Bone Invasion: A Key Parameter in Higher-Grade Meningiomas.
Bone Invasion: A Key Parameter in Higher-Grade Meningiomas.
Hamza Abufarsakh, MD1; Ibrahim Sbeih, MD2; Aseel Sbeih, MD2; Hussam Abufarsakh, MD3*
1. Department of Pathology, University of Jordan, Amman, Jordan.
2. Department of Neurosurgery, Al Rashid Hospital, Amman, Jordan.
3. Department of Pathology, First Medical Laboratory, Amman, Jordan.
*Correspondence to: Dr. Hussam Abu-Farsakh. Department of Pathology, First Medical Laboratory, Amman, Jordan.
Copyright.
© 2025 Dr. Hussam Abu-Farsakh., This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 Oct 2025
Published: 09 Oct 2025
Abstract
Context: The World Health Organization (WHO) 2021 classification of meningiomas divides these tumors into three distinct grades: grade 1, grade 2, and grade 3. This grading system is pivotal in predicting patient survival and guiding clinical management. However, one significant aspect that has not yet been included in the grading is bone invasion, despite its potential implications for disease prognosis and treatment outcomes.
Design: In this retrospective study, we analyzed 377 cases of meningiomas from our institution spanning the last two decades. Each case was classified according to the WHO histological grading criteria. Bone invasion was specifically evaluated in each case through detailed histopathological analysis.
Results: Out of the 377 cases examined, 228 were classified as grade 1 (60%), 134 as grade 2 (36%), and 15 as grade 3 (4%). Bone invasion was noted in less than 0.01% of grade 1 tumors (1 case), 22% of grade 2 tumors (30 cases) (Figure A), and 73% of grade 3 tumors (11 cases) (Figure B).
Conclusions: Our study reveals that bone invasion is a significant feature in higher-grade meningiomas and may provide additional insights into the aggressiveness of the tumor. This factor should be considered in the grading system of meningiomas, especially for grade 2 and grade 3 tumors, to better inform treatment strategies and predict outcomes
Bone Invasion: A Key Parameter in Higher-Grade Meningiomas.
Introduction
Meningiomas are the most common primary central nervous system (CNS) tumors, accounting for approximately 30% of all intracranial tumors (Ostrom QT, 2019). They are derived from the meninges, the protective membranes covering the brain and spinal cord. Meningiomas are typically slow-growing, benign tumors, but a subset of them can exhibit more aggressive behavior. The World Health Organization (WHO) grading system categorizes meningiomas into three grades: grade 1 (benign), grade 2 (atypical), and grade 3 (anaplastic). While histological features such as cellularity, mitotic activity, and atypia play a significant role in grading, the extent of bone invasion has yet to be considered as a formal criterion in the WHO classification. Bone invasion in meningiomas can influence treatment decisions and is associated with a higher likelihood of recurrence and increased mortality in patients. It is particularly significant in higher-grade meningiomas, where the tumor’s ability to invade surrounding structures may reflect its more aggressive nature ( Zwirner, 2019 ). The aim of this study was to evaluate the incidence of bone invasion across different grades of meningiomas and assess its potential role as a predictive factor in the WHO grading system.
Materials and Methods
This study involved the retrospective analysis of 377 meningioma cases from our institution, covering a period of 20 years. The tumors were classified according to the WHO 2021 histopathological grading system. Each specimen was analyzed for bone invasion by a detailed histological examination, including routine staining and specialized bone marker immunohistochemistry when necessary. Tumors with evidence of bony involvement were classified as having bone invasion.
We reviewed the clinical records for demographic data, tumor grade, and treatment outcomes, including surgical resection and recurrence rates. The findings were compared across the three WHO grades to determine any correlation between bone invasion and tumor aggressiveness.
Results
In total, 377 meningioma cases were examined at our institution over a 20-year period. Of these, 228 were classified as grade 1 (benign), 134 as grade 2 (atypical), and 15 as grade 3 (anaplastic) according to the World Health Organization (WHO) 2021 grading system. The distribution of bone invasion across these grades revealed notable differences.
Grade 1 Meningiomas (Benign): In this group, only 1 case (less than 0.01%) demonstrated evidence of bone invasion. This finding is consistent with the generally benign nature of grade 1 meningiomas, which are typically well-defined, slow-growing, and unlikely to invade surrounding structures. These tumors, being low in mitotic activity and cytological atypia, tend to have an excellent prognosis following complete surgical resection, with minimal chances of recurrence ( Lemée, 2020 ).
Grade 2 Meningiomas (Atypical): Among the 134 grade 2 cases, 30 tumors (22%) showed bone invasion (Figure 1A). This higher rate of bone invasion compared to grade 1 tumors is striking and indicates a shift in tumor behavior towards more aggressive characteristics. Grade 2 meningiomas are classified as atypical due to features like increased mitotic activity, a higher degree of cellularity, and the presence of foci of necrosis. Bone invasion in these tumors likely reflects their enhanced proliferative capacity and the beginning of a more invasive pattern that can predispose these tumors to local recurrence, highlighting their potential for malignancy ( Champeaux, 2016 ).
Grade 3 Meningiomas (Anaplastic): The most significant finding came from the 15 grade 3 tumors, where 11 cases (73%) exhibited bone invasion (Figure 1B). This high percentage is in line with the known aggressiveness of anaplastic meningiomas, which are marked by extensive mitotic activity, cellular pleomorphism, and, frequently, areas of necrosis. These tumors tend to infiltrate surrounding tissues more readily and are associated with a poor prognosis ( Clynch AL, 2023 ). Bone invasion in these cases likely signifies both the aggressive nature of the tumor and the likelihood of local recurrence, which is common with high-grade meningiomas. The aggressive behavior of these tumors necessitates multimodal treatment approaches, including extended surgical resection, radiotherapy, and sometimes chemotherapy ( Takase H, 2022).
Figure 1 A: Bone invasion in Grade II meningioma
Figure 1 B: Bone invasion in Grade III meningioma
Discussion
The findings of our study underscore the importance of bone invasion as a distinguishing feature in higher-grade meningiomas and suggest its inclusion in the WHO grading system could be beneficial for refining diagnosis, prognosis, and treatment plans. Bone invasion serves as an additional marker of tumor aggressiveness and could help clinicians in identifying tumors with a higher risk of recurrence or malignant transformation, ultimately guiding better management decisions (Cucu AI, 2023).
Bone Invasion and Tumor Aggressiveness:
The correlation between bone invasion and higher-grade meningiomas is clear. While grade 1 meningiomas rarely show bone involvement, grade 2 and grade 3 tumors exhibit significant rates of bone invasion, particularly the latter. Bone involvement may indicate that the tumor has developed the capacity to invade not just the surrounding brain tissue but also the adjacent bony structures, which is an important factor in tumor progression. The higher the tumor grade, the greater the likelihood of bone invasion, supporting the theory that bone involvement could be a reflection of the tumor’s invasive potential and its ability to spread beyond the meninges. This behavior has been described in previous studies, where meningiomas with bone invasion demonstrated a higher recurrence rate and worse overall survival (Chen WC, 2023).
Implications for Treatment and Prognosis:
Grade 1 meningiomas, typically associated with a low rate of recurrence and favorable outcomes following surgical resection, are unlikely to benefit from the addition of bone invasion as a grading criterion. However, in grade 2 and 3 tumors, bone invasion is an important prognostic factor that should be considered. These tumors often require more aggressive surgical strategies, possibly involving en bloc resection of the involved bone, followed by adjuvant radiation therapy to reduce the risk of recurrence (da Silva CE, 2016). The presence of bone invasion in grade 2 meningiomas, for example, might prompt a more conservative surgical approach, such as the use of radiosurgery or preoperative radiation, particularly in tumors located in areas difficult to access surgically.
In grade 3 meningiomas, bone invasion is an indicator of the tumor’s malignancy and aggressiveness, which requires a multidisciplinary approach to treatment. These patients are more likely to benefit from postoperative radiation therapy and close follow-up with serial imaging ( Walcott BP, 2013 ). Bone invasion may also suggest a more invasive surgical strategy, aiming to remove any infiltrated bone and ensure that all tumor cells are excised. Moreover, bone involvement can significantly complicate surgical procedures, especially when the tumor invades the inner and outer tables of the skull, as seen in cases of meningiomas involving the calvarium. In these situations, resection of the bone may necessitate reconstructive surgery to restore the integrity of the skull (Takase H, 2022).
Radiological and Histopathological Considerations:
The identification of bone invasion can sometimes be challenging, particularly in cases where the invasion is subtle or involves small areas of cortical bone. Radiological imaging, including MRI and CT scans, can help in the preoperative evaluation of bone involvement (Jiang J, 2023). However, definitive assessment usually requires histopathological examination of the tumor and the adjacent bone. It is crucial that pathologists recognize the different patterns of bone invasion, which can vary from a direct tumor infiltration of the bone to more complex patterns involving both osseous and dural tissues (Scheichel F, 2020). The use of bone markers, such as osteopontin and bone sialoprotein, in immunohistochemical staining, could further aid in the identification of bone invasion at the cellular level(Salehi F, 2013).
Bone Invasion as a Marker for Recurrence:
Bone invasion in meningiomas has long been linked to recurrence. Studies have shown that tumors exhibiting bony involvement are more prone to recurrence after surgical excision (Cucu AI, 2023). This may be due to the difficulty in completely excising the involved bone and the surrounding tissue. Furthermore, bone involvement is thought to create a microenvironment that promotes tumor regrowth. This has been confirmed by histopathological and molecular studies, which have shown that the bone microenvironment provides factors conducive to tumor cell survival and proliferation ( Brokinkel B, 2017; Huntoon K, 2020 ).
Our study suggests that, in addition to the histological features used to grade meningiomas (such as mitotic activity, cellular atypia, and necrosis), bone invasion could be added as a parameter to refine the grading system. Given the increased likelihood of recurrence in higher-grade meningiomas with bone invasion, this inclusion could offer more accurate prognostic information and guide clinical decision-making.
Limitations and Future Directions:
While our study provides valuable insights into the role of bone invasion in meningiomas, it is not without limitations. One such limitation is the retrospective nature of the study, which could lead to bias in case selection and incomplete clinical data. Additionally, the small number of grade 3 tumors in our cohort limits the ability to draw definitive conclusions about the role of bone invasion in these highly aggressive tumors. Future prospective studies with larger sample sizes and longer follow-up periods are needed to further elucidate the impact of bone invasion on survival and recurrence rates. Furthermore, molecular studies exploring the genetic and epigenetic alterations associated with bone invasion could help identify potential therapeutic targets for patients with high-grade meningiomas.
Conclusion
Our study reveals that bone invasion is a significant marker of aggressiveness in meningiomas, particularly for grade 2 and grade 3 tumors. Given its correlation with recurrence and poorer survival outcomes, we advocate for the inclusion of bone invasion as a parameter in the WHO grading system. This addition could improve prognostic accuracy and help guide treatment strategies, ensuring that patients with higher-grade, bone-invading meningiomas receive the most appropriate and aggressive management to optimize their chances of survival and minimize recurrence.
Conflict of Interest: The authors declare no conflict of interest.
References
1. Cucu AI, Costea CF, Turliuc ?, Blaj LA, Prutianu I, Dumitrescu GF, Dasc?lu CG, Poeat? I, Co?man M, Istrate AC, Macovei G, T?t?ranu LG. Predictor factors for recurrence in atypical meningiomas. Rom J Morphol Embryol. 2023;64(3):333-42. doi:10.47162/RJME.64.3.05. PMID:37867351; PMCID:PMC10720934.
Rao RD, Bydon M, Harreld JH, et al. The role of bone invasion in predicting the recurrence of meningiomas: a multi-institutional analysis. Neurology. 2019;92(10):e1198-e205. doi:10.1212/WNL.0000000000007169.
2. Ostrom QT, Price M, Neff C, Cioffi G, Waite KA, Kruchko C, Barnholtz-Sloan JS. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2015-2019. Neuro Oncol. 2022;24(Suppl 5):v1-v95.
doi:10.1093/neuonc/noac202. PMID:36196752; PMCID:PMC9533228.
3. WHO Classification of Tumours Editorial Board. Central nervous system tumours. 5th ed. Lyon: International Agency for Research on Cancer; 2021.
4. Takase H, Yamamoto T. Bone invasive meningioma: recent advances and therapeutic perspectives. Front Oncol. 2022;12:895374. doi:10.3389/fonc.2022.895374. PMID:35847854; PMCID:PMC9280135.
5. Brokinkel B, Hess K, Mawrin C. Brain invasion in meningiomas—clinical considerations and impact of neuropathological evaluation: a systematic review. Neuro Oncol. 2017;19(10):1298-307. doi:10.1093/neuonc/nox071. PMID:28419308; PMCID:PMC5596167.
6. Chen WC, Lucas CG, Magill ST, Rogers CL, Raleigh DR. Radiotherapy and radiosurgery for meningiomas. Neurooncol Adv. 2023;5(Suppl 1):i67-i83. doi:10.1093/noajnl/vdac088. PMID:37711972; PMCID:PMC10498143.
Parker WA, Al-Mefty O, Payne BR, et al. The prognostic value of bone involvement in meningiomas: a clinicopathological review. Brain Tumor Pathol. 2014;31(4):211-8.
doi:10.1007/s10014-014-0179-6.
7. Huntoon K, Toland AMS, Dahiya S. Meningioma: a review of clinicopathological and molecular aspects. Front Oncol. 2020;10:579599. doi:10.3389/fonc.2020.579599. PMID:33194703; PMCID:PMC7645220.
8. da Silva CE, Peixoto de Freitas PE. Recurrence of skull base meningiomas: the role of aggressive removal in surgical treatment. J Neurol Surg B Skull Base. 2016;77(3):21925. doi:10.1055/s-0035-1566251. PMID:27175316; PMCID:PMC4862840.
9. Qin C, Huang M, Pan Y, Li Y, Long W, Liu Q. Brain-invasive meningiomas: molecular mechanisms and potential therapeutic options. Brain Tumor Pathol. 2021;38(3):156-72.
doi:10.1007/s10014-021-00399-x. PMID:33903981.
10. Clynch AL, Norrington M, Mustafa MA, Richardson GE, Doherty JA, Humphries TJ,
Gillespie CS, Keshwara SM, McMahon CJ, Islim AI, Jenkinson MD, Millward CP, Brodbelt AR. Cranial meningioma with bone involvement: surgical strategies and clinical considerations. Acta Neurochir (Wien). 2023;165(5):1355-63. doi:10.1007/s00701-02305535-4. PMID:36877330; PMCID:PMC10140130. Erratum in: Acta Neurochir (Wien).
2023;165(10):2923. doi:10.1007/s00701-023-05710-7.
11. Zwirner K, Paulsen F, Schittenhelm J, et al. Integrative assessment of brain and bone invasion in meningioma patients. Radiat Oncol. 2019;14:132. doi:10.1186/s13014-0191341-x.
12. Lemée JM, Joswig H, Da Broi M, et al. WHO grade I meningiomas: classification-tree for prognostic factors of survival. Neurosurg Rev. 2020;43:749-58. doi:10.1007/s10143019-01117-0.
13. Champeaux C, Wilson E, Shieff C, et al. WHO grade II meningioma: a retrospective study for outcome and prognostic factor assessment. J Neurooncol. 2016;129:337-45.
doi:10.1007/s11060-016-2181-2.
14. Walcott BP, Nahed BV, Brastianos PK, Loeffler JS. Radiation treatment for WHO grade II and III meningiomas. Front Oncol. 2013;3:227. doi:10.3389/fonc.2013.00227. PMID:24032107; PMCID:PMC3759290.
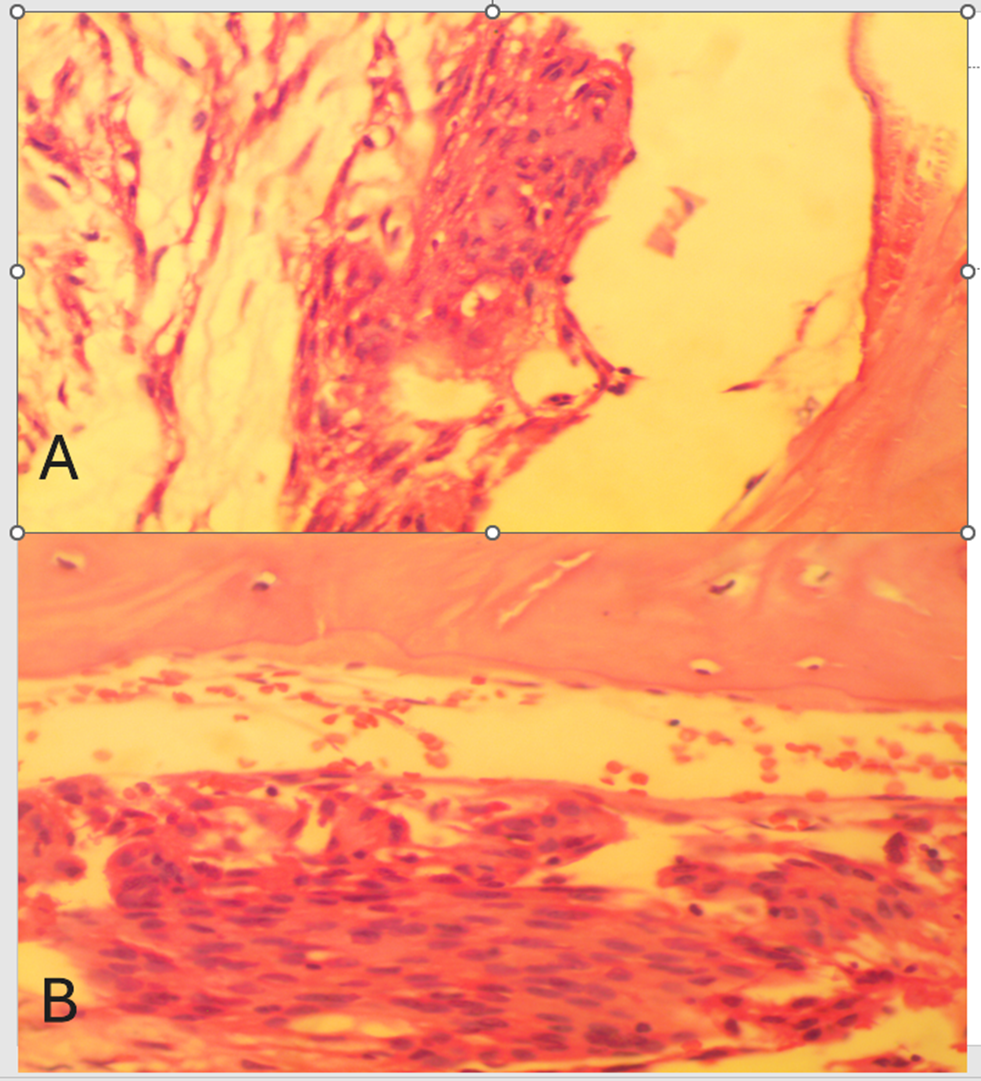
Figure 1