Ormond’s Disease: A Challenging Diagnosis.
Ormond’s Disease: A Challenging Diagnosis.
Mayco da Silva Botaro 1, Fauzia F. Naime2*
1. Internal Medicine Resident at the Mandaqui Hospital Complex. https://orcid.org/0009-0009-6663-8772
*Correspondence to: Fauzia F. Naime, Clinical Oncologist at the Paulista Institute of Oncology and the Dr. Arnaldo Vieira de Carvalho Cancer Institute (ICAVC). Medical Residency Preceptor at the Mandaqui Hospital Complex and ICAVC. Master's degree in Oncology. Professor at the School of Medicine of Nove de Julho University. https://orcid.org/0000-0002-7944-8689
Copyright.
© 2025 Fauzia F. Naime This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 Sep 2025
Published: 17 Sep 2025
DOI: https://doi.org/10.5281/zenodo.17287939
Abstract
Background: Ormond’s disease, or retroperitoneal fibrosis, is a rare inflammatory condition frequently associated with ureteral obstruction and progressive renal dysfunction. In its IgG4-related form, it may mimic malignant, infectious, or autoimmune processes, making diagnosis particularly challenging.
Case Presentation: We report the case of a 61-year-old male patient with progressive weight loss, abdominal pain, and vomiting, who developed acute kidney injury secondary to bilateral ureteral obstruction. Imaging revealed a retroperitoneal mass encasing the ureters and major vessels. Multiple biopsies confirmed chronic inflammation with fibrosis and IgG4-positive plasma cell infiltration, establishing the diagnosis of IgG4-related retroperitoneal fibrosis. Despite partial improvement with corticosteroid therapy and relief of obstruction through nephrostomy and double-J catheter placement, the patient progressed to chronic kidney failure requiring long-term hemodialysis. During treatment, he also developed severe infectious complications, including infective endocarditis requiring cardiac surgery. Rituximab therapy was subsequently indicated due to refractory disease.
Discussion: IgG4-related retroperitoneal fibrosis shares clinical and radiological features with malignant and infectious disorders, making histopathology and immunohistochemistry essential for definitive diagnosis. First-line treatment with glucocorticoids often leads to clinical improvement, although fibrotic tissue is less responsive, highlighting the importance of early diagnosis. In refractory cases, immunosuppressants such as rituximab and mycophenolate mofetil have shown promising results.
Conclusion: This case illustrates the severe clinical course of IgG4-related Ormond’s disease, emphasizing the need for early recognition, histopathological confirmation, and timely initiation of therapy. Multidisciplinary management is critical to preventing irreversible complications, such as chronic kidney failure, and improving patient outcomes.
Keywords: Retroperitoneal fibrosis, Ormond’s disease, IgG4-related disease, hydronephrosis, chronic kidney failure.
Ormond’s Disease: A Challenging Diagnosis.
Introduction
Ormond’s disease, or retroperitoneal fibrosis, is a rare condition first described by John Ormond in 1948.1 IgG4-related diseases may be idiopathic or secondary to infections, autoimmune disorders, neoplasms, trauma, radiotherapy, surgeries, and the use of certain medications such as methysergide, bromocriptine, ergotamine, methyldopa, hydralazine, analgesics, or β-blockers2,3. The incidence is 1.3 per 100,000, and it usually affects individuals between 40 and 60 years of age, with a slight male predominance.4
Idiopathic retroperitoneal fibrosis (IRF) is currently classified within a group of conditions known as chronic periaortitis. The three main components of chronic periaortitis are IgG4-related idiopathic retroperitoneal fibrosis, IgG4-related abdominal aortitis, and IgG4-related perianeurysmal fibrosis.5
The fibrosis typically begins at the level of the fourth lumbar vertebra and then spreads toward the renal hilum, encasing the ureters and other abdominal organs.6,7 In most cases, it is detected during the evaluation of acute kidney injury or hypertension.8 Ureteral involvement is reported in 80 to 100% of cases, being the most common and severe complication.2
Clinical manifestations of the disease may be nonspecific, such as fatigue, weight loss, low-grade fever, and general malaise, which hinders diagnosis.1 The most common presentations include poorly localized pain in the back, flanks, lower abdomen, or thighs; leg edema; and hydronephrosis due to ureteral involvement. The most frequently affected sites are the periaortic regions, periureteral areas, and plaque-like masses encasing the retroperitoneum.5
Diagnosis requires a combination of histopathology, immunohistochemistry, and imaging. The presence of IgG4-positive plasma cells and fibrotic findings are characteristic of the IgG4-related form.9
Computed tomography (CT) and magnetic resonance imaging (MRI) are the imaging modalities of choice, capable of identifying fibrotic retroperitoneal masses often located anterior to the abdominal aorta and encasing the ureters. On CT, fibrous tissue enhancement varies according to disease stage: more vascularized with good contrast enhancement in early stages, and showing mild enhancement in long-standing fibrosis.10
MRI provides better definition of fibrotic tissue compared to surrounding structures, especially when fat-saturation sequences are used. PET-CT may be useful to assess inflammatory activity and monitor therapeutic response.2
From an epidemiological perspective, although rare, Ormond’s disease is underdiagnosed due to its nonspecific presentation and the lack of familiarity of most clinicians with the condition. In addition to its predominance in middle-aged men, studies suggest an association with other autoimmune and inflammatory disorders, such as Hashimoto’s thyroiditis, vasculitis, and rheumatologic diseases, reinforcing the need for comprehensive clinical evaluation.2
We present a case of Ormond’s disease confirmed by histopathology and immunohistochemistry, associated with severe renal complications.
Case Report
In early November 2023, a 61-year-old male patient was admitted to the emergency department of a public hospital near his residence with severe abdominal pain, vomiting, decreased urine output, reduced appetite, and a weight loss of 20 kg in one month. He had experienced mild abdominal pain and occasional vomiting over the past 6 months, having sought care at the same facility on two previous occasions, where he was treated on an outpatient basis with symptomatic medication.
During the diagnostic workup at that hospital in November 2023, the patient presented with acute kidney injury (AKI) and urinary tract infection. An initial abdominal ultrasound revealed a retroperitoneal mass in the periaortic region, causing extrinsic compression of the ureters. The patient underwent hemodialysis (4 sessions) followed by placement of a double-J catheter in the right ureter due to extrinsic compression from the mass. He showed improvement in renal function and was also treated for the urinary infection. He was discharged from that institution to continue outpatient treatment.
In December 2023, he presented to our public hospital with abdominal pain and vomiting refractory to medication. A non-contrast abdominal CT scan revealed bilateral ureterohydronephrosis up to the mid-ureter and a lymph node conglomerate (Figure 1). Laboratory tests showed anemia (Hb 9.3 g/dL), leukocytosis (20,450/mm³), hyperkalemia (K+ 8.3 mEq/L), elevated urea (204 mg/dL) and creatinine (3.3 mg/dL), C-reactive protein (4.5 mg/dL), and urinalysis with >1 million leukocytes, 160,000 red blood cells, and abundant bacteria (+++). The patient received clinical treatment for acute kidney injury, including initial management of hyperkalemia with conservative measures, followed by hemodialysis due to refractoriness. He was treated with antibiotic therapy for the urinary tract infection.
Figure 1. Abdominal Magnetic Resonance Imaging: Irregular solid mass located in the retroperitoneum, measuring approximately 8.7 × 2.8 × 5.8 cm, involving vascular structures such as the abdominal aorta and inferior vena cava. The lesion causes marked bilateral hydronephrosis. Bilateral renal cysts (Bosniak 1 and 2), diffuse thickening of the bladder wall, and an enlarged prostate are also observed. Findings are compatible with a retroperitoneal expansive/infiltrative process.
During the first 2 days, the patient showed clinical and laboratory worsening (progression of anemia, increased leukocytosis and CRP, worsening renal function, and hyperkalemia of 8.0). Placement of a “Shilley” dialysis catheter and continuation of hemodialysis were indicated. Differential diagnoses included lymphomas, sarcomas, and retroperitoneal metastases from gastrointestinal carcinomas, among others.
In January 2024, a laparoscopic biopsy of a mesenteric lymph node was performed, and histopathology revealed chronic inflammatory process with fibrosis, follicular hyperplasia, and chronic reactive lymphadenitis, with no evidence of neoplasia. Immunohistochemistry showed chronic reactive lymphadenitis, peritoneum without neoplasia, and mild chronic inflammation with fibrosis. A bone marrow biopsy was also performed, revealing lymphocytosis without neoplasia.
The double-J catheter was replaced, and bilateral nephrostomy was performed on 01/24/2024. The last hemodialysis session in this phase was on 01/29/2024. During hospitalization, the patient underwent upper gastrointestinal endoscopy and colonoscopy, both of which were unremarkable. In February, the patient lost the left nephrostomy tube and remained dialysis-free until March 2024, when refractory hyperkalemia required resumption of hemodialysis.
A new biopsy was necessary and performed on 03/20/2024 of the retroperitoneal mass via laparoscopy. Intraoperative frozen section examination revealed proliferation of spindle cells without atypia, with deposition of dense collagen permeated by mild lymphomononuclear inflammatory infiltrate. The final immunohistochemistry result, obtained only on 05/07/2024, demonstrated chronic inflammation with fibrosis, presence of IgG4-positive plasma cells (up to 14 per HPF, approximately 70% of plasma cells counted), suggesting IgG4-related disease (Table 1).
Table 1 - Immunohistochemistry
|
Clone |
Resultados |
|
|
CK AE1/AE2 |
AE1/AE2 |
Negative |
|
Desmina |
D33 |
Negative |
|
Actina 1A4 |
1A4 |
Positive |
|
Prot.S100 |
Policlonal |
Negative |
|
CD34 |
QBEND10 |
Vessels |
|
Beta-Catenin |
BETA-CATENIN-1 |
Negative |
|
Ki-67 |
MIB-1 |
5% |
|
CD20 |
L26 |
Rare cells |
|
CD3 |
Policlonal |
Numerosos linfócitos |
|
PAX-5 |
DAK-PAX-5 |
Rare cells |
|
Caldesmon |
H-CD |
Negative |
|
Calponina |
CALP |
Rare cells |
|
CD68 |
KP1 |
Focal |
|
Factor XIIIa |
EP3372 |
Positive |
|
ALK-1(CD246) |
ALK-1 |
Negative |
|
CD138 |
MI15 |
Up to 20% of plasma cells per HPF |
|
AA-ref A P O I O |
- |
IgG4 in 14 plasma cells per HPF |
After discharge from our institution, the patient was referred to another hospital with specialties in oncology/hematology, rheumatology and nephrology. He continues to undergo outpatient hemodialysis three times a week and has been maintained on prednisone 20 mg/day for over one year, with significant reduction of retroperitoneal fibrosis (Figures 2 (before) and Figure 3 (after)
Figure 2. Total abdominal computed tomography: Examination performed at the onset of the condition, prior to treatment, showing bilateral hydronephrosis and a large retroperitoneal mass.
Figure 3. Total abdominal computed tomography: Image obtained after initiation of corticosteroid therapy, showing improvement of hydronephrosis and significant reduction in the size of the retroperitoneal mass.
Discussion
IgG4-related diseases mimic many malignant, infectious, and inflammatory conditions. Histopathology is essential for diagnosis. The pathological hallmarks of the disease are lymphoplasmacytic infiltration, storiform fibrosis, and obliterative phlebitis.
Currently, Ormond’s disease, or retroperitoneal fibrosis, is classified as an IgG4-related disease, which may be idiopathic (two-thirds of cases) or secondary to infections, neoplasms, or autoimmune diseases. It is a chronic inflammatory condition characterized by tissue infiltration with IgG4-positive plasma cells, fibrosis, and often elevated serum IgG4 levels. The inflammatory process affects the infrarenal portion of the abdominal aorta and the iliac arteries, and infiltrates involving the ureters and the inferior vena cava are also commonly observed.1
The three central pathological features are lymphoplasmacytic infiltration, obliterative phlebitis, and storiform fibrosis. Lymphocytes and plasma cells are polyclonal, eosinophils are often present, and neutrophilic infiltration is rare.11 Fibrosis is a histopathological condition required for diagnosis, presenting with a typically irregular distribution and storiform pattern, characterized by collagen fibers arranged radially and interlaced within the tissue — a unique pattern associated with IgG4-related disease.9
In the idiopathic form, the pathophysiology is not yet fully understood, although an autoimmune response is believed to be involved. Lymphocyte and plasma cell infiltration accompanied by a cytokine-mediated inflammatory reaction appears to be the central mechanism of pathogenesis. Tissue infiltration by IgG4-positive plasma cells, as well as elevated serum levels of this immunoglobulin, may be observed in some cases; however, IgG4 presence is not exclusive to the disease.1 Serum IgG4 levels are not sufficiently sensitive or specific. Plasma IgG4 concentrations may vary from normal to elevated depending on the site of involvement. Monitoring serum IgG4 levels may be useful for assessing disease activity but should not be used in isolation for therapeutic decisions.12 Systematic reviews, such as that of Umehara et al. (2012)13, emphasize the importance of biomarkers such as serum IgG4 in helping to differentiate this condition from other causes of retroperitoneal fibrosis.
Tissue biopsy is the gold standard for diagnosis. Imaging exams such as contrast-enhanced computed tomography, magnetic resonance imaging, and PET-CT are important for the diagnostic approach across multiple organs, and differentiating IgG4-related disease from malignant tumors is essential.
The main differential diagnoses in this case include lymphomas, sarcomas, sarcoidosis, histiocytosis, drug-induced tubulointerstitial nephritis, idiopathic membranous glomerulonephritis, among others.
First-line standard treatment is glucocorticoids, aimed at attenuating or halting the chronic inflammatory process. The initial dose of prednisolone is generally 0.6–1.0 mg/kg per day.14,15 After 2 to 4 weeks, the dose is reduced by 5 mg every 1 to 2 weeks, according to clinical response. A longer course of glucocorticoid therapy may be necessary. Clinical manifestations generally respond rapidly, with significant improvement in inflammatory lesions and recovery of affected organ function. However, retroperitoneal fibrosis is less responsive to glucocorticoid therapy, which underscores the importance of early diagnosis and treatment.16
If patients do not respond to corticosteroids, literature recommends the use of antiestrogenic agents such as tamoxifen or immunosuppressants such as azathioprine and cyclophosphamide.17 The extent of fibrosis is a determining factor in treatment response; however, in refractory cases or in those showing little improvement with corticosteroids, immunosuppressants such as rituximab and mycophenolate mofetil are used as alternatives. Zhang et al. (2020)18 reported successful outcomes with rituximab in patients with IgG4-related retroperitoneal fibrosis.
This case illustrates the typical progression of IgG4-related Ormond’s disease, from bilateral urinary obstruction to chronic renal failure. In patients with renal failure due to obstructive uropathy, relieving the obstruction is essential to preserving renal function. Histopathology and immunohistochemistry confirmed the diagnosis, underscoring the relevance of detailed diagnostic investigation. Although initial management provided partial relief of obstruction, the patient’s course was marked by complications such as refractory hyperkalemia and recurrent infections. The presented case showed a more severe progression, with established chronic renal failure, due to delayed diagnosis and initiation of specific treatment.
Retroperitoneal fibrosis should be considered as a manifestation of systemic disease because of its potential to affect multiple organs. Studies suggest that early diagnosis and aggressive management can prevent irreversible complications.19
Conclusion
Ormond’s disease, particularly in its IgG4-related form, remains a rare and challenging condition that can lead to severe complications such as chronic kidney failure. Given its ability to mimic malignant, infectious, and inflammatory disorders, it should always be included in the differential diagnosis of retroperitoneal masses of uncertain origin. Early recognition and prompt initiation of treatment are crucial to prevent irreversible organ damage and improve patient outcomes.
References
1. Pr?cha M, Kolombo I, Štádler P. Ormond's Disease--IgG4-related Disease. Prague Med Rep. 2015;116(3):181-92. doi: 10.14712/23362936.2015.57
2. Vaglio A, Salvarani C, Buzio C. Retroperitoneal fibrosis. Lancet 2006;
367: 241–251.
3. Heckmann M, Uder M, Kuefner MA, Heinrich MC. Ormond's disease or secondary retroperitoneal fibrosis? An overview of retroperitoneal fibrosis. Rofo. 2009 Apr;181(4):317-23.
4. van Bommel EFH, Jansen I, Hendriksz TR, Aarnoudse ALHJ. Idiopathic retroperitoneal fibrosis: prospective evaluation of incidence and clinicoradiologic presentation.. Medicine (Baltimore). 2009 Jul;88(4):193-201.
5. Kamisawa T, Zen Y, Pillai S, Stone JH. IgG4-related disease.Lancet. 2015 Apr 11;385(9976):1460-71.
6. Amis Jr ES. Retroperitoneal fibrosis. Am J Roentgenol 1991; 157: 321– 329.
7. Gilkeson GS, Allen NB. Retroperitoneal fibrosis. A true connective tissue disease. Rheum Dis Clin North Am 1996; 22: 23–38
8. van Bommel EF. Retroperitoneal fibrosis. Neth J Med 2002; 60: 231– 242.
9. Zen Y, Nakanuma Y. IgG4-related disease: a cross-sectional study of 114 cases. Am J Surg Pathol 2010; 34: 1812–19.
10.Vivas I, Nicolas AI, Velazquez P et al. Retroperitoneal fibrosis: typical and atypical manifestations. Br J Radiol 2000; 73: 214–222
11. Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol 2012; 25: 1181–92.
12. Kamisawa T, Shimosegawa T, Okazaki K, et al. Standard steroid treatment for autoimmune pancreatitis. Gut 2009; 58: 1504–07.
13. Umehara H, Okazaki K, Masaki Y, Kawano M; Research Program for Intractable Disease by Ministry of Health, Labor and Welfare (MHLW) Japan G4 team. A novel clinical entity, IgG4-related disease (IgG4RD): general concept and details. Mod Rheumatol. 2012;22(1):1–14.
14. Shimosegawa T, Chari ST, Frulloni L, et al, and the International Association of Pancreatology. International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology. Pancreas 2011; 40: 352–58
15. Kamisawa T, Shimosegawa T, Okazaki K, et al. Standard steroid treatment for autoimmune pancreatitis. Gut 2009; 58: 1504–07.
16. Shimizu Y, Yamamoto M, Naishiro Y, et al. Necessity of early intervention for IgG4-related disease–delayed treatment induces fi brosis progression. Rheumatology (Oxford) 2013; 52: 679–83.
17. Heckmann M, Uder M, Kuefner MA, Heinrich MC . Ormond's disease or secondary retroperitoneal fibrosis? An overview of retroperitoneal fibrosis. Rofo. 2009 Apr;181(4):317-23
18. Zhang W, Stone, J. H., & XU, T. Efficacy of rituximab in IgG4-related disease: A retrospective analysis of 12 patients. Clinical Rheumatology, 2020; 39(2), 495-503.
19. Runowska M, Majewski D & Puszczewicz M. Retroperitoneal fibrosis: The role of IgG4-related disease, idiopathic, and secondary causes. Frontiers in Immunology, 2019;10, 1615.
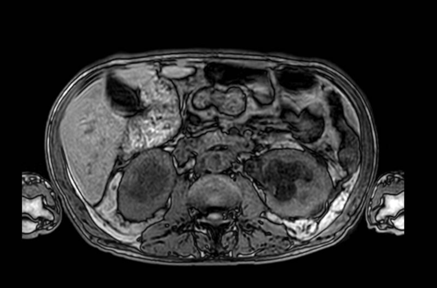
Figure 1
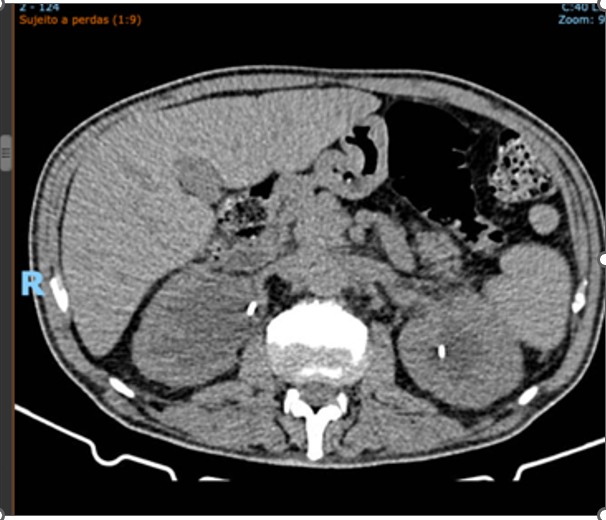
Figure 2
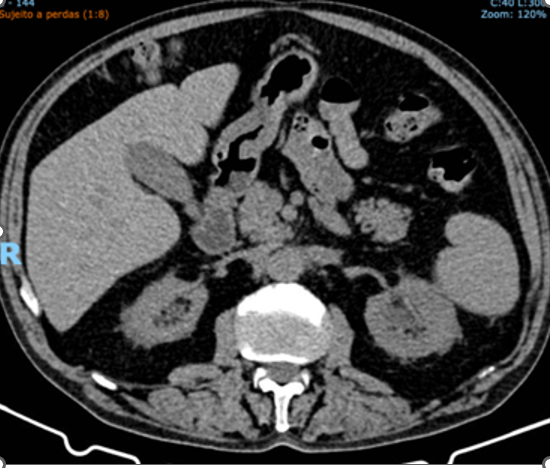
Figure 3