An Unusual Case of Recurrent Bloody Nipple Discharge in an 11-Year-Old Girl.
An Unusual Case of Recurrent Bloody Nipple Discharge in an 11-Year-Old Girl.
Fatimah Jafer Hassan Almabyouq1, Tafe Adel Badghaish2*, Walaa Salman Alsharrah3, Zahrh Faisal Abualsaud4
1, 4. Department of Pediatric Surgery, King Fahad Hospital of the University, Imam Abdulrahman Bin Faisal University, KSA.
2. College of Medicine, Alfaisal University, Riyadh, KSA.
3. College of Medicine, Imam Abdulrahman Bin Faisal University, KSA.
*Correspondence to: Tafe Adel Badghaish, lege of Medicine, Alfaisal University, Riyadh, KSA.
Copyright.
© 2025 Tafe Adel Badghaish, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 Aug 2025
Published: 17 Sep 2025
DOI: https://doi.org/10.5281/zenodo.17301619
Abstract
Background: Bloody nipple discharge is defined as the secretion of blood or turbid fluid from the nipple. The discharge is associated with a variety of underlying medical conditions, ranging from common benign conditions such as duct ectasia and intraductal papilloma to rarer causes, including breast cancer.
Case Presentation: We report a rare instance of an 11-year-old girl who was presented with bloody nipple discharge from both breasts for two days associated with bilateral breast pain and menorrhagia. The girl is known to have bilateral duct ectasia and celiac disease. Ultrasound of bilateral breast revealed irregular heterogeneous glandular tissue extending away from the retroareolar region compatible with tanner stage III. As per the ultimate evaluation, Breast- Imaging Reporting and Data System is categorized as benign category 2. Furthermore, a bilateral breast magnetic resonance imaging with contrast demonstrated normal breast tissue.
Conclusion: Bloody nipple discharge in children associated with duct ectasia, is an uncommon breast symptom, especially in those with a history of systemic diseases such as celiac disease. This rare case emphasizes the necessity for further studies on pediatric patients with duct ectasia.
Keywords: Bloody Nipple Discharge, Duct Ectasia, Menorragia.
An Unusual Case of Recurrent Bloody Nipple Discharge in an 11-Year-Old Girl.
Introduction
Bloody nipple discharge is a clinical symptom that can be concerning for patients and complex for healthcare providers.1 It is characterized by the secretion of blood or turbid fluid from the nipple and can indicate various underlying conditions. The etiology of bloody nipple discharge can vary from benign conditions such as duct ectasia or intraductal papilloma to more serious pathologies like breast carcinoma.2
Despite its potential severity, many cases of bloody nipple discharge are linked to benign breast conditions.2 Understanding the differential diagnosis is crucial for appropriate management and treatment. The evaluation typically involves a thorough clinical examination, imaging studies, and sometimes biopsy, to ascertain the underlying cause.3
The presentation of bloody nipple discharge can vary widely in terms of associated symptoms, the pattern of discharge, and its unilateral or bilateral nature.4 Comprehending differential diagnosis is essential for proper therapy and management.2
Case Presentation
An 11-year-old patient with a known history of celiac disease presented to the emergency department (ED) with intermittent recurrent bilateral nipple discharge. The discharge commenced 14 days prior and continued for 5 days duration. The discharge was intermediate in quantity, exhibiting a bloody appearance, and was associated with breast swelling, pain and discomfort. The pain was characterized as dull and moderate in severity. No history of fever, prior trauma, or nipple retraction reported. Her family history was unremarkable. The mother provided a photograph of a stained bra.
In addition, mother reported having recurrent episodes of dysmenorrhea and menorrhagia.
Upon physical examination, the patient was conscious, alert and oriented. Vitally Within normal limits. Her Breast examination did not show palpable masses. There was smooth firm breast tissue present. No active discharge was observed from either breast, and there were no skin changes or palpable axillary lymphadenopathy. Laboratory investigation done and were within normal limits. (Table 1, 2)
US Breast and Axilla was done and showed irregular, heterogeneous glandular tissue extending from the retroareolar region, consisting with Tanner stage III. No significant or suspicious lumps or collections were observed. A central echogenic hilum was observed in both benign axillary lymph nodes. The final assessment classifies BI-RADS as benign category 2.
Patient was admitted for further investigation under the care of Pediatric Surgery. MRI Breast with Contrast was done and was unremarkable. A sample for Cytology from nipple discharge showed negative results.
The following services were consulted: Breast Surgery for assessing the bloody nipple discharge, Pediatric Endocrinology for investigating hormonal status, Pediatric Hematology to rule out bleeding tendency and Obstetrics and Genecology for menstrual complaints.
Breast surgery team evaluated the patient and confirmed the diagnosis of duct ectasia. She was given follow-up appointment as outpatient. The pediatric endocrinology team evaluated her for delayed menarche, observing normal development of secondary sexual characteristics and adrenarche, without any symptoms indicative of impaired puberty or abnormal progression.
Both Obstetric and Gynecology and Pediatric Hematology teams did reassurance since hemoglobin levels were normal and excluded the possibility of bleeding disorder.
Table 1 presents the laboratory investigations of the patient, all of which were within normal limits.( Fig 2)
The evaluation tests for bleeding disorders (Table 2) were within normal limits.
Table 2 illustrates the evaluation tests for bleeding disorders in the patient, all of which were within normal limits. (fig 3)
Patient kept following in the Pediatric surgery clinic with no active complaint for 1 year since discharge. she reported occasional breast pains with no further nipple discharge. follow-up US Breast and MRI were unremarkable.
Fig. 1 A) Axial T2-weighted breast MRI shows appearance of the patient’s breast. B) ADC normalization of both breasts is seen.
Discussion
This case involves a rare incident of turbid and bloody discharge from both nipples in an 11- year-old girl with a confirmed medical background of celiac disease and bilateral duct ectasia. This set of symptoms is not commonly seen together in children, which makes this case important for clinical practice.
Nipple discharge in pediatric patients is an uncommon finding, particularly when associated with duct ectasia.5 While duct ectasia typically occurs in middle-aged or elderly women and is rarely reported in children, its presence in this patient raises interesting questions.6 The literature on pediatric cases of duct ectasia is sparse, with most cases being incidental findings. Moreover, the association between duct ectasia and celiac disease has not been widely documented, suggesting that this case may represent a unique intersection of these conditions.7
The patient's bloody discharge, although alarming, was not associated with any suspicious masses on ultrasound or MRI, which is consistent with benign conditions reported in similar cases.1,5 The stability of imaging findings over two- and three-month intervals further supports the benign nature of the presentation. However, the recurrent nature of the symptoms, coupled with her history of menorrhagia, might suggest an underlying hormonal imbalance8 or other systemic conditions8 that could be contributing to her symptoms.
With the benign results on imaging (BI-RADS category 2) and no major issues found on MRI, treatment for this case should concentrate on reducing symptoms and closely monitoring the condition.8 Further examination is needed due to the recurring symptoms, especially considering the menorrhagia in the patient. Exploring hormonal therapy or other interventions to manage her menorrhagia and any related endocrine problems could be advantageous.9
The patient's past celiac disease raises questions about how her autoimmune status could be affecting her breast symptoms. While there is no clear proof connecting celiac disease to duct ectasia or nipple discharge, the autoimmune characteristics of celiac disease could make her more vulnerable to other inflammatory or ductal issues. This theory needs further investigation with more research and case studies.7
Limitations and Future Research
Our case was followed for more than 1 year and will continue following with Breast Surgery for the duct Duct Ectasia. Long-term monitoring is important to see if the patient's symptoms improve or continue and to uncover any possible long-term issues. Moreover, even though the imaging results remained unchanged, it could be worthwhile to investigate if utilizing more advanced imaging techniques or specific molecular indicators might offer further understanding of the cause of her symptoms.
Additional studies are required to gain a deeper comprehension of the connection between celiac disease and duct ectasia, especially in children. Conducting extensive studies or registries containing similar cases could assist in determining if this discovery is by chance or if there is a connected pathophysiological cause
Conclusion
This case highlights the importance of considering a broad differential diagnosis in pediatric patients presenting with unusual breast symptoms, particularly when there is a history of systemic conditions like celiac disease. The benign imaging findings and lack of significant changes over time are reassuring, but the recurrent symptoms and associated menorrhagia suggest that ongoing monitoring and possibly further hormonal evaluation are warranted. This case adds to the limited body of literature on pediatric duct ectasia and underscores the need for further research into its etiology and management in young patients.
References
1. Acer, T., Derbent, M., & Hiçsönmez, A. (2015). Bloody nipple discharge as a benign, self-limiting disorder in young children: A systematic review including two related case reports. Journal of Pediatric Surgery, 50(11), 1975–1982. https://doi.org/10.1016/j.jpedsurg.2015.08.049
2. ?mamoglu, M., Çay, A., Reis, A., Özdemir, O., Sapan, L., & Sarihan, H. (2005). Bloody nipple discharge in children: Possible etiologies and selection of appropriate therapy. Pediatric Surgery International, 22(2), 158–163. https://doi.org/10.1007/s00383-005-1559-6
3. Gupta, D., Mendelson, E. B., & Karst, I. (2021). Nipple discharge: Current clinical and imaging evaluation. American Journal of Roentgenology, 216(2), 330–339. https://doi.org/10.2214/ajr.19.22025
4. Patel, B. K., Falcon, S., & Drukteinis, J. (2015). Management of nipple discharge and the associated imaging findings. The American Journal of Medicine, 128(4), 353–360. https://doi.org/10.1016/j.amjmed.2014.09.031
5. Kitahara, S., Wakabayashi, M., Shiba, T., Nonaka, K., Nonaka, H., & Kobayashi, I. (2001). Mammary duct ectasia in children presenting bloody nipple discharge: A case in a pubertal girl. Journal of Pediatric Surgery, 36(6), 1–2. https://doi.org/10.1053/jpsu.2001.24011
6. Rahal, R. M., de Freitas-Júnior, R., Carlos da Cunha, L., Moreira, M. A., Rosa, V. D., & Conde, D. M. (2011). Mammary duct ectasia: An overview. The Breast Journal, 17(6), 694–695. https://doi.org/10.1111/j.1524-4741.2011.01166.x
7. Packova, B., Kohout, P., Dastych, M. et al. Malignant complications of celiac disease: a case series and review of the literature. J Med Case Reports 16, 460 (2022). https://doi.org/10.1186/s13256-022-03682-3
8. Kadir, R. A., & Lee, C. A. (2001). Menorrhagia in adolescents. Pediatric Annals, 30(9), 541–546. https://doi.org/10.3928/0090-4481-20010901-09
9. Albers, J. R., Hull, S. K., & Wesley, R. M. (2004, April 15). Abnormal uterine bleeding. American Family Physician. https://www.aafp.org/pubs/afp/issues/2004/0415/p1915.html
10. Themes, U. (2019, August 25). Management of Masses: BI-RADS 2, 3, or 4?. Radiology Key. https://radiologykey.com/management-of-masses-bi-rads-2-3-or-4/.
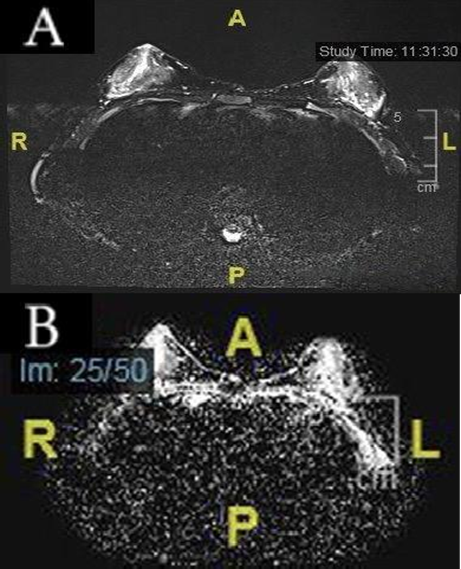
Figure 1
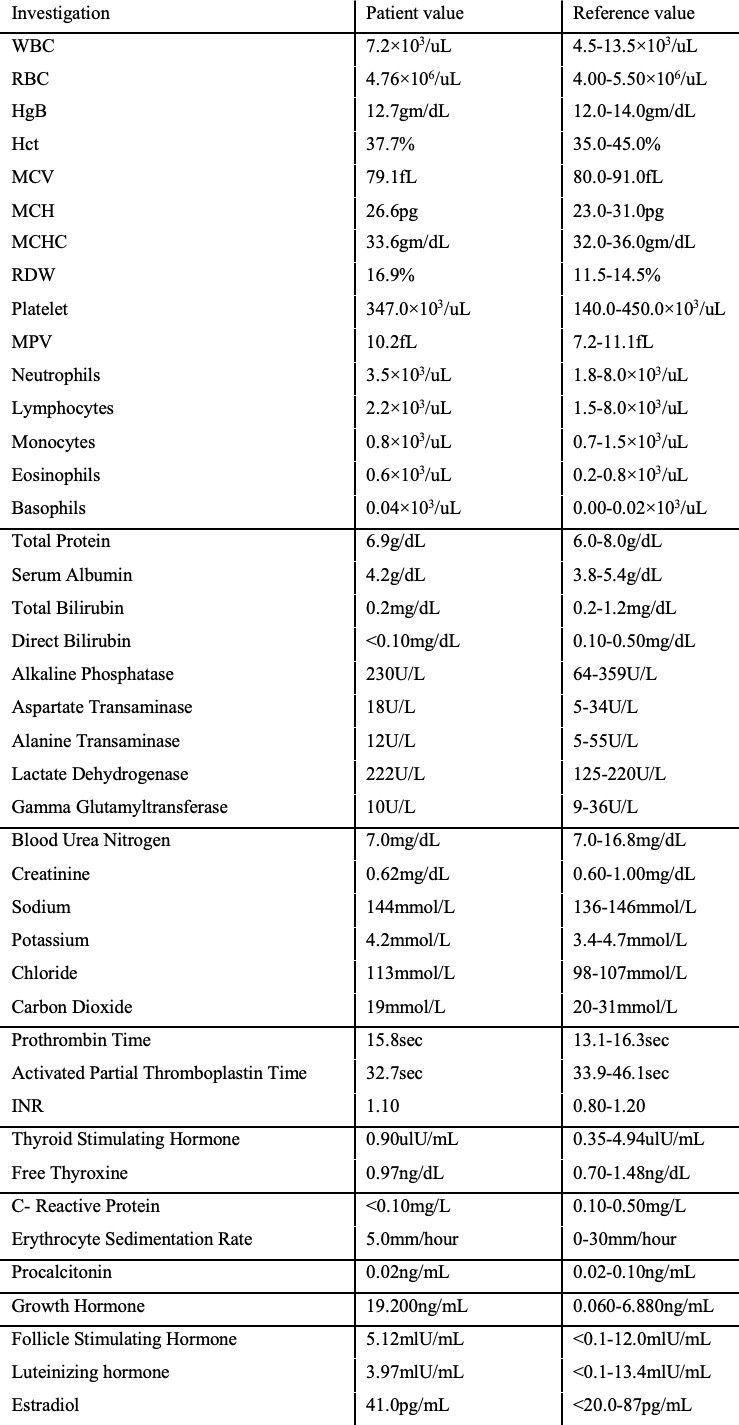
Figure 2
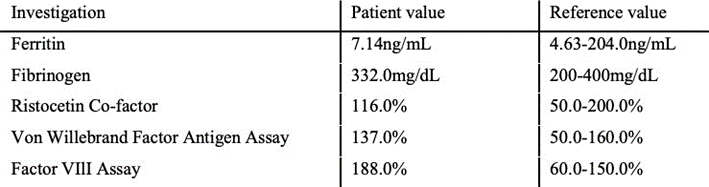
Figure 3