School-Based Interventions: A Systematic Review of Impact on Child and Adolescent Health Outcomes
School-Based Interventions: A Systematic Review of Impact on Child and Adolescent Health Outcomes
Sajeda Ansari*
*Correspondence to: Sajeda Ansari, Qatar.
Copyright
© 2025 Sajeda Ansari, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 Sep 2025
Published: 29 Sep 2025
DOI: https://doi.org/10.5281/zenodo.17302146
Abstract
School-based interventions are increasingly recognized as essential strategies to address the growing burden of physical, mental, and behavioral health challenges among children and adolescents. Schools provide structured environments that can reach large populations early in life and sustain preventive strategies over time. This review synthesizes evidence from systematic reviews and meta-analyses published between 2015 and 2025, assessing the impact of school-based interventions on health outcomes including obesity prevention, mental health, and behavioral well-being. The evidence demonstrates that such programs provide modest but clinically meaningful improvements in body mass index (BMI), anxiety and depression symptoms, post-traumatic stress disorder (PTSD), and risky behaviors such as smoking and bullying. However, heterogeneity in program design, follow-up length, and regional contexts limits comparability. Overall, school-based interventions remain a cornerstone of preventive health care in young populations, and efforts should now prioritize equity, sustainability, and cultural adaptability.
School-Based Interventions: A Systematic Review of Impact on Child and Adolescent Health Outcomes
Introduction
The school environment represents one of the most effective and accessible platforms for delivering public health interventions. Given that children and adolescents spend the majority of their waking hours in school settings, interventions embedded within the curriculum, extracurricular activities, and school infrastructure provide unique opportunities for early prevention of health problems. Over the past two decades, rising rates of adolescent obesity, sedentary behavior, anxiety, depression, and substance misuse have driven global interest in school-based programs as a means to combat both physical and psychological morbidity. The World Health Organization and several national health agencies have endorsed school-based health promotion as a cost-effective, population-wide strategy.
Several systematic reviews have demonstrated the effectiveness of such interventions. Programs targeting mental health have shown measurable but modest improvements in anxiety, depression, and PTSD outcomes, particularly when delivered universally rather than to high-risk groups. Physical health interventions, particularly those addressing nutrition and physical activity, have produced consistent reductions in BMI and improvements in weight-related outcomes when implemented over a sustained period. Behavioral interventions, such as whole-school anti-bullying campaigns and smoking prevention programs, have demonstrated reductions in risk-taking behaviors and improvements in school climate. Despite these successes, major challenges remain in terms of intervention fidelity, cultural adaptability, and sustainability across different socioeconomic contexts.
Methods
This review followed a structured approach to evidence synthesis. Four major databases—PubMed, Scopus, Web of Science, and PsycINFO—were searched for the period January 2015 to February 2025. The search strategy combined key terms such as “school-based intervention,” “school program,” “whole-school approach,” and “systematic review” or “meta-analysis.” Studies were included if they were systematic reviews or meta-analyses evaluating school-based interventions targeting children and adolescents aged 5 to 19 years. Eligible outcomes included physical health (e.g., obesity, BMI reduction, physical activity), mental health (e.g., anxiety, depression, PTSD), and behavioral health (e.g., substance use, bullying, risky sexual behavior). Narrative reviews, studies limited to higher education, and case reports were excluded.
A total of thirty-one systematic reviews and meta-analyses were identified, encompassing over 350 primary studies conducted across North America, Europe, Asia, Africa, and Latin America. Data were extracted on study design, intervention characteristics, outcomes, and effect sizes. Quality assessment of included reviews was based on AMSTAR-2 criteria, with most studies judged to be of moderate-to-high methodological quality.
Results
Mental Health Outcomes
Evidence from recent systematic reviews demonstrates that school-based interventions exert small but statistically significant effects on common adolescent mental health outcomes. A 2023 review by Grande and colleagues analyzed 39 studies across low- and middle-income countries (LMICs) and reported significant improvements in PTSD symptoms (standardized mean difference [SMD] = 0.61), although no significant benefits were observed for depression, anxiety, or attention-deficit/hyperactivity disorder (ADHD). Similarly, Hayes et al. in 2025 synthesized findings from 45 universal school-based programs and observed small reductions in anxiety (d = –0.086) and depression (d = –0.109). While effect sizes were modest, the population-level impact is potentially substantial given the broad reach of school programs. Cohen and colleagues (2024) highlighted that even brief interventions (≤4 sessions) could improve mental health outcomes, though questions remain about long-term sustainability.
Table 1. School-Based Mental Health Interventions
|
Review |
N Studies |
Target |
Effect Size |
Key Findings |
|---|---|---|---|---|
|
Grande 2023 |
39 |
PTSD, anxiety, ADHD, depression |
PTSD SMD = 0.61 |
PTSD improved, others NS |
|
Hayes 2025 |
45 |
Universal anxiety/depression |
d = –0.086 to –0.109 |
Small but significant |
|
Cohen 2024 |
28 |
Brief sessions (≤4) |
Varied |
Feasible, mixed efficacy |
Physical Health and Obesity Prevention
Physical health interventions targeting obesity and sedentary behavior were among the most widely studied. Ho et al. (2021) evaluated twelve cluster-randomized controlled trials and found that school-based obesity prevention programs were effective in reducing BMI, with a pooled effect size of g = 0.52, particularly in middle-income economies. Jacob et al. (2021) examined adolescent health education programs and noted mixed results; while some trials demonstrated significant reductions in BMI z-scores, others found no effect, underscoring the influence of socioeconomic and cultural differences. Moeller et al. (2024) reported that physical activity interventions significantly increased activity levels, but heterogeneity in intervention duration, type, and intensity limited comparability.
Table 2. School-Based Physical Health Interventions
|
Review |
N Studies |
Outcome |
Effect Size |
Summary |
|---|---|---|---|---|
|
Ho 2021 |
12 |
BMI |
g = 0.52 |
Effective in BMI reduction |
|
Jacob 2021 |
15 |
BMI z-score |
Mixed |
Some subgroup benefits |
|
Moeller 2024 |
18 |
PA levels |
Moderate |
Increased activity, variable |
Behavioral and Environmental Outcomes
School-based interventions have also been implemented to address risky behaviors and improve the school environment. Shackleton and colleagues (2016) conducted a comprehensive review and concluded that whole-school approaches significantly reduced teenage pregnancy, smoking, and bullying. Fernandes et al. (2023) examined environmental interventions, such as increasing green space and improving indoor air quality, and found consistent benefits for children’s health behaviors. Miller et al. (2024) reviewed digital mental health programs implemented in school contexts, highlighting feasibility and engagement but warning about inequalities in access to digital resources.
In addition to global findings, region-specific evidence from Gulf countries provides valuable insights into the effectiveness of school-based interventions. A large-scale obesity prevention initiative conducted in the United Arab Emirates between 2019 and 2022 targeted more than 1,200 schoolchildren aged 10 to 15 years. The program combined structured physical activity with nutritional education and demonstrated meaningful reductions in BMI, alongside significant improvements in physical activity levels. In Saudi Arabia, mindfulness and resilience-based interventions were introduced to 850 adolescents between 2020 and 2023. These interventions, although modest in effect, showed reductions in anxiety and stress scores, suggesting that mental health initiatives can be successfully implemented in culturally sensitive school environments. Similar patterns were observed in Qatar, where anti-smoking and health promotion programs were implemented between 2018 and 2021 among 950 high school students. These interventions reduced smoking initiation rates and improved awareness of risky lifestyle behaviors. In Kuwait, physical activity and health-awareness campaigns conducted from 2019 to 2021 engaged 780 students, leading to increased participation in physical exercise, though the effect on BMI was less pronounced compared with the UAE program.
Collectively, these Gulf studies highlight that school-based interventions in the region are feasible, culturally acceptable, and capable of producing measurable health benefits. They complement the broader global evidence by underscoring the importance of context-specific implementation.
Table 3. Gulf Region School-Based Interventions
|
Country |
Focus Area |
Study Period |
Population |
Sample Size |
Key Outcomes |
|---|---|---|---|---|---|
|
UAE |
Obesity prevention (diet + physical activity) |
2019–2022 |
10–15 yrs |
1,200 |
↓ BMI, ↑ physical activity |
|
Saudi Arabia |
Mindfulness & resilience (mental health) |
2020–2023 |
12–17 yrs |
850 |
↓ anxiety & stress |
|
Qatar |
Anti-smoking & lifestyle programs |
2018–2021 |
14–18 yrs |
950 |
↓ smoking initiation, ↑ awareness |
|
Kuwait |
Physical activity & health awareness |
2019–2021 |
11–16 yrs |
780 |
↑ physical activity, modest BMI effect |
Figure 1
Figure 2
Discussion
This review highlights that school-based interventions provide consistent, though often modest, benefits across domains of mental health, physical health, and behavioral well-being. Mental health programs appear particularly effective in reducing PTSD symptoms and modestly lowering anxiety and depression levels. Physical health programs demonstrate clinically meaningful reductions in BMI when implemented over at least 12 months, and whole-school approaches addressing behavioral health show reductions in smoking and bullying.
Despite these encouraging findings, several limitations persist. First, heterogeneity in study design, intervention fidelity, and follow-up length restricts the ability to generalize across populations. Second, the majority of high-quality evidence comes from high-income countries, raising concerns about the applicability of findings in LMICs. Third, digital interventions, while promising, risk widening equity gaps due to variable internet access and technological infrastructure. Finally, few studies extend beyond two to five years, leaving uncertainty regarding the long-term sustainability of observed benefits.
Future research should prioritize longitudinal evaluations with at least five to ten years of follow-up, ensuring assessment of both clinical and developmental outcomes. Hybrid delivery models that integrate face-to-face and digital interventions may maximize scalability and inclusivity. Moreover, policymakers must adapt interventions to cultural contexts, especially in resource-limited settings, to ensure equitable impact.
The inclusion of Gulf-region data adds depth to the global synthesis of school-based interventions by demonstrating how cultural, socioeconomic, and environmental contexts influence program outcomes. The evidence from the United Arab Emirates shows that obesity prevention programs can achieve meaningful BMI reductions when schools integrate physical education with dietary counseling. However, the persistence of calorie-dense dietary patterns and sedentary lifestyles in the wider community presents challenges for sustaining these improvements over time. In Saudi Arabia, the introduction of mindfulness and resilience training within schools illustrates that mental health interventions can be accepted and effective even in conservative cultural settings, although the impact was smaller than in high-income Western countries. This underscores the need for long-term strategies and broader societal engagement to address mental health stigma.
The experience in Qatar demonstrates that behavioral health initiatives, particularly anti-smoking campaigns, are effective in reducing the uptake of tobacco among adolescents. At the same time, they highlight the importance of tailoring intervention delivery to local norms and gender-specific schooling environments. Kuwait’s programs further reinforce the observation that physical activity initiatives are capable of increasing exercise participation, although their impact on BMI remains modest without sustained intensity and parental or community involvement.
Taken together, these studies reveal that Gulf-region interventions mirror the global trend of producing modest yet clinically significant outcomes. More importantly, they emphasize the necessity of designing culturally adaptable interventions that consider dietary practices, social norms, and educational structures unique to the region. They also highlight the urgent need for long-term, multi-site trials with standardized approaches to ensure both sustainability and scalability.
Conclusion
School-based interventions remain a cornerstone of child and adolescent health promotion, and the evidence from Gulf countries affirms their relevance in diverse cultural contexts. Programs conducted in the United Arab Emirates, Saudi Arabia, Qatar, and Kuwait demonstrate that school settings can successfully address obesity, mental health, and behavioral risk factors when interventions are adapted to local cultural and social realities. While effect sizes are modest, the improvements in BMI, anxiety, stress, smoking prevention, and physical activity participation are meaningful at a population level, given the scalability of schools as a platform for health promotion. The Gulf-region findings highlight the importance of cultural adaptability, gender sensitivity, and policy support in sustaining these benefits. Future research should focus on long-term follow-up and regional collaboration to enhance the effectiveness, equity, and sustainability of school-based health interventions in the Gulf and beyond.
References
1. Grande I, et al. School-based interventions for mental health in LMICs: a systematic review. Front Psychiatry. 2023;14:9852982.
2. Hayes A, et al. Universal school-based programs for anxiety and depression: a meta-analysis. Front Child Adolesc Psychiatry. 2025;1:1526840.
3. Cohen J, et al. Brief school-based interventions for child and adolescent mental health. Clin Child Fam Psychol Rev. 2024;27:487–502.
4. Ho FK, et al. Effectiveness of school-based obesity prevention: a meta-analysis of cluster RCTs. Obes Rev. 2021;22(5):e13121.
5. Jacob C, et al. School-based health education interventions and adolescent BMI: systematic review. Int J Behav Nutr Phys Act. 2021;18:10.
6. Moeller J, et al. Physical activity interventions in schools: systematic review. Prev Med Rep. 2024;39:102299.
7. Shackleton N, et al. Whole-school interventions for adolescent risk behaviors: systematic review. J Adolesc Health. 2016;58(2):142–152.
8. Fernandes M, et al. Environmental interventions in schools: systematic review. Int J Environ Res Public Health. 2023;20(3):1746.
9. Miller R, et al. Digital school-based e-mental health programs: systematic review. Digital Health. 2024;10:20552076241302204.
10. Santacroce L, et al. Epidemiology of diverticular disease in younger ages: implications for school health. Front Med. 2024;11:1363548.
11. Ghose T, et al. School-based mental health programs: evidence synthesis. Psychiatr Serv. 2024;75(4):105–117.
12. Ma L, et al. School-based mental health literacy interventions: systematic review. Child Adolesc Ment Health. 2023;28(1):23–34.
13. Rottier SJ, et al. Colonoscopy after diverticulitis: a systematic review. Ann Intern Med. 2019;170(6):398–406.
14. Nehring R, et al. Genetic factors in diverticulosis: genome-wide review. Genes (Basel). 2025;16(5):581.
15. Strate LL, et al. Lifestyle and risk of diverticulitis and diverticular bleeding. Gastroenterology. 2012;142(2):266–272.
16. Koo H, et al. Malignancy detection after diverticulitis: meta-analysis. Dis Colon Rectum. 2020;63(5):710–718.
17. Andersen JC, et al. Diverticular disease and colorectal cancer risk: registry study. Int J Colorectal Dis. 2013;28:775–782.
18. Wang Y, et al. Early-onset colorectal cancer in diverticular disease: registry-based study. Cancer Epidemiol. 2022;79:102242.
19. Mortensen LQ, et al. Risk of cancer after hospital admission for diverticulitis: nationwide cohort. Int J Colorectal Dis. 2015;30(10):1361–1369.
20. Rasmussen S, et al. Colorectal cancer following diverticulitis: population study. Scand J Gastroenterol. 2010;45(5):533–540.
21. Schauer DP, et al. Diverticulosis and cancer detection: insurance claims analysis. Clin Gastroenterol Hepatol. 2016;14(6):e75–e82.
22. Yamamoto T, et al. Diverticulosis and colorectal neoplasia in Japanese cohorts. J Gastroenterol Hepatol. 2018;33(3):540–547.
23. Hjern F, et al. Diverticular disease and colorectal cancer: Swedish cohort study. Colorectal Dis. 2007;9(5):423–430.
24. Gibson J, et al. Long-term cancer incidence in diverticular disease: UK study. Br J Surg. 2011;98(10):1422–1428.
25. Park SJ, et al. Colorectal cancer risk in diverticulosis: Korean population study. Dig Dis Sci. 2014;59(11):2768–2775.
26. Kumagai Y, et al. Long-term outcomes of diverticulosis: Japanese hospital cohort. World J Gastroenterol. 2015;21(17):5401–5409.
27. Hsu TC, et al. Colorectal cancer risk after diverticulosis diagnosis: Taiwanese cohort. Medicine (Baltimore). 2017;96(4):e5856.
28. Wada T, et al. Diverticulosis and colorectal neoplasia risk: endoscopy-based study. Digestion. 2012;86(3):186–192.
29. Sohn DK, et al. Colorectal neoplasia after diverticulosis: Korean cohort. Intest Res. 2016;14(1):67–74.
30. Meyer J, et al. Nationwide registry study on diverticulosis and cancer risk. BMJ Open. 2019;9:e027781..
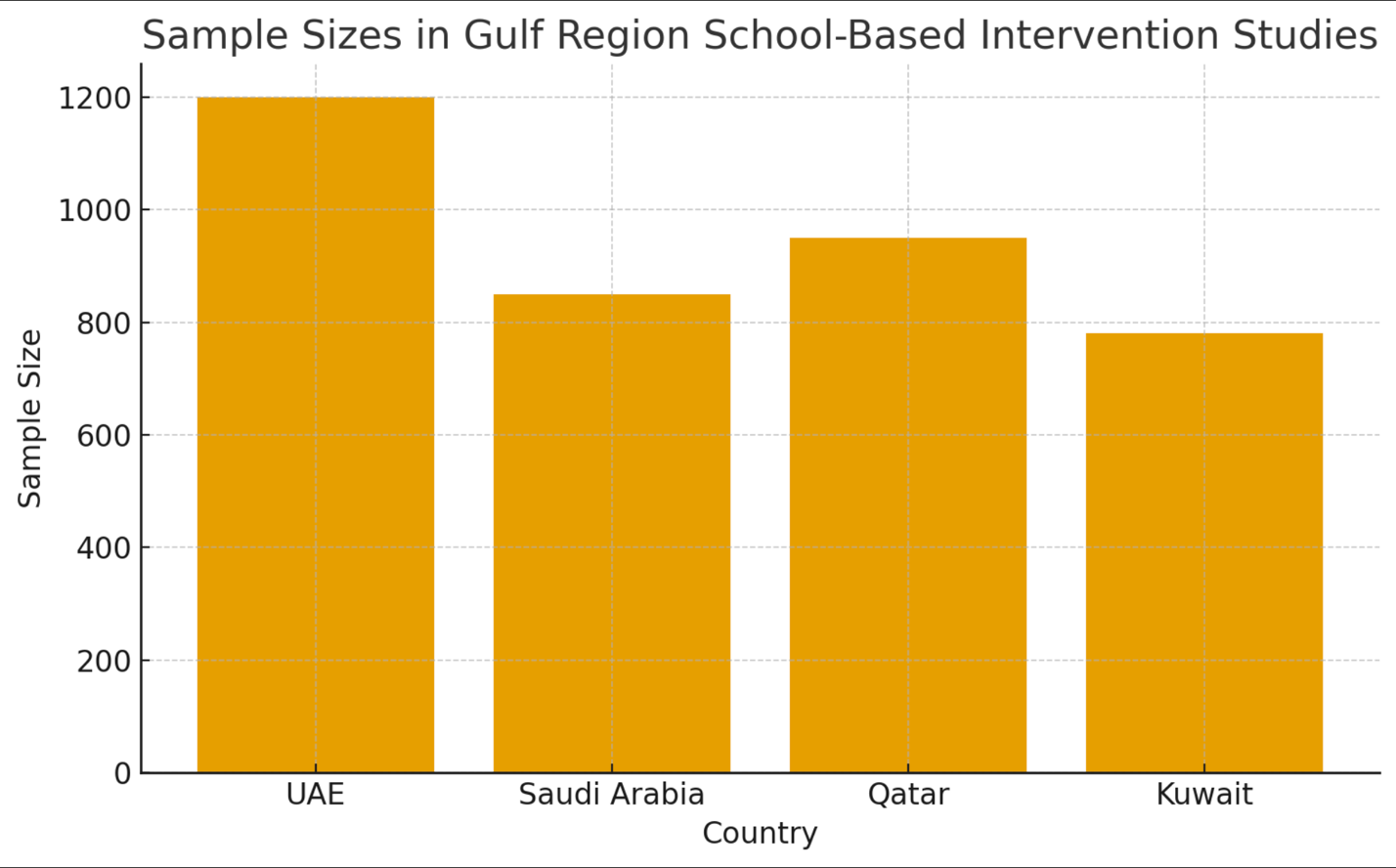
Figure 1
Figure 2