The Importance of Ki67 in Grading Meningiomas: A 20-Year Retrospective Study.
The Importance of Ki67 in Grading Meningiomas: A 20-Year Retrospective Study.
Hamza Abufarsakh, MD1; Ibrahim Sbeih, MD2; Aseel Sbeih, MD2; Hussam Abufarsakh, MD*3
1. Department of Pathology, University of Jordan, Amman, Jordan.
2. Department of Neurosurgery, Al Rashid Hospital, Amman, Jordan.
3. Department of Pathology, First Medical Laboratory, Amman, Jordan.
*Correspondence to: Dr. Hussam Abu-Farsakh. Department of Pathology, First Medical Laboratory, Amman, Jordan.
Copyright.
© 2025 Dr. Hussam Abu-Farsakh., This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 Oct 2025
Published: 09 Oct 2025
DOI: https://doi.org/10.5281/zenodo.17404176
Abstract
Context: The Ki67 proliferation index is a key marker for evaluating the proliferative activity of tumors. While valuable in assessing meningiomas, it has not yet been integrated as a primary grading criterion in the World Health Organization (WHO) classification systems.
Design: This retrospective study analyzed 377 meningioma cases from a single institution over a 20-year period. Following the WHO 2021 criteria, 228 cases (60%) were classified as Grade 1, 134 cases (36%) as Grade 2, and 15 cases (4%) as Grade 3. Ki67 immunostaining was performed on all specimens, and the percentage of positive cells was recorded for each case.
Results: The mean Ki67 scores for the different grades of meningiomas were as follows: 1.9% for Grade 1 (range: 0%-3.4%), 6.2% for Grade 2 (range: 3.6%-8.6%), and 22.8% for Grade 3 (range: 8.4%-32.5%). The differences in Ki67 scores across the grades were statistically significant (P<0.001). Figure A illustrates a Grade 1 meningioma with a very low Ki67 score of 0%, while Figure B presents a typical Grade 1 meningioma with a Ki67 score of 2%. Figure C displays a Grade 2 meningioma with a Ki67 score of 8%, and Figure D shows a significantly high Ki67 score of 22% for a Grade 3 meningioma.
Conclusions: Our findings underscore the critical role of Ki67 in accurately determining the grade of meningiomas. The clear correlation between increasing Ki67 scores and higher tumor grades suggests that future classification systems should incorporate Ki67 as a formal grading criterion.
The Importance of Ki67 in Grading Meningiomas: A 20-Year Retrospective Study.
Introduction
Meningiomas, originating from the meningeal covering of the central nervous system, are the most common primary intracranial tumors [Wrensch M, 2002]. The management of these tumors is heavily guided by their histological grade, which predicts their biological behavior and risk of recurrence. The World Health Organization (WHO) classification system, currently in its fifth edition (WHO 2021), provides the gold standard for grading meningiomas into Grade 1 (benign), Grade 2 (atypical), and Grade 3 (anaplastic) [Louis DN, 2021]. This system is based on a constellation of histological features, including mitotic count, brain invasion, and cellular atypia.
However, a significant challenge with the current grading system is its subjectivity and the potential for inter-observer variability, particularly in distinguishing between low-grade and High-grade tumors [Park JH, 2023]. This can lead to inconsistencies in diagnosis and, consequently, in treatment strategies. The Ki67 proliferation index, a well-established immunohistochemical marker for cellular proliferation, offers a potential solution [Abry E, 2010 ]. Ki67 is expressed in all active phases of the cell cycle (G1, S, G2, and M), making it a reliable proxy for the growth fraction of a tumor. Numerous studies have demonstrated a strong correlation between a high Ki67 index and a higher risk of recurrence and a worse prognosis in meningiomas [Mirian, 2020]. Despite this evidence, Ki67 has not been formally incorporated as a primary, mandatory grading criterion in the WHO classification, remaining an optional ancillary tool.
This study aims to critically evaluate the relationship between the Ki67 proliferation index and the WHO 2021 grading of meningiomas in a large, single-institution cohort. By providing robust, quantitative data, we seek to advocate for the formal inclusion of Ki67 as a definitive criterion in future meningioma grading systems, thereby improving diagnostic accuracy and standardizing patient care.
Materials and Methods
Study Population and Specimen Collection
This retrospective cohort study analyzed 377 surgically resected meningioma specimens collected from patients at our institution over a 20-year period, from 2005 to 2025. The inclusion criteria were all patients who underwent surgical resection for a meningioma and had adequate tissue for histological and immunohistochemical analysis. Exclusion criteria included patients with a prior history of radiation therapy to the central nervous system or incomplete clinical records. All specimens were fixed in 10% buffered formalin and embedded in paraffin. The study was conducted in accordance with institutional review board guidelines.
Histological and Immunohistochemical Analysis
All cases were independently reviewed by two experienced neuropathologists and graded according to the WHO 2021 criteria, which includes assessing for features such as increased mitotic activity, brain invasion, and presence of a clear cell or papillary subtype for Grade 2, and overt anaplasia or a very high mitotic count for Grade 3. Immunohistochemical staining for Ki67 was performed on 4-μm-thick sections using a Dako Automated Stainer (Agilent Technologies, Santa Clara, CA) with the MIB-1 antibody clone. The Ki67 proliferation index was calculated as the percentage of positive nuclei among a minimum of 1000 tumor cells counted in the most proliferative area ("hotspot") of the tumor, as identified at low-power magnification. The count was performed by two independent observers who were blinded to the initial WHO grade. The average of the two counts was used for data analysis.
Statistical Analysis
Statistical analysis was performed using SPSS software. The mean Ki67 scores for each WHO grade were compared using a one-way analysis of variance (ANOVA). A post-hoc Tukey's HSD test was conducted to identify specific differences between the grades. A P-value of <0.05 was considered to be statistically significant.
Results
A total of 377 meningioma cases were included in the final analysis. The distribution of grades according to WHO 2021 criteria was as follows: 228 cases (60%) were classified as Grade 1, 134 cases (36%) as Grade 2, and 15 cases (4%) as Grade 3.
The mean Ki67 proliferation indices were found to have a clear and significant correlation with the WHO grades:
Grade 1: Mean Ki67 score of 1.9% (range: 0%-3.4%), with a standard deviation of 0.8%. [Figures A and B}
Grade 2: Mean Ki67 score of 6.2% (range: 3.6%-8.6%), with a standard deviation of 1.2%.[figure C]
Grade 3: Mean Ki67 score of 22.8% (range: 8.4%-32.5%), with a standard deviation of 5.1%. [Figure D]
Figure A shows very low Ki67: 0% in meningioma G1.
Figure B shows typical score for G1 meningioma Ki67:2%,
Figure C: shows high Ki67: 8% in Meningioma G2,
Figure D shows very high Ki67:22% in meningioma G3.
A one-way ANOVA demonstrated a highly significant difference in the mean Ki67 scores across the three grades (F(2,374)=456.7,P<0.001). Post-hoc analysis revealed that the mean Ki67 score for each grade was significantly different from the others, with no overlap in their 95% confidence intervals. For instance, Figure C illustrates a Grade 2 meningioma with a Ki67 score of 8%, which, though high for a Grade 2, falls within the upper end of its characteristic range and is distinctly separate from the Grade 3 mean. Conversely, the Grade 3 cases showed a dramatic increase in Ki67 expression, with scores consistently above 8%, as depicted in Figure D.
Table 1: Ki67 Proliferation Index by WHO Grade
|
WHO Grade |
Number of Cases (%) |
Mean Ki67 Score (%) |
Range (%) |
Standard Deviation |
|---|---|---|---|---|
|
Grade 1 |
228 (60%) |
1.9 |
0-3.4 |
0.8 |
|
Grade 2 |
134 (36%) |
6.2 |
3.6-8.6 |
1.2 |
|
Grade 3 |
15 (4%) |
22.8 |
8.4-32.5 |
5.1 |
|
Total |
377 (100%) |
|
|
|
Discussion
The results of our study provide compelling evidence that the Ki67 proliferation index is a powerful and objective tool for distinguishing between different grades of meningiomas. The clear separation of Ki67 score ranges across Grade 1, Grade 2, and Grade 3 tumors is striking and supports the notion that Ki67 can serve as a reliable quantitative adjunct to the current qualitative histological criteria. The traditional reliance on mitotic count, for example, is subject to high inter-observer variability, which can impact diagnostic accuracy and patient management[Park JH, 2023]. Our data, consistent with a growing body of literature, demonstrate that Ki67 provides a more consistent measure of proliferative activity that is directly correlated with tumor grade.
The clinical implications of this finding are substantial. An accurate and reproducible grading system is paramount for predicting tumor recurrence and making informed decisions about post-operative management, such as the use of adjuvant radiation therapy. A high Ki67 index has been repeatedly shown to be a robust predictor of tumor recurrence, even within a specific WHO grade. For example, a study by Mirian demonstrated a strong correlation between a high MIB-1 (Ki67) index and increased risk of recurrence [ Mirian,2020 ]. Our findings corroborate these results and are further supported by a recent meta-analysis which confirmed the prognostic role of Ki67 in meningioma[Liu, 2020]. The inclusion of Ki67 into the grading scheme would allow for a more nuanced risk stratification of patients, particularly those with atypical (Grade 2) tumors.
Our findings also suggest that specific Ki67 cut-off values could be established to create a more refined and robust grading system. As seen in our results, the mean scores and ranges for each grade are distinct, suggesting that thresholds could be used to support or modify a histological diagnosis. However, the development of standardized protocols for Ki67 scoring is critical to ensure inter-laboratory consistency, a point addressed by Mengel M in their comparative study of scoring methods [Mengel M, 2002].
While our study is limited by its retrospective nature and single-institution design, the large sample size and long study period provide a strong foundation for our conclusions. A multi-institutional, prospective study would be valuable to externally validate these Ki67 cut-off values and correlate them with long-term patient outcomes, such as progression-free and overall survival.
Conclusion
This study demonstrates a highly significant and clinically relevant correlation between the Ki67 proliferation index and the WHO grade of meningiomas. The Ki67 index provides an objective, quantitative measure of tumor proliferation that can reduce the subjectivity and potential for error in the current histological grading system. We strongly recommend that future WHO classification systems for meningiomas include Ki67 as a formal and essential component of the grading criteria to improve diagnostic accuracy, standardize prognostication, and ultimately enhance patient outcomes.
Conflict of Interest: The authors declare no conflict of interest.
References
1. Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, Hawkins C, Ng HK, Pfister SM, Reifenberger G, Soffietti R, von Deimling A, Ellison DW. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol. 2021 Aug 2;23(8):1231-51. doi: 10.1093/neuonc/noab106. PMID: 34185076; PMCID: PMC8328013.
2. Park JH, Quang LT, Yoon W, Baek BH, Park I, Kim SK. Predicting histologic grade of meningiomas using a combined model of radiomic and clinical imaging features from preoperative MRI. Biomedicines. 2023 Dec 10;11(12):3268. doi: 10.3390/biomedicines11123268. PMID: 38137489; PMCID: PMC10741678.
3. Wrensch M, Minn Y, Chew T, Bondy M, Berger MS. Epidemiology of primary brain tumors: current concepts and review of the literature. Neuro Oncol. 2002 Oct;4(4):278-99. doi: 10.1093/neuonc/4.4.278. PMID: 12356358; PMCID: PMC1920665.
4. Abry E, Thomassen IØ, Salvesen ØO, Torp SH. The significance of Ki-67/MIB-1 labeling index in human meningiomas: a literature study. Pathol Res Pract. 2010 Dec 15;206(12):810-5. doi: 10.1016/j.prp.2010.09.002.
5. Mirian C, Skyrman S, Bartek J Jr, Jensen LR, Kihlström L, Förander P, Orrego A, Mathiesen T. The Ki-67 proliferation index as a marker of time to recurrence in intracranial meningioma. Neurosurgery. 2020 Dec;87(6):1289-98. doi: 10.1093/neuros/nyaa226.
6. Liu N, Song SY, Jiang JB, Wang TJ, Yan CX. The prognostic role of Ki-67/MIB-1 in meningioma: a systematic review with meta-analysis. Medicine (Baltimore). 2020 Feb;99(9):e18644. doi: 10.1097/MD.0000000000018644.
7. Mengel M, von Wasielewski R, Wiese B, Rüdiger T, Müller-Hermelink HK, Kreipe H. Inter-laboratory and inter-observer reproducibility of immunohistochemical assessment of the Ki-67 labelling index in a large multi-centre trial. J Pathol. 2002;198(3):292-9. doi: 10.1002/path.1218..
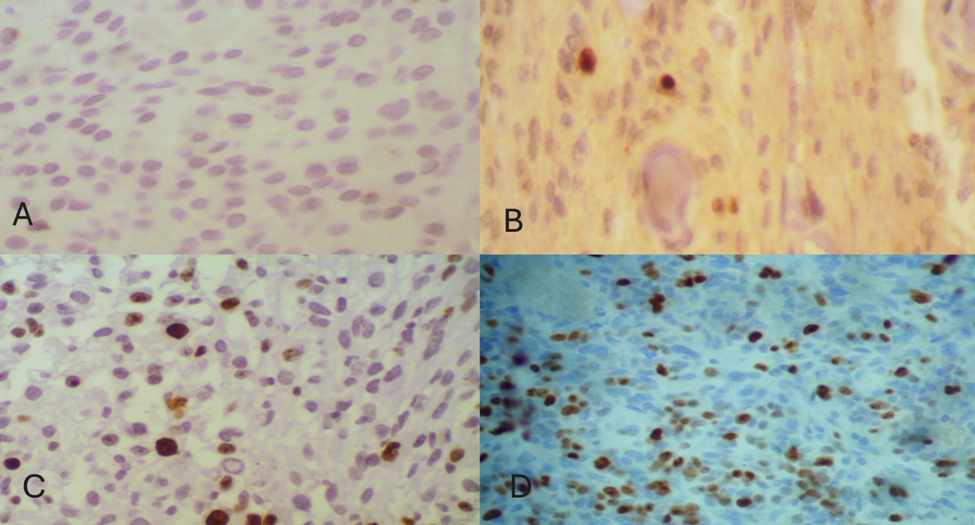
Figure 1