13% [7].
In the early stages of the disease, symptoms often lack specificity, and some individuals may exhibit manifestations like cough, sputum production, chest tightness, and shortness of breath, often leading to misdiagnosis as other respiratory conditions. Definitive diagnosis is established through imaging and histological examinations [8].
In most cases, wherever resectable, surgical resection is the treatment of choice. Radiotherapy (RT) is reserved for adjuvant settings or in cases with extensive disease or those who are medically unfit for surgery. The basic challenges in surgical resection of tracheal tumors are the following: type and access for anesthesia, dissection around the trachea, type of tracheal resection, and restoration of continuity of the trachea [9].
Here we report three cases of malignant tracheal tumors with description of the surgical techniques employed along with a review of literature on this condition.
Case Presentation
Patient 1
A 46 year old female presented with complaints of breathing difficulty for the past five months. She had consulted a pulmonologist for the above symptoms and was started on medical management. As there was no relief in her symptoms, she was then evaluated with CT scan of neck and thorax which revealed a suspicious subglottic growth. No obvious neck or mediastinal nodes were noted. Flexible bronchoscopy revealed a polypoidal lesion arising from the right lateral wall with significant lumen narrowing extending from the second tracheal ring till about three centimeters distally. Rest of her clinical and laboratory examinations were normal. To relieve her of her breathing difficulty and to obtain a diagnosis, she was taken up for laser debulking of the said lesion under general anaesthesia. Histopathologic examination showed features of adenoid cystic carcinoma. She was then referred to our centre. Here further evaluation and a multimodality tumour board meeting was conducted and it was decided to proceed with primary surgery followed by adjuvant RT. Anterior cervical approach was used with a low collar incision. Resection was performed from the first tracheal ring till the fifth ring. Adequate gross margins were confirmed. The larynx and the lower stump of the trachea were then mobilised digitally and anastomosis done in end to end fashion. A tracheostomy was done two rings distal to the anastomosis. The suture site was further buttressed with the strap muscles and the wound was closed. Stay sutures were placed from skin over the lower jaw to the clavicle (Guardian sutures) to maintain neck flexion and the same was retained for a period of two weeks after which she was discharged.
Post operative histopathology report showed adenoid cystic carcinoma with a close inferior margin (<5 mm). She received adjuvant RT (60 Gy) and was decannulated after completion of the same. She was then regularly followed up and has been disease free for two years.
Fig 1: Trans cervical view of the trachea post resection
Fig 2: Neck flexed in postoperative period with Guardian suture
Patient 2
A 51 year old female patient presented with a history of neck swelling that had been gradually increasing in size over the past six months and breathing difficulty for the last two months. A CT of the neck showed a mass lesion in the right lobe of thyroid infiltrating the right lateral wall of trachea with significant right level III lymph node. FNAC of the thyroid swelling showed evidence of papillary carcinoma of thyroid. Flexible bronchoscopy revealed growth in the right wall of trachea around 1 cm below the subglottis.
Fig 3: Contrast enhanced CT (axial view) image showing tumour involving the right lobe of thyroid with extrathyroidal extension in to trachea right lateral wall
Fig 4: Bronchoscopic image of tracheal infiltration
She underwent total thyroidectomy with en bloc resection of the anterior wall and part of the right posterior wall of trachea extending from the first to fifth rings. Additionally, right comprehensive neck dissection was done. To ensure that the closure does not significantly compromise the tracheal lumen, the posterior wall was divided in a diagonal fashion and the proximal and distal stumps were rotated and anastomosis was done in a skewed manner. The anastomosis was buttressed with the strap muscles, tracheostomy was performed and guardian sutures were placed. Guardian sutures and tracheostomy tube were removed in the second post operative week. Her histopathology revealed a conventional type of papillary carcinoma with invasion of trachea. Margins of resection were free. She also had regional metastasis to the right middle jugular group of nodes. She received adjuvant high dose radio Iodine ablation and then was started on a suppressive dose of thyroxine.
Patient 3
A 64 year old female patient had a history of right sided neck swelling for two years. She was evaluated at an outside centre and was found to have a thyroid nodule. An FNAC of the same did not show any evidence of malignancy. She underwent a right hemithyroidectomy. As postoperative histopathology revealed multifocal papillary carcinoma of thyroid she was advised to undergo completion thyroidectomy, however she defaulted further treatment. After a period of five months she presented to us with swelling on both sides of the neck and had developed hoarseness over the last three months. Contrast enhanced CT of the neck and thorax revealed a heterogenous soft tissue lesion in the region of the left lobe of thyroid and bilateral significant cervical lymphadenopathy. FNAC of the node showed papillary carcinoma thyroid. Flexible endoscopy evaluation revealed left vocal cord palsy alone. She underwent completion thyroidectomy with bilateral comprehensive neck dissection. The left recurrent laryngeal nerve was seen to be entering the tumor and could not be salvaged. The thyroid was seen to be adherent to the first tracheal cartilage on the left side and the anterior wall of the same was excised. Cut ends of the trachea were sutured primarily and reinforced with strap muscles. Tracheostomy was done. Guardian sutures were deferred as there was no tension at the anastomosis. The patient was nursed with her neck flexed during the postoperative stay. She was discharged one week postoperatively and decannulated a week later. Her histopathology report showed evidence of conventional papillary carcinoma thyroid with extra capsular invasion and infiltration of tracheal cartilage with no intramural extension. Bilateral Jugular group of lymph nodes showed evidence of metastasis. She too received high dose radio Iodine ablation and is now on regular follow up.
Discussion
Originally meant for resolution of benign tracheal stenosis, tracheal resection with an end-to-end anastomosis is now widely used to treat tracheal tumors. The pioneers of this technique were Dr. Hermes Grillo and Dr. Joel Cooper in the 1960s. Since then, many significant advancements in airway management and in maneuvers to obtain a tension-free anastomosis have been achieved [10]. However, it is imperative for the treating surgeon to be well versed with the anatomy of the involved field before venturing into the same.
The trachea has a D-shaped cross-section structure consisting of 16 to 20 incomplete, horseshoe-shaped cartilaginous rings anteriorly and laterally with a membranous wall posteriorly. The trachealis muscle lines between the membranous wall and the esophagus. Intercartilaginous membranes connect each cartilaginous ring [11].
The blood supply is segmental and approaches laterally and divides longitudinally into superior and inferior branches. The branches anastomose with the segmental arteries above and below. At the same time, the arteries branch anteriorly and posteriorly within the intercartilaginous membrane and anastomose to the contralateral side [11].
The most common indication for tracheal resection surgery still is subglottic/tracheal stenosis unresponsive to balloon dilatation or CO2 laser scar excision. Resection of malignant tumor is another indication and is the preferred modality wherever feasible. Radiotherapy and chemotherapy are reserved for subjects with extensive disease or when the patient is unfit for such a surgery. Other less common indications include airway trauma, inhalation burns, radiation injury, tracheoesophageal/tracheoinnominate fistulas and congenital lesions [11].
Role of Endoscopy and Imaging in evaluation of extent of involvement
While planning for surgery, it is of utmost importance to know the precise extent of the disease and assess the feasibility of a primary anastomosis. A thorough evaluation with endoscopy and imaging is mandatory. Ishihara et al [12] recommend endoscopic examination of the trachea and stress the difficulty of accurately assessing the extent of invasion by this technique. Nakao et al [13] recommend endoscopy and computed tomography as part of the preoperative evaluation of a patient. They also stress the need to examine the margins of the resected trachea with frozen sections, as proposed by Mathey et al,[14].
Transcutaneous ultrasonography is another technique that can detect the depth of airway invasion, reliably distinguishing superficial (Shin I-II) vs. deeper (Shin III-IV) infiltration with a diagnostic accuracy potentially reaching 93% [15].
Securing the Airway
The peculiar problem while operating on trachea is securing the airway as it is shared both by anesthetist and surgeon. The conventional method is bypassing the endotracheal tube beyond the growth or passing the tube after incising the trachea distal to the growth [16]. Other techniques include high-frequency jet ventilation, rigid bronchoscopy, and laryngeal mask airway and cardiopulmonary bypass [9].
Resection and anastomosis
When the trachea is involved in the cervical segment, a cervical approach provides adequate access. Inferior extension mandates a sternotomy or even a thoracotomy. Adequate margins for disease clearance have to be ascertained. It is advisable to use the help of a frozen section whenever feasible.
Complete resection rates ranging from 42 to 57% have been reported in a few series [17]. However, a high incidence of R1 or R2 resection rates have also been noted because of late detection of the tumor, complex anatomy, and surgeons not being exposed to this particular pathology [9].
The next most crucial step in this procedure is to achieve a tension free anastomosis. Various release maneuvers have been described for this purpose. These include anterior and posterior blunt tracheal dissection, neck flexion, thyrohyoid, suprahyoid, hilar, and intrapericardial release techniques [11].
Mullikan et al. showed up to 4.5 cm of the trachea can be resected with tension-free anastomosis with neck flexion alone [18].
The thyrohyoid or suprahyoid laryngeal release allows the larynx to drop caudally and add 1 to 2 cm of tracheal length. However, the suprahyoid release is preferred as it provides a similar length without risking injury to the superior laryngeal vessels and nerve [11].
Complications
Auchincloss et al. [19] in their study showed a median postoperative hospital stay of 8 days, a success rate of 95%, and a complication rate of 18.2%.
Anastomotic dehiscence is the most dreaded complication. Its incidence ranges from 4% to 14% with a mortality of 7.8% [20]. The length of the resected tracheal segment is directly correlated with the tension over the suture line. Tracheal resections longer than 4 cm are associated with a remarkable rise of anastomotic dehiscence rate [21].To prevent this continuous neck flexion should be maintained using the guardian stitch, mechanical ventilation with paralytics, neck brace or posterior neck plaster splint. Patients can usually be extubated 1-7 days later. However, if the surgeon feels that an early extubation is unlikely a tracheostomy can be performed ensuring a distance of 2 cm from the anastomosis [11]. Another point to be borne in mind is preservation of the tracheal blood supply. The dissection should take place along the anterior wall and it should be limited only to the resected segment. Piazza et al. suggest dissecting no more than 1 cm from the residual stumps [22]. Some surgeons cover anastomotic line with musculocutaneous flap to preserve and protect tracheal anastomosis [21].
Restenosis can present in up to 10% of patients and is the most common complication of tracheal resection, possibly due to granulation tissue development at the suture line [11].
Wound infection can present with erythema, drainage, and increased pain. Treatment involves a culture of the wound, antibiotics. Tracheoinnominate or tracheoesophageal fistula can result due to anastomotic dehiscence and needs to be addressed immediately [11].
In all the three cases described here, the extent of tracheal involvement was limited, hence it was possible to adequately resect the tumor and anastomose primarily. Critical points to remember while performing such a procedure are to know the exact site and extent of the tumor. A sound anatomical knowledge of blood supply is equally important. To avoid any undue tension over the anastomosis one should ascertain adequate neck flexion and be aware of the various release maneuvers available which will ensure the additional length for tension free safe anastomosis.
Conclusion
In most tracheal malignancies the symptom presentation is often misleading and a correct diagnosis may be delayed by months to years. Clinical suspicion plays a fundamental role and endoscopic and CT evaluation remain the cornerstones in the diagnosis. Appropriate surgical resection and reconstruction is still the best modality to achieve long term survival with a decent quality of life. However this remains a challenging procedure and an in-depth knowledge of surgical and reconstruction techniques is absolutely essential.
Disclosure
This material has never been published and is not under evaluation in any other peer-reviewed publication.
Use of Generative AI
Generative AI was not used to write this article.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors declare no conflicts of interest.
References
1. Nouraei SM, Middleton SE, Nouraei SA, et al. Management and prognosis of primary tracheal cancer: a national analysis. Laryngoscope 2014;124:145-50. [PubMed] [Google Scholar]
2. Junker K. Pathology of tracheal tumors. Thorac Surg Clin 2014;24:7-11. [PubMed] [Google Scholar]
3. Thompson AD, Talavari Y, Mehari A, et al. Tracheal cancer mortality and trends in the United States. Internet J Oncol 2014;10:1-2. [Google Scholar]
4. Urdaneta AI, Yu JB, Wilson LD. Population based cancer registry analysis of primary tracheal carcinoma. Am J Clin Oncol 2011;34:32-7. [PubMed] [Google Scholar] [Ref list]
5. Webb BD, Walsh GL, Roberts DB, et al. Primary tracheal malignant neoplasms: the University of Texas MD Anderson Cancer Center experience. J Am Coll Surg 2006;202:237-46. [PubMed] [Google Scholar] [Ref list]
6. Shadmehr MB, Farzanegan R, Graili P, et al. Primary major airway tumors; management and results. Eur J Cardiothorac Surg 2011;39:749-54. [PubMed] [Google Scholar] [Ref list]
7. Matsumoto F, Ikeda K. Surgical Management of Tracheal Invasion by Well-Differentiated Thyroid Cancer. Cancers (Basel). 2021 Feb 14;13(4):797. doi: 10.3390/cancers13040797. PMID: 33672929; PMCID: PMC7918429.
8. Chen, Y. et al. (2024) Case report: A novel perspective on the treatment of primary tracheal small cell carcinoma: A patient’s experience with immuno-combined EP therapy and literature review, Frontiers. Available at: https://doi.org/10.3389/fimmu.2024.1356268 (Accessed: 03 July 2024).
9. Parshad, S., Gogna, S., Saroha, V., Lohchab, S. S., & Karwasra, R. K. (2020). Tracheal Resection and Reconstruction for Malignant Tumor. Indian Journal of Surgical Oncology, 11(S2), 199–203. doi:10.1007/s13193-020-01124-4
10. Tracheal resection and anastomosis for squamous cell carcinoma [Internet]. MMCTS. [cited 2024 Jul 4]. Available from: https://mmcts.org/tutorial/1719
11. Young A, Bigcas JLM. Tracheal Resection [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK563234/
12. Ishihara TKikuchi KIkeda T et al. Resection of thyroid carcinoma infiltrating the trachea. Thorax. 1978;33378- 386 Google Scholar Crossref
13. Nakao KMiyata MIzukura MMonden YMaoda MKanashima Y Radical operation for thyroid carcinoma invading the trachea. Arch Surg. 1984;1191046- 1049
ArticleGoogle ScholarCrossref
14. Mathey JBinet JPGaley JJEvrard CLemoine GDenis S Tracheal and tracheobronchial resections: technique and results in 20 cases. J Thorac Cardiovasc Surg. 1966;511- 13 Google Scholar
15. Piazza C, Lancini D, Tomasoni M, D’Cruz A, Hartl DM, Kowalski LP, et al. Tracheal and Cricotracheal Resection With End-to-End Anastomosis for Locally Advanced Thyroid Cancer: A Systematic Review of the Literature on 656 Patients. Frontiers in Endocrinology [Internet]. 2021 [cited 2023 Aug 30];12:779999. Available from: https://pubmed.ncbi.nlm.nih.gov/34858348/
16. Zhu B, Ma LL, Ye TH, Huang YG (2010) Anesthesia management of tracheal resection. Chin Med J 123:3725–3727
17. Yasumatsu R, Fukushima J, Nakashima T, Kadota H, Segawa Y, Tamae A, Kato M, Komune S (2012) Surgical management of malignant tumors of the trachea: report of two cases and review of literature. Case Rep Oncol 5(2):302–307
18. Mulliken JB, Grillo HC. The limits of tracheal resection with primary anastomosis: further anatomical studies in man. J Thorac Cardiovasc Surg. 1968 Mar;55(3):418-21. [PubMed] [Reference list]
19. Auchincloss HG, Wright CD. Complications after tracheal resection and reconstruction: prevention and treatment. J Thorac Dis. 2016 Mar;8(Suppl 2):S160-7. [PMC free article] [PubMed] [Reference list]
20. Gerwat J, Bryce DP. The management of subglottic laryngeal stenosis by resection and direct anastomosis. Laryngoscope 1974;84:940-57. [Crossref] [PubMed]
21. Rotolo, N., Cattoni, M., & Imperatori, A. (2017). Complications from tracheal resection for thyroid carcinoma. Gland Surgery, 6(5), 574–578. doi:10.21037/gs.2017.08.05
22. Piazza C, Del Bon F, Barbieri D, et al. Tracheal and Crico-Tracheal Resection and Anastomosis for Malignancies Involving the Thyroid Gland and the Airway. Ann Otol Rhinol Laryngol 2016;125:97-104. [Crossref] [PubMed].
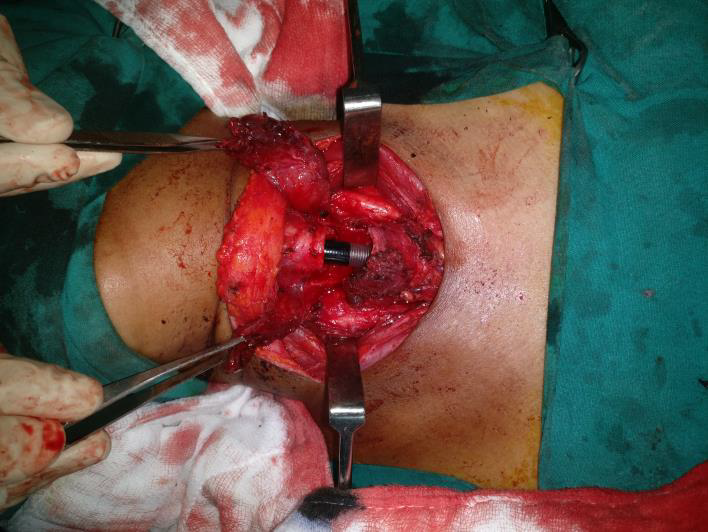
Figure 1

Figure 2

Figure 3

Figure 4