Appendicular Mucocele Complicated by Pseudomyxoma Peritonei
Sidi Ely Mokhtar1, F.Zahra Cheikhna2*, Md Dede Alioune3, Mkhaitratt Yahya4
1,2,3,4. Radiology Department, Gastroenterology Department, Surgery Department, Nouakchott Military Hospital, Mauritania.
*Correspondence to: F.Zahra Cheikhna, Nouakchott Military Hospital, Mauritania.
Copyright.
© 2025 F.Zahra Cheikhna This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 Oct 2025
Published: 15 Oct 2025
ABSTRACT
Appendiceal mucocele is a rare condition, defined as a cystic dilation of the lumen of the appendix due to an accumulation of intraluminal mucinous secretions, which are translucent and gelatinous, and may affect either the entire organ or a segment, most often distal. Appendiceal pseudomyxoma, or gelatinous peritoneal disease, is the most dreaded complication of appendiceal mucocele; it is a rare disease characterized by the presence of abundant gelatinous material in the abdomen secondary to the rupture of a mucinous appendix lesion.
Our case involves a 47-year-old woman who presents with peritoneal pseudomyxoma, detected early in relation to a ruptured appendiceal pseudomyxoma localized in the peri-appendiceal region.
Keyword: Appendiceal mucocele, peritoneal pseudomyxoma, surgery, appendiceal mucinous neoplasm.
Appendicular Mucocele Complicated by Pseudomyxoma Peritonei
Observation
A 47-year-old patient with no particular medical history presented with hypogastric abdominal pain and fever of 40 degrees Celsius (104.4 Fahrenheit) for the past 48 hours. Physical examination noted guarding in the right iliac fossa and hypogastric region. Blood count: White blood cell count at 17,000 cells/mm3, predominantly polymorphonuclear neutrophils. Abdominal CT: Tubular formation at the level of the IDF measuring 34 mm in maximum thickness, with fluid content and a calcified wall enhanced after injection of contrast agent with a fluid collection around it.
She underwent surgery by midline laparotomy objectifying a ruptured swollen appendix with gelatinous fluid emerging from the rupture located periappendicular. The surgical procedure consisted of an appendectomy since the base was macroscopically healthy with abdominal cleansing and drainage of the culs of the Douglas sac.
The patient was placed on dual antibiotic therapy + analgesic and anticoagulant. The postoperative course was unremarkable with resumption of bowel movements on postoperative day 2. The patient was declared discharged on the fourth day of hospitalization. Anatomopathological study: Morphological appearance in favor of acute suppurative appendicitis on a low-grade appendicular mucinous neoplasm; fissured with peritoneal reaction and presence of mucin on the appendicular serosa; healthy appendicular margin.
Discussion
Appendiceal mucocele (AM) was first described by Rokitansky in 1842. [1]
Appendiceal mucocele is a rare condition, defined as a cystic dilation of the appendiceal lumen following an intraluminal accumulation of translucent, gelatinous mucinous secretions, which can affect either the entire organ or a segment, most often distal. It is a pathology discovered postoperatively histologically in nearly 70% of cases; Two converging theories have been put forward to explain this disease: the obstructive theory: AMs are due to an accumulation of mucus upstream of a stenosis of the appendiceal lumen (cecal adenocarcinoma, appendiceal tumor, tuberculosis). The neoplastic theory: the tumor is responsible for hypersecretion of mucus into the appendiceal lumen. [2,3,4, 5]
Appendiceal mucoceles have a highly varied and nonspecific clinical presentation. They may be asymptomatic and discovered incidentally during imaging (CT, ultrasound, etc.), colonoscopy, or even intraoperatively or postoperatively through pathological examination of resection specimens. [4, 6]
The most frequently encountered symptoms are right iliac fossa pain (present in 27 to 64% of cases of appendectomy and in 40 to 77% of cases of cystadenocarcinoma), an abdominal mass (9 to 46% of cases), an AOI, and an enlarged umbilical or inguinal hernia. Most often, the symptomatology is dominated by right iliac fossa pain; mucoceles are found in 0.2 to 0.3% of appendectomies. [5, 6]
The most serious complication is peritoneal rupture in 5-15% of cases: pseudomyxoma peritonei [5, 6]
Paraclinical investigations can be of great value for diagnosis [3, 4, 6]. Indeed, annular or arcuate calcifications with a porcelain appendix can sometimes be present on a plain abdominal X-ray.
Imaging based on a combination of ultrasound and CT is a crucial examination for preoperative diagnosis. On ultrasound, MA presents as an elliptical cystic mass, well-limited by the wall which may be partially calcified, with echogenic and stratified content, producing an “onion bulb” appearance. The differential diagnosis is generally with acute appendicitis. A transverse diameter greater than or equal to 15 mm is associated with a sensitivity of 83% and a specificity of 92% for the diagnosis of MA. In the case of simple acute appendicitis, the transverse diameter is greater than 6 mm [4].
On computed tomography (CT), uncomplicated AD appears as a cystic mass of the IDF, well-demarcated by fluid density. Arcuate parietal calcifications are inconsistent, but their presence supports the diagnosis of AD, differentiating it from an abscessed collection of the IDF [5]. The benign or malignant nature of AD is confirmed by pathological examination. On MRI, the contents of the AD appear as T1-weighted hypointense and T2-weighted hyperintense. Calci?cations are less well visualized than on CT.
Complications include acute intestinal intussusception, torsion, or extrinsic compression on a neighboring organ. But the most feared complication is intraperitoneal rupture, spontaneous or during a surgical procedure, responsible for pseudomyxoma peritonei (PMP). PMP is defined by dissemination in the abdominal cavity of the mucous contents of the MA; it is therefore a thick ascites like jelly. It was long thought that ovarian origin was a cause of PMP due to the clear female predominance and the frequent involvement of the ovaries, but more recent studies have contradicted this hypothesis based on immunohistochemical and molecular biology analyses demonstrating the appendicular origin of almost all PMPs. Ovarian involvement is therefore secondary [6]. Abdominal CT is the examination of choice to diagnose PMP and specify its characteristics; the typical appearance of PMP is "scalloping" on the surface of solid organs, particularly the liver and spleen. This sign is explained by the extrinsic compression of gelatinous masses on solid organs. On CT, this ascites appears hypodense (denser than serous ascites), and sometimes it can contain fine septa and curvilinear calcifications. [7,8,9].
Treatment consists of appendectomy in the absence of histological signs of malignancy and in the presence of retentional MA. In the presence of a cystadenoma, cecal resection is sometimes necessary for complete excision of the lesion. In the case of a malignant lesion, hemicolectomy is considered the treatment of choice and is required immediately in the case of frozen section examination or secondarily after a definitive histological diagnosis, hence the importance of systematically performing an anatomopathological examination of any appendectomy specimen. The laparoscopic approach should be avoided given the risks of recurrence and intraoperative dissemination. [10,11].
Conclusion
Mucus-secreting tumors of the appendix are rare. They should be considered in cases of atypical appendiceal syndrome or a right iliac fossa mass. Early diagnosis of unruptured AM by a radiologist improves the prognosis of the disease and thus avoids any form of repeat interventions.
Conflicts of Interest
The authors declare no conflicts of interest.
Author Contributions
All authors contributed to this work.
References
[1] M. Outznit, H. Bellamlih, Y. Omor, R. Latib Appendicular mucocele complicated with pseudomyxoma peritonei
[2] Haritopoulos KN, Brown DC, Lewis P, Mansour F, Eltayar AR, Labruzzo C, et al.
Appendiceal mucocele: a case report and review of the literature. Int Surg. 2001 Oct-Dec;86(4):259–62. [PubMed] [Google Scholar]
[3] Scotté M, Laquerriére A, Riff Y, Majerus B, Manouvrier B, Leblanc JL, et al. Appendiceal mucoceles: pathophysiology and therapeutic implications. J Chir (Paris). 1994 Jun-Jul;131(6-7):303–12. [PubMed] [Google Scholar]
[4]Etienne JC, Oberlin P, Bergue A, Felsenheld C, Hillion Y, Fignerhut A. Mucosecretory tumors of the appendix. Six observations. Ann Chir. 1991;45(7):577–583. [PubMed] [Google Scholar]
[5]Shukunami K, Kaneshima M, Kotsuji F. Preoperative diagnosis and radiographic findings of a freely movable mucocele of the vermiform appendix. Can Assoc Radiol J. 2000 Oct;51(5):281–2. [PubMed] [Google Scholar]
[6] P,Sharma et al. Dilated appendix: is there more to it? Case report and brief review of literature with radiologic-pathological correlation J Clin Imaging Sci(2019)
[7] Soweid AM, Clarkston WK, Andrus CH, Janney CG. Diagnosis and management of appendix mucoceles. Dig Dis. 1998 May-Jun;16(3):183– doi: 10.1159/000016863. [DOI] [PubMed] [Google Scholar]
[8] Sharma P, Soin P, Chugh M, Goyal P. Dilated appendix: is there more to it? Case report and brief review of literature with radio-logic-pathological correlation. J Clin Imaging Sci 2019;9:9.
[9] Aggarwal N, Bhargava A. Appendiceal mucocele secondary totortion in an asymptomatic patient. J Surg Case Rep 2019;2019:rjz241.
[10] Carr NJ, Cecil TD, Mohamed F, Sobin LH, Sugarbaker PH, Gonzalez-Moreno S, et al. A consensus for classi?cation and pathologic reporting of pseudomyxoma peritonei and associated appendiceal neoplasia: the results of the Peritoneal Surface Oncology Group International (PSOGI) Modified Delphi Process. Am J Surg Pathol 2016;40:14–26.Appendiceal mucocele complicated by pseudomyxoma peritonei Clinical case69
[11]Gonzales MS, Shmookler BM, Sugarbaker PH. Appendiceal mucocele, contraindication to laparoscopic appendicectomy. Surg Endosc. 1998 Sep;12(9):1177–9. doi:10.1007/s004649900811. [DOI] [PubMed] [Google Scholar].
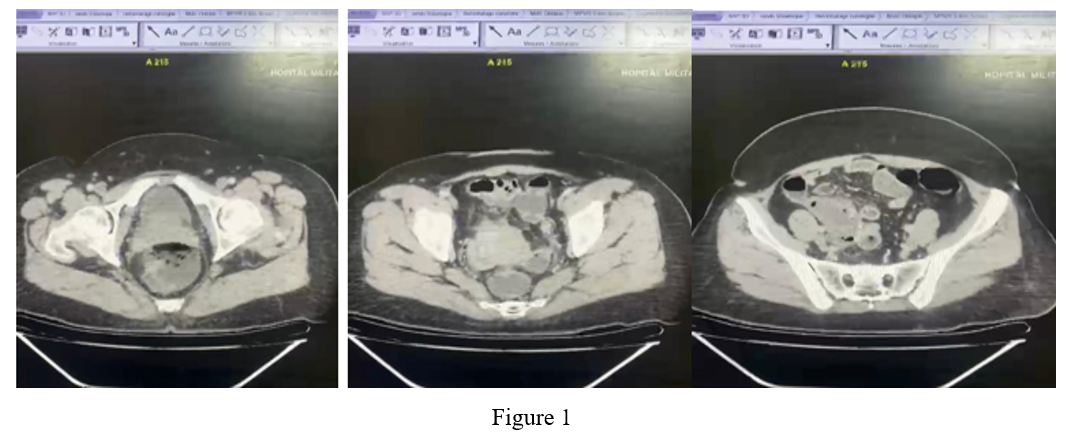
Figure 1
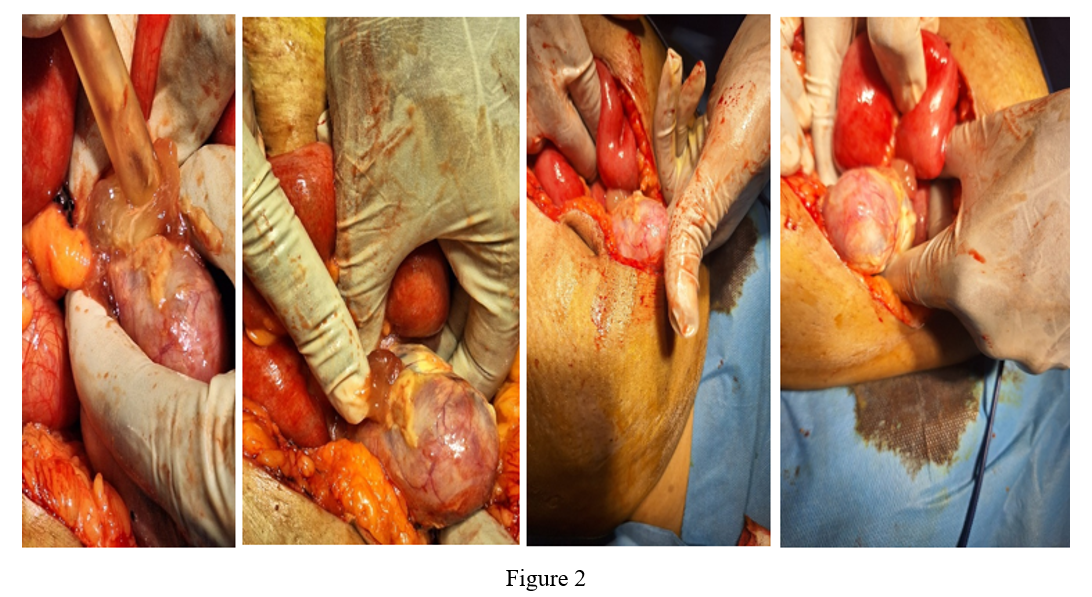
Figure 2